Introduction
Renal cell carcinoma (RCC) is the seventh most
common cancer in males and the ninth most common cancer in females,
and accounts for ~2% of all malignant diseases in adults (1). RCC continues to be a devastating
cancer and the worldwide incidence and mortality rates are rising
at a rate of 2–3% per decade (2).
Furthermore, the initial clinical course of RCC is asymptomatic,
resulting in 25–30% of patients presenting with metastatic disease
at the time of diagnosis (2). To
date, the definite etiology of RCC remains unclear. A number of
studies have shown that active and/or passive smoking (3), moderate and/or heavy alcohol
consumption (4), obesity (5,6) and
hypertension (7) are established
risk factors that play key roles in the development of RCC.
However, as they do not entirely explain the etiology, there may be
other risk factors that are involved. With developments in
molecular biology, researchers have investigated whether genetic
factors are involved in RCC development.
Vascular endothelial growth factor (VEGF) is a
potent endothelial cell mitogen that plays a key role in
angiogenesis (8,9). Compelling evidence from meta-analyses
has indicated that VEGF gene polymorphisms are associated with the
risk of various diseases, including gastric cancer (10), pre-eclampsia (11), cardiovascular disease (12) and amyotrophic lateral sclerosis
(13). The VEGF receptors, VEGFR1,
VEGFR2 and VEGFR3, have significant roles in the signaling pathways
that are involved in RCC pathogenesis, and mutations in VEGFRs may
affect the signaling networks (14). Therefore, VEGF gene polymorphisms
may be associated with RCC. In 2002, Abe et al(15) investigated the association between
single nucleotide polymorphisms in the 3′-untranslated region (UTR)
of the VEGF gene and RCC in the Japanese population, and indicated
that the C702T, C936T and G1612A polymorphisms in the 3′-UTR of the
VEGF gene are not associated with the risk of RCC. However, their
results showed significant ethnic differences in the frequencies of
the C702T and G1612A alleles (15).
Certain studies have also been performed to detect
the association between VEGF gene polymorphisms and RCC, and the
results are varied. The present systematic review and meta-analysis
aims to present the genetic knowledge on the VEGF gene
polymorphisms and RCC risk in humans based on the published
evidence.
Materials and methods
Literature selection
The proposed Preferred Reporting Items for
Systematic reviews and Meta-Analyses (PRISMA) (16) statement was followed to report the
present meta-analysis. Initially, the published studies that tested
the association between VEGF gene polymorphisms and RCC were
identified by searching PubMed for studies that were published
between January 2000 and December 2012. The search terms that were
used were ‘renal cell’ and ‘carcinoma’ or ‘cancer’ and ‘vascular
endothelial growth factor’ or ‘VEGF’ and ‘polymorphism’, ‘mutation’
or ‘variation’, without restrictions. In addition, the reference
lists of retrieved papers and recent reviews were also
examined.
Study selection
Any study that matched the following criteria was
included: i) A case-control study design; ii) an association
between VEGF gene polymorphisms and RCC in humans; iii) RCC
confirmed by the accepted diagnostic criteria; iv) inclusion of the
odds ratio (OR) and the corresponding 95% confidence intervals
(CIs), or the number of events that may be used to calculate
them.
To evaluate the eligibility of all the studies
retrieved from the databases on the basis of the predetermined
selection criteria, two independent investigators were used.
Disagreements were resolved by discussion.
Data extraction
The two independent reviewers extracted the
following data: gene polymorphisms, first author’s last name, year
of publication, site of origin, source of controls, matching
criteria, number of cases and controls, number of different
genotypes in cases and controls, Hardy-Weinberg equilibrium (HWE)
and minor allele frequency in controls. Any disagreements were
resolved by consensus.
Data analysis
The articles that met the inclusion criteria were
identified and classified according to the gene polymorphisms that
they described. Subsequent to categorizing the data, a descriptive
analysis of the data that were unsuitable for conducting the
meta-analysis was performed. The data that were suitable for
pooling were used in the meta-analysis.
A pooled OR and 95% CI was computed for the risk
allele using RevMan 5.1 (Nordic Cochrane Centre, Copenhagen,
Denmark) to generate forest plots, in order to determine whether a
statistical association was present between the case and control
groups and to assess the heterogeneity of the included studies. The
HWE was tested by a χ2 test at a significance level of
P<0.05. Heterogeneity was quantifiably evaluated using the
χ2-based Cochran’s Q statistic (17) and the I2 statistic
(18). The I2 statistic
yields results ranging between 0 and 100% (0–25%, no heterogeneity;
25–50%, moderate heterogeneity; 50–75%, large heterogeneity; and
75–100%, extreme heterogeneity). If heterogeneity was present, the
random effects model was used, otherwise, the fixed effects model
was used. A sensitivity analysis was conducted by switching the
effects models. If possible, potential publication bias was
assessed by a visual inspection of the funnel plots.
