Introduction
Pheochromocytomas occur most frequently in
individuals aged 40–50 years, with a slight predilection in females
(1). The tumors produce
catecholamine, which may lead to severe hypertension and other
systemic disturbances (1).
Anesthetic management of any surgical patient with pheochromocytoma
is challenging and may be difficult to deal with if the tumor has
not been diagnosed. A proportion of patients are diagnosed at the
time of incidental surgery and, in this situation, the mortality
rate is ~80% (2). The serious and
potentially lethal nature of this complication is caused by the
potent effect of the paroxysmal release of catecholamines.
Physicians should be aware of the clinical manifestations and
complications of excess catecholamine and be ready to provide
proper pre-operative management to minimize catecholamine-related
pre-, intra- and post-operative adverse events (3,4).
Written informed consent was obtained from the patient.
Case report
A 54-year-old female (weight, 46 kg; height, 153
cm), was transferred to Tri-Service General Hospital on account of
an unexpected large pancreatic tumor. The clinical history of the
patient included paroxysmal headaches, mildly elevated blood
pressure (BP), diaphoresis and occasional palpitations. The patient
was previously diagnosed with ventricular arrhythmia by
cardiovascular departments in numerous hospitals, without any other
significant findings. The patient was not administered regular
treatment for the headaches or hypertension as the symptoms were
considered insignificant. One month prior to surgery, the patient
underwent a detailed health checkup and an abdominal mass was
identified using abdominal sonography. A large, well-encapsulated
pancreatic tail tumor, measuring 9 cm in length, was observed on
abdominal computed tomography (Fig.
1). The patient was consequently transferred for surgical
intervention.
On admission, mildly elevated BP (138–160/80–90
mmHg) with a heart rate (HR) of 70–90 beats per minute (bpm) was
noted. The ECG revealed a normal sinus rhythm with two ventricular
premature contractions (VPCs). Other laboratory tests showed no
significant abnormalities. An exploratory laparotomy with a
resection of the tumor was scheduled. Thoracic epidural anesthesia
was initially performed without adverse events, followed by general
anesthesia. When the pancreas was approached, no any abnormal
lesions were identified, with the exception of a bulging mass from
the retroperitoneal region. The mass originated from the adrenal
gland and presented as a capsulated, vessel-rich tumor. The
systolic BP surged to 260 mmHg abruptly with fluctuations and the
HR increased to 150 bpm during the manipulation of the tumor. The
concentration of the anesthesia was increased along with an
additional administration of 100 μg intravenous (i.v.) fentanyl.
The fentanyl was ineffective and 5 mg i.v. labetalol was
administered twice. However, the hypertensive crisis remained. The
surgeon made a temporary stay of surgery until the vital signs were
under control and then the tumor was removed.
The BP dropped (75/50 mmHg) once the tumor was
removed. Aggressive fluid replacement and vasopressors were
administered until the patient was hemodynamically stable. The
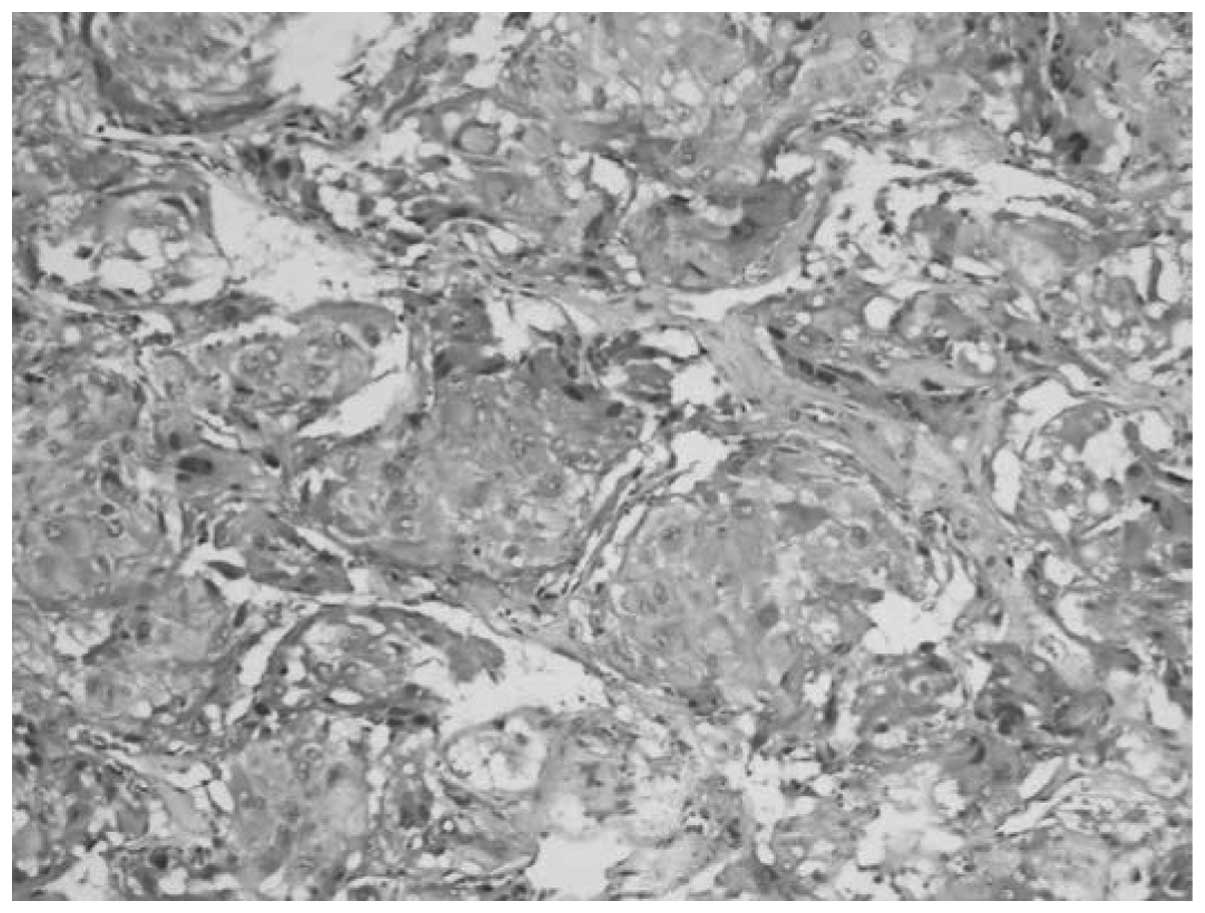
endotracheal tube was then removed. At one day post-surgery, the
patient was completely asymptomatic and no sequelae were
identified. The pathological report confirmed a diagnosis of
pheochromocytoma (Fig. 2) and the
patient was discharged five days later.
Discussion