Results
Identification of eligible studies
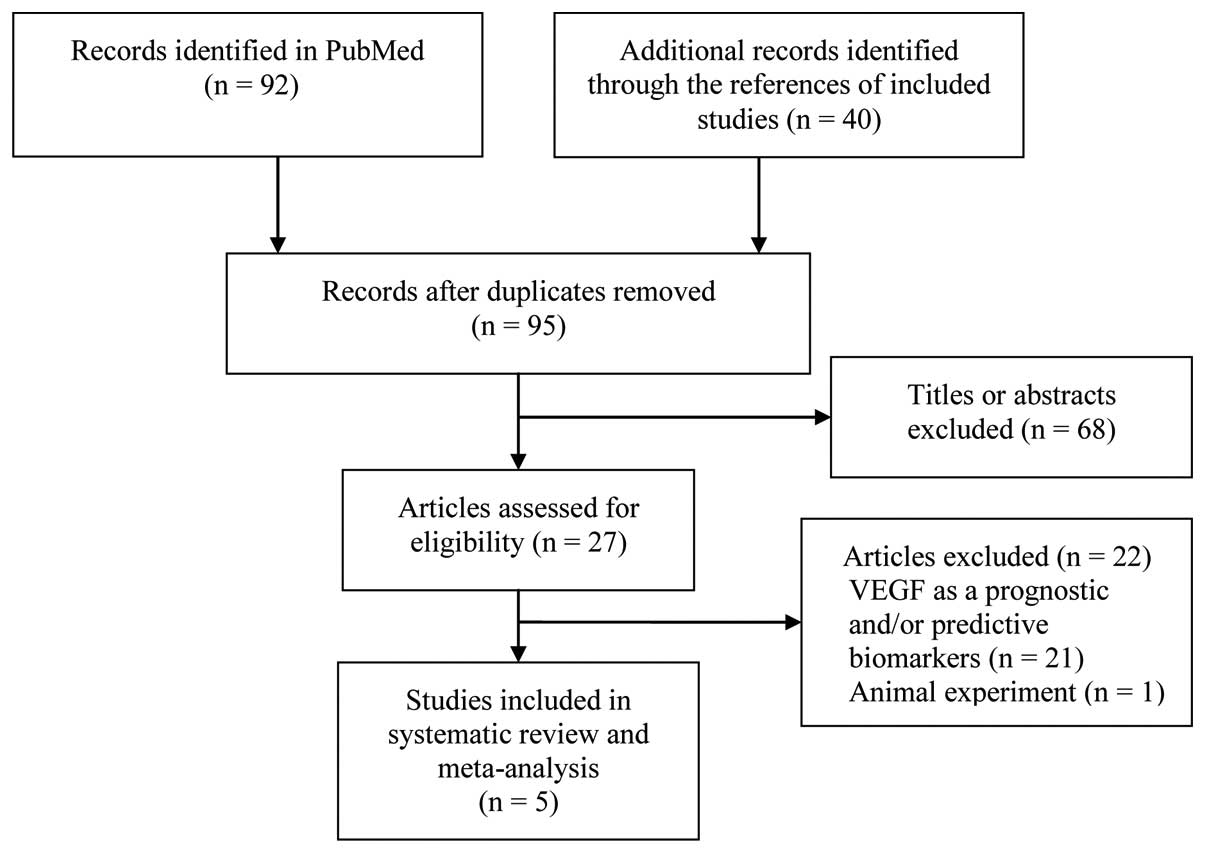
Of the initial 132 references, five case-control
studies (15,19–22)
were identified, including eight polymorphisms. A flow chart
showing the study selection process is presented in Fig. 1.
Characteristics of studies
The detailed characteristics of the included studies
are summarized in Tables I and
II. All studies were published in
English and the sample sizes ranged between 51 and 343
participants. The controls were all healthy individuals and were
matched for age and gender. The genotypes of two studies (19,20)
were analyzed using PCR (polymerase chain reaction), two (15,21)
were analyzed by PCR-RFLP (restriction fragment length
polymorphism) and one (22) by a
TaqMan assay. The genotype distributions in the controls of all the
studies were in accordance with the HWE.
 | Table IBaseline characteristics of the
included studies. |
Table I
Baseline characteristics of the
included studies.
| | Sample size, n | | |
|---|
| |
| | |
|---|
| First author, year
(ref) | Ethnicity | Case | Control | Gene
polymorphism | Genotyping
method |
|---|
| Abe et al,
2002 (15) | Asian | 145 | 145 | 936C/T (rs3025039),
1612G/A (rs10434), 702C/T | PCR-RFLP |
| Ricketts et
al, 2009 (19) | Caucasian | 343 | 321 | −1154G/A
(rs1570360) | PCR |
| Bruyère et
al, 2010 (20) | Caucasian | 51 | 202 | 936C/T (rs3025039),
−1154G/A (rs1570360),−2549I/D, −460T/C (rs833061), 405G/C
(rs2010963) | PCR |
| Ajaz et al,
2011 (21) | Asian | 143 | 106 | −2578C/A (rs699947)
936C/T (rs3025039) | PCR-RFLP |
| Sáenz-López et
al, 2013 (22) | Caucasian | 216 | 216 | 936C/T (rs3025039),
−460T/C (rs833061), −2578C/A (rs699947) | TaqMan |
| Table IIGenotype distribution of all the
included studies. |
Table II
Genotype distribution of all the
included studies.
| A, 936C/T
(rs3025039) |
|---|
|
|---|
| | Case | | Control | |
|---|
| |
| |
| |
|---|
| Reference | Location | CC | TT | CT | Source of
control | CC | TT | CT | P-value for
HWE |
|---|
| Abe 2002 | 3′UTR | 97 | 41 | 7 | HC | 90 | 52 | 3 | 0.146 |
| Bruyère 2010 | 3′UTR | 29 | 17 | 1 | HC | 141 | 53 | 2 | 0.124 |
| Sáenz-López
2013 | 3′UTR | 156 | 57 | 2 | HC | 200 | 73 | 7 | 0.912 |
|
| B, 1612G/A
(rs10434) |
|
| | Case | | Control | |
| |
| |
| |
| Reference | Location | GG | GA | AA | Source of
control | GG | GA | AA | P-value for
HWE |
|
| Abe 2002 | 3′UTR | 113 | 31 | 1 | HC | 109 | 33 | 3 | 0.788 |
|
| C, 702C/T |
|
| | Case | | Control | |
| |
| |
| |
| Reference | Location | CC | CT | TT | Source of
control | CC | CT | TT | P-value for
HWE |
|
| Abe 2002 | 3′UTR | 145 | 0 | 0 | HC | 145 | 0 | 0 | / |
|
| D, −1154G/A
(rs1570360) |
|
| | Case | | Control | |
| |
| |
| |
| Reference | Location | GG | GA | AA | Source of
control | GG | GA | AA | P-value for
HWE |
|
| Ricketts 2009 | PR | 134 | 143 | 47 | HC | 146 | 130 | 38 | 0.281 |
| Bruyère 2010 | PR | 27 | 17 | 5 | HC | 94 | 83 | 25 | 0.322 |
|
| E, −2549I/D. |
|
| | Case | | Control | |
| |
| |
| |
| Reference | Location | II | ID | DD | Source of
control | II | ID | DD | P-value for
HWE |
|
| Bruyère 2010 | PR | 5 | 28 | 18 | HC | 45 | 108 | 49 | 0.322 |
|
| F, −460T/C
(rs833061). |
|
| | Case | | Control | |
| |
| |
| |
| Reference | Location | TT | TC | CC | Source of
control | TT | TC | CC | P-value for
HWE |
|
| Bruyère 2010 | PR | 19 | 29 | 1 | HC | 47 | 109 | 46 | 0.260 |
| Sáenz-López
2013 | PR | 56 | 111 | 49 | HC | 77 | 138 | 58 | 0.793 |
|
| G, −405G/C
(rs2010963). |
|
| | Case | | Control | |
| |
| |
| |
| Reference | Location | GG | GC | CC | Source of
control | GG | GC | CC | P-value for
HWE |
|
| Bruyère 2010 | 5′UTR | 15 | 25 | 8 | HC | 86 | 92 | 20 | 0.522 |
| Sáenz-López
2013 | 5′UTR | 101 | 93 | 20 | HC | 129 | 118 | 32 | 0.528 |
|
| H, −2578C/A
(rs699947). |
|
| | Case | | Control | |
| |
| |
| |
| Reference | Location | CC | CA | AA | Source of
control | CC | CA | AA | P-value for
HWE |
|
| Ajaz 2011 | PR | 30 | 81 | 32 | HC | 44 | 41 | 21 | 0.053 |
| Sáenz-López
2013 | PR | 54 | 114 | 48 | HC | 77 | 142 | 53 | 0.388 |
Abe et al(15) studied three polymorphisms, 936C/T
(rs3025039), 1612G/A (rs10434) and 702C/T. The study by Ricketts
et al(19) was concerned
with one polymorphism, −1154G/A (rs1570360). Bruyère et
al(20) investigated five
polymorphisms, 936C/T (rs3025039), −1154G/A (rs1570360), −2549I/D,
−460T/C (rs833061) and 405G/C (rs2010963). Ajaz et
al(21) surveyed two
polymorphisms, −2578C/A (rs699947) and 936C/T (rs3025039).
Sáenz-López et al(22)
inquired about three polymorphisms, 936C/T (rs3025039), −460T/C
(rs833061) and −2578C/A (rs699947).
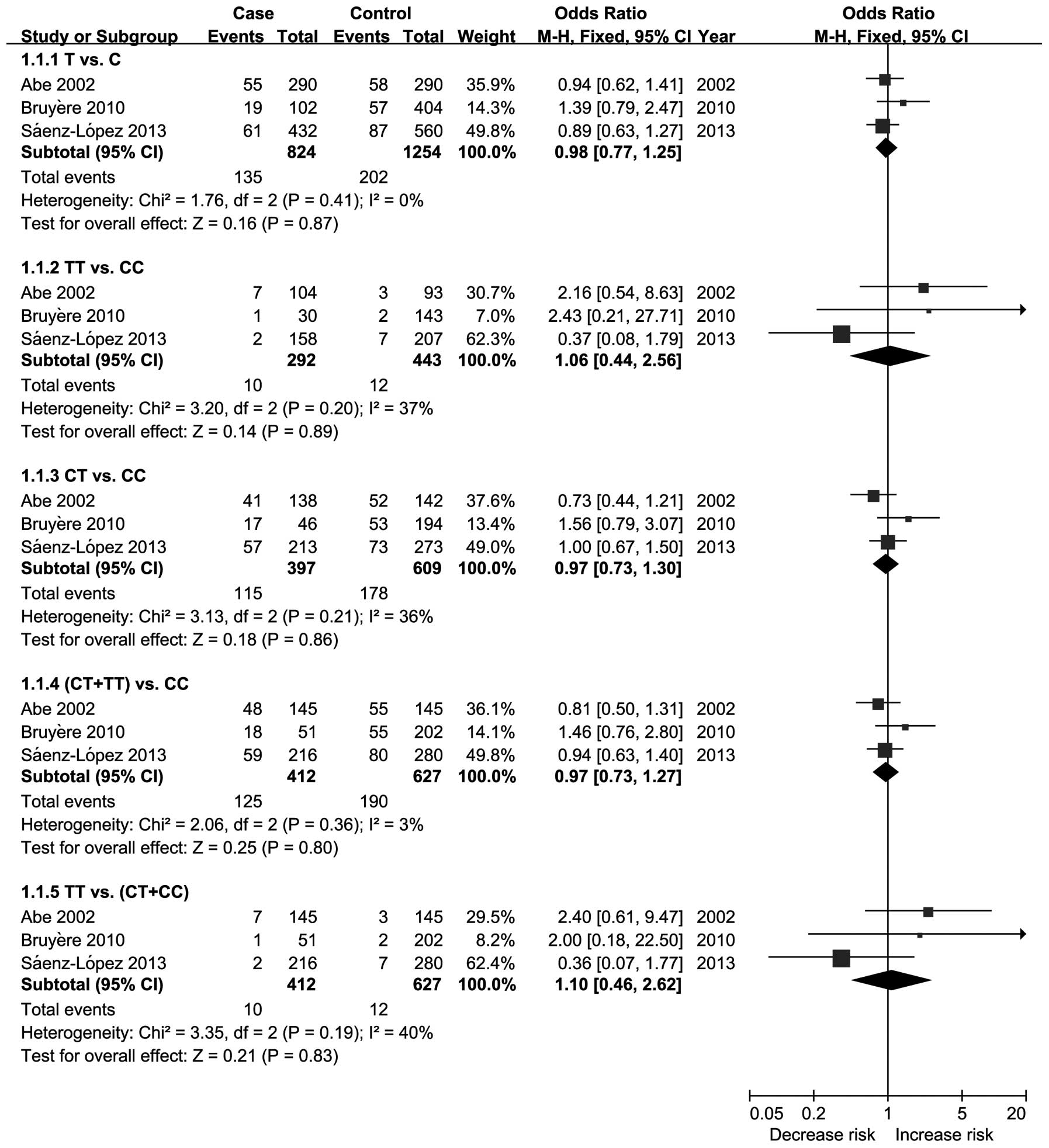
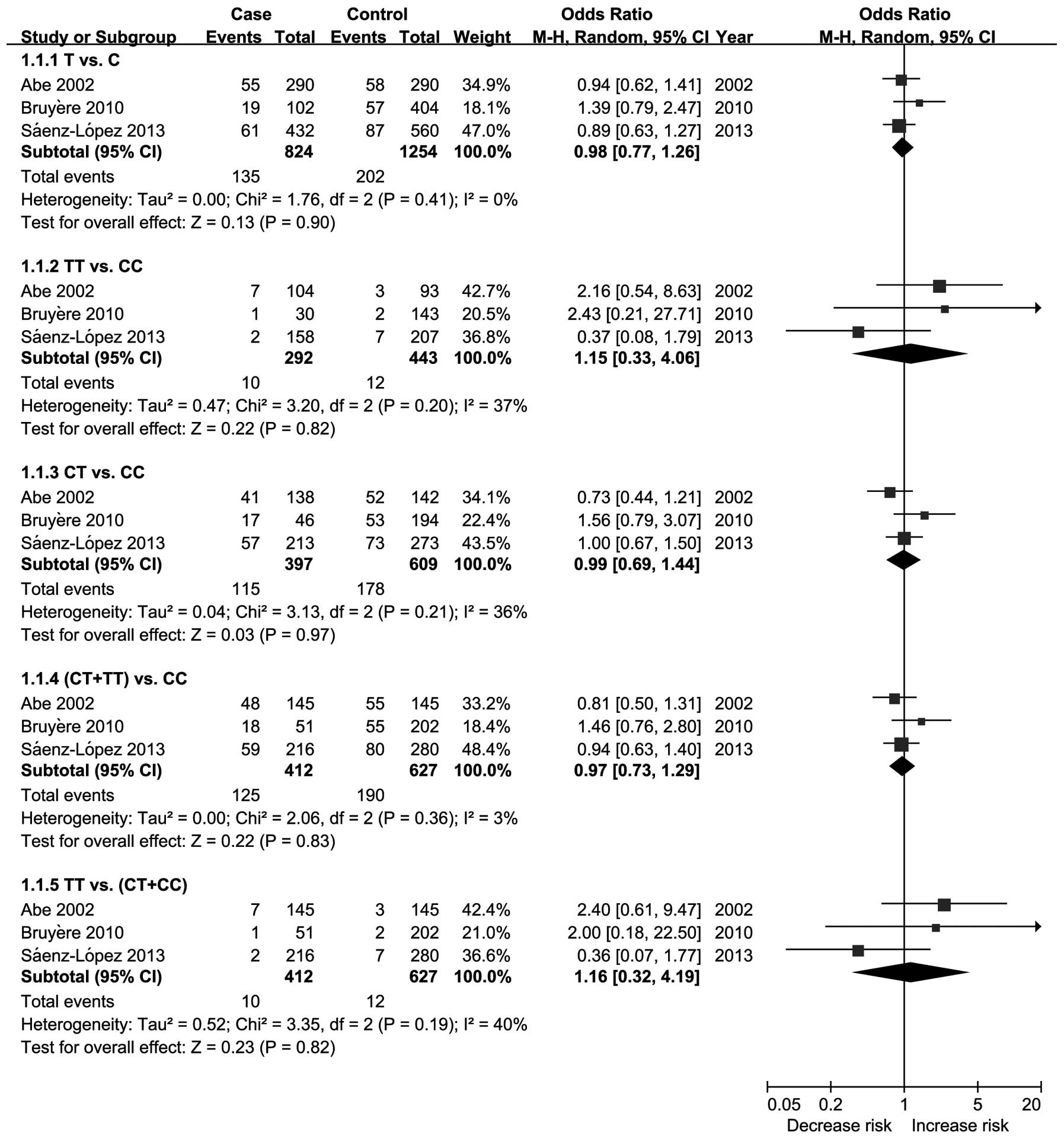
936C/T polymorphism and RCC
A total of four studies (15,20–22)
investigated the 936C/T polymorphism in RCC. Of these studies,
three (15,20,22)
provided enough data to be combined. Figs. 2 and 3 show the results of the meta-analysis
based on the fixed effects and random effects models, respectively.
The results indicate that the VEGF gene 936C/T polymorphism was not
associated with the risk of RCC.
Ajaz et al(21) did not report the number of each
genotype distribution of the VEGF 936C/T polymorphism. They
reported that the 936C/T polymorphism lacked an association with
RCC (OR, 1.5; 95% CI, 0.7–3.3; P=0.36).
1612G/A polymorphism and RCC
Only Abe et al(15) investigated the VEGF gene 1612G/A
polymorphism and RCC. The results showed no association between the
1612G/A polymorphism and a risk of RCC [A vs. G (OR, 0.83; 95% CI,
0.50–1.36; P=0.45); AA vs. GG (OR, 0.32; 95% CI, 0.03–3.14;
P=0.33); AG vs. GG (OR, 0.91; 95% CI, 0.52–1.58; P=0.73); AA+AG vs.
GG (OR, 0.86; 95% CI, 0.50–1.48; P, 0.58); AA vs. GG+GA; OR, 0.33;
95% CI, 0.03–3.20; P=0.34)].
702C/T polymorphism and RCC
Abe et al(15) tested the VEGF gene 702C/T
polymorphism and RCC. The results showed that there was no
polymorphism in 702C/T in either the case or control groups (data
shown in Table II).
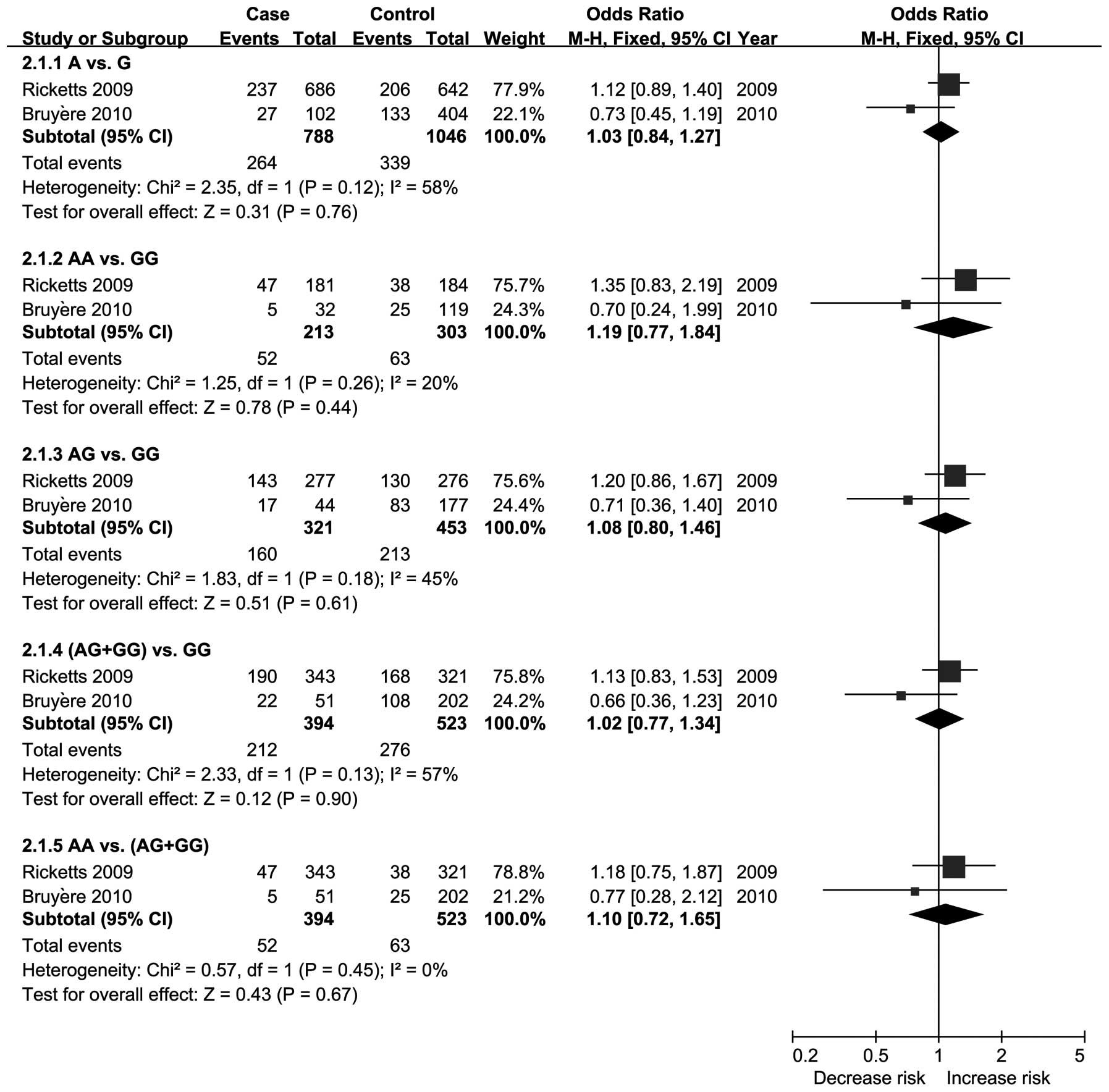
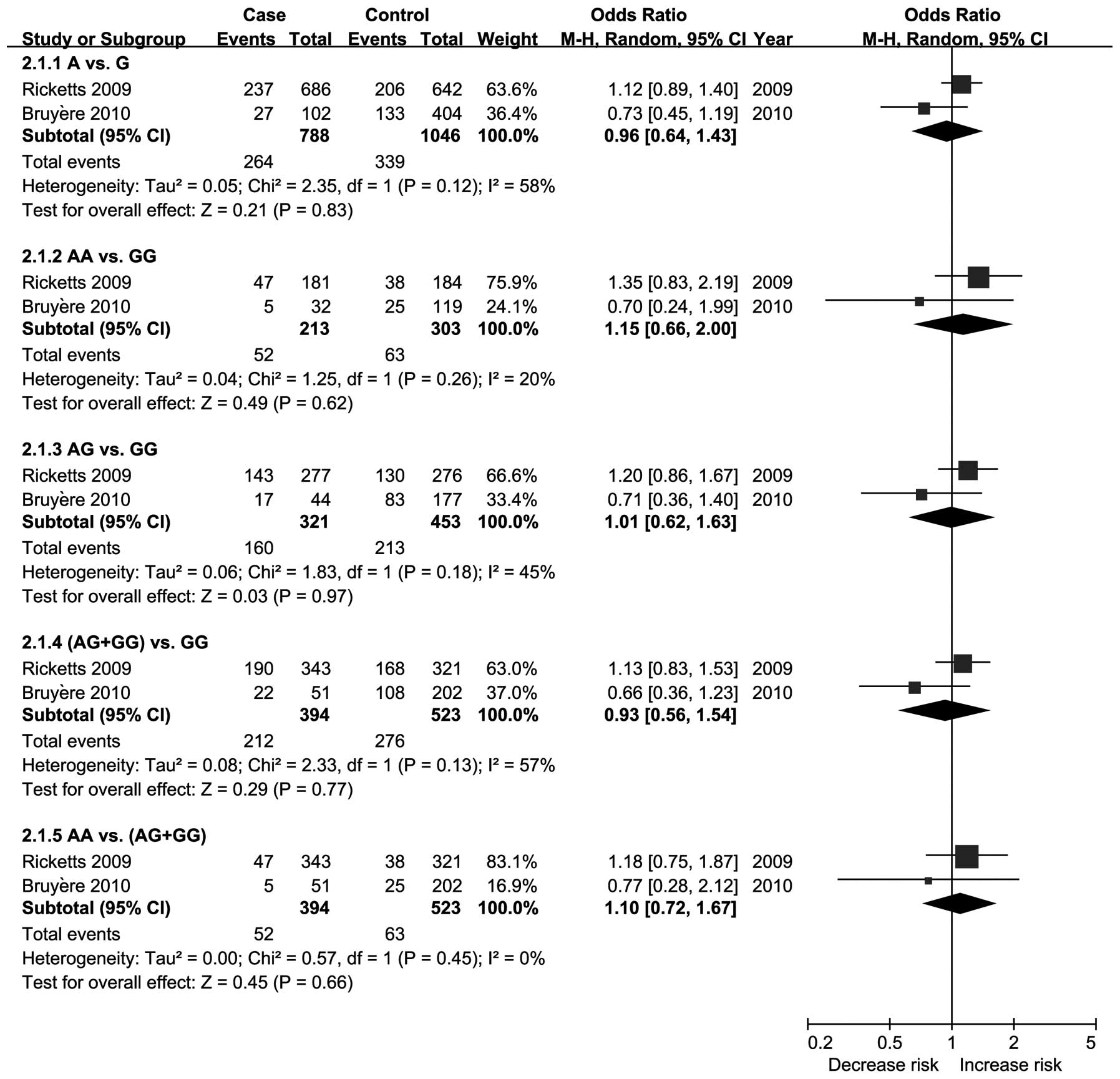
−1154G/A polymorphism and RCC
A total of two studies (19,20)
investigated the −1154G/A polymorphism and RCC. Figs. 4 and 5 show the results of the meta-analysis
based on the fixed effects and random effects models, respectively.
The results indicate that the VEGF gene −1154G/A polymorphism was
not associated with the risk of RCC.
−2549I/D polymorphism and RCC
Bruyère et al(20) analyzed the VEGF gene −2549I/D
polymorphism and RCC. The results showed that the genotype at the
−2549 polymorphism exhibited a non-significant trend for an
increased risk of RCC. However, the D allele was associated with a
significantly increased risk [D vs. I (OR, 1.62, 95% CI, 1.04–2.53;
P=0.03); DD vs. II (OR, 3.31; 95% CI, 1.13–9.64, P=0.03); DI vs. II
(OR, 2.33; 95% CI, 0.85–6.43; P=0.10); DI+DD vs. II (OR, 2.64; 95%
CI, 0.99–7.03, P=0.05); DD vs. II+ID (OR, 1.70; 95% CI, 0.88–3.29;
P=0.11)].
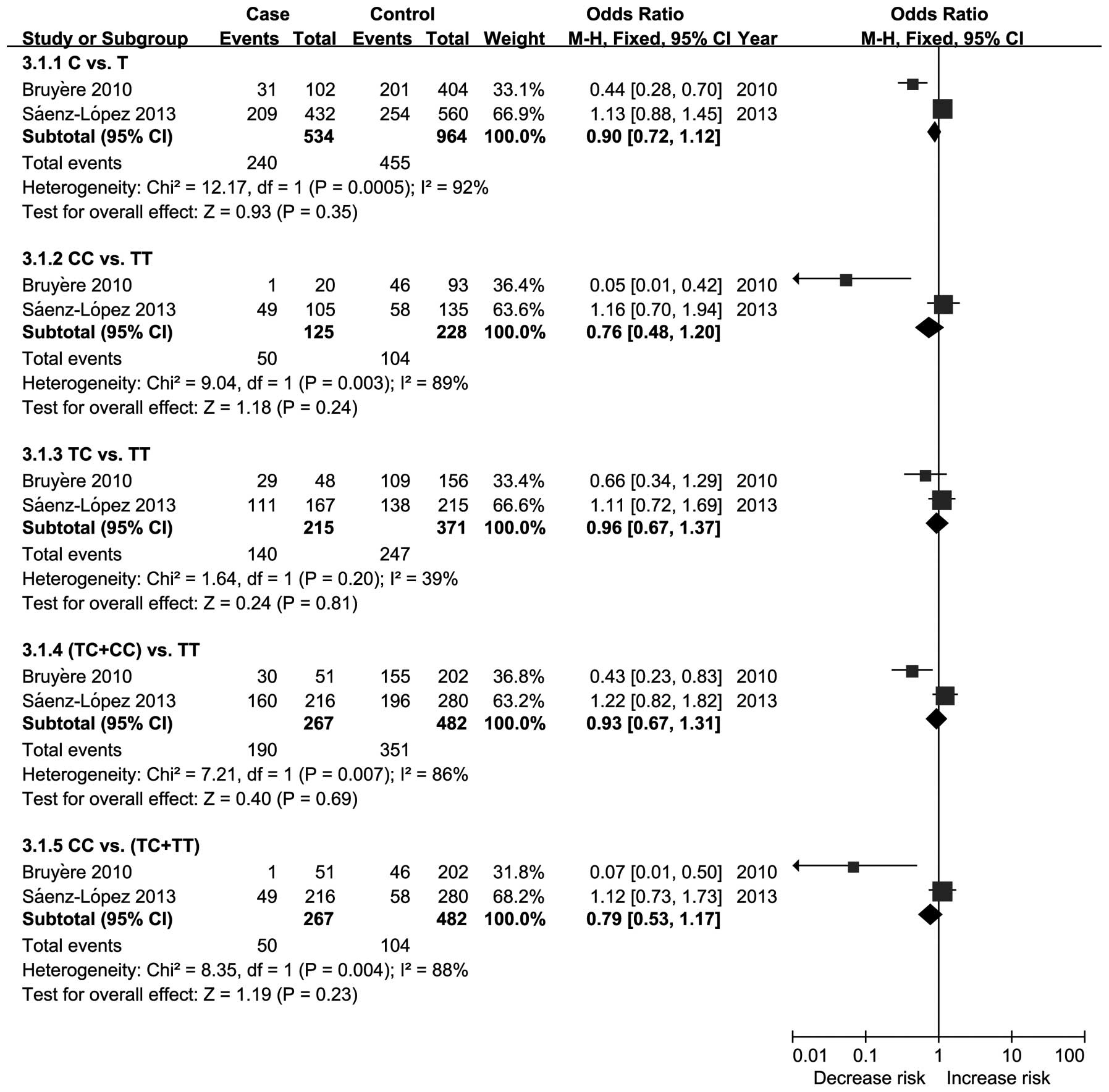
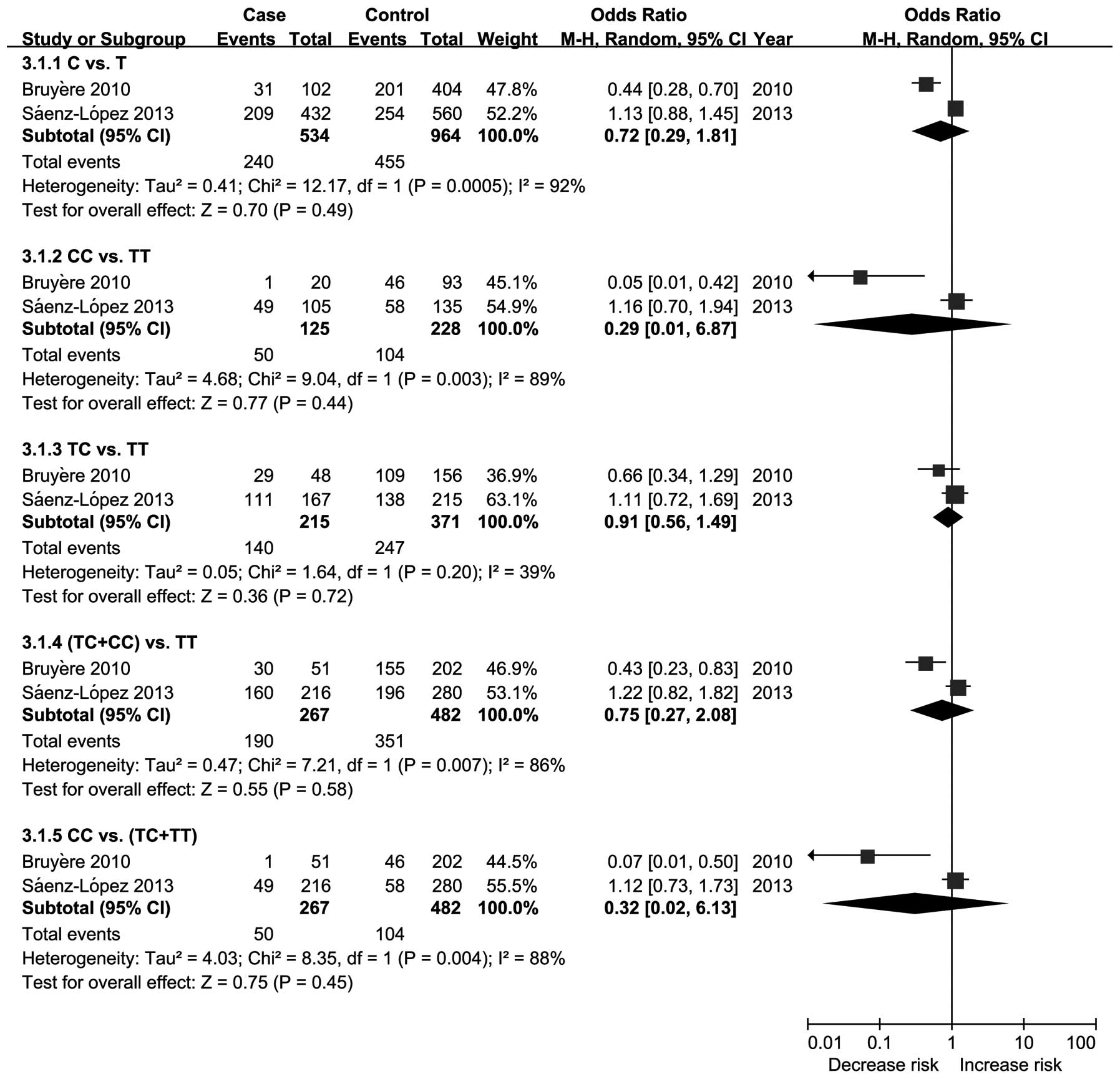
−460T/C polymorphism and RCC
A total of two studies (20,22)
investigated the −460T/C polymorphism and RCC. Figs. 6 and 7 show the results of the meta-analysis
based on the fixed effects and random effects models, respectively.
The results indicated that the VEGF gene −460T/C polymorphism was
not associated with the risk of RCC.
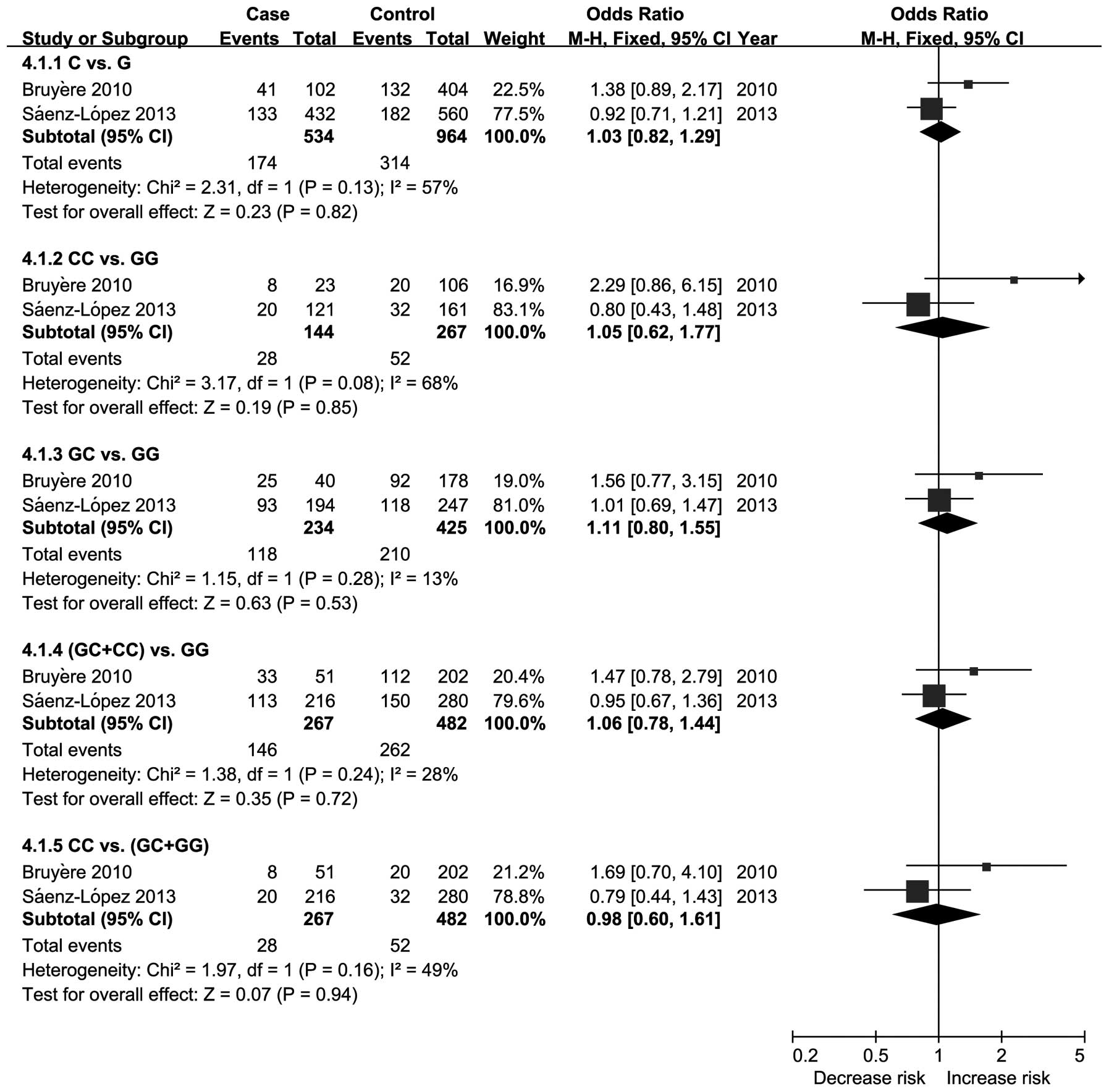