Although the majority of pancreatic tumors are
malignant, others, including insulinomas, gastrinomas and
vasoactive intestinal peptide-producing tumors (VIPoma), are benign
endocrine tumors (5). The most
common clinical symptoms are gastrointestinal (GI) tract
discomfort, including jaundice, abdominal pain, anorexia and body
weight loss (6). These symptoms
were not observed in the present patient. Adrenal gland tumors are
identified in as many as 10% of autopsies and the majority are
asymptomatic (1).
Pheochromocytoma is one of these adrenal tumors and
may lead to life-threatening events if precautions are not taken,
particularly during surgery. The symptoms and signs that may be
solicited are paroxysmal attacks of sweating, headaches,
hypertension, glucose intolerance and arrhythmia, which may occur
in certain cases (1,7,8). These
symptoms and signs were consistent with the patient in the present
case. Undiagnosed pheochromocytoma may be catastrophic for
physicians, as it accounts for 25–50% of hospital mortalities
during the induction of anesthesia or during surgical procedures
(9). In the present study, upon
reviewing the patient's past history, no GI symptoms were observed,
but the palpitations, headaches, diaphoresis and the image
presentation of this case mimicked a pancreatic tail tumor
(Fig. 1). Misdiagnoses may occur
easily, resulting in adverse events. The present case provides
first-line clinical physicians with an additional option to
consider as a diagnosis when dealing with a suspicious pancreatic
tumor. Performing the appropriate history and physical examinations
is always the most important diagnostic action. If the initial
diagnosis is not consistent with these previously mentioned
subjective complaints, a more detailed history or comprehensive
examination is required. For anesthesiologists and surgeons who
encounter an unexpected hypertensive crisis during abdominal tumor
surgery, undiagnosed pheochromocytoma should always be considered
as an option.
References
|
1
|
Lenders JW, Eisenhofer G, Mannelli M and
Pacak K: Phaeochromocytoma. Lancet. 366:665–675. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Myklejord DJ: Undiagnosed
pheochromocytoma: the anesthesiologist nightmare. Clin Med Res.
2:59–62. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ahmed A: Perioperative management of
pheochromocytoma: anaesthetic implications. J Pak Med Assoc.
57:140–146. 2007.PubMed/NCBI
|
|
4
|
Pacak K: Preoperative management of the
pheochromocytoma patient. J Clin Endocrinol Metab. 92:4069–4079.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Howard TJ, Stabile BE, Zinner MJ, Chang S,
Bhagavan BS and Passaro E Jr: Anatomic distribution of pancreatic
endocrine tumors. Am J Surg. 159:258–264. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Porta M, Fabregat X, Malats N, et al:
Exocrine pancreatic cancer: symptoms at presentation and their
relation to tumour site and stage. Clin Transl Oncol. 7:189–197.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pauker SG and Kopelman RI: Interpreting
hoofbeats: can Bayes help clear the haze? N Engl J Med.
327:1009–1013. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Witteles RM, Kaplan EL and Roizen MF:
Sensitivity of diagnostic and localization tests for
pheochromocytoma in clinical practice. Arch Intern Med.
160:2521–2524. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sutton MG, Sheps SG and Lie JT: Prevalence
of clinically unsuspected pheochromocytoma: Review of a 50-year
autopsy series. Mayo Clin Proc. 56:354–360. 1981.
|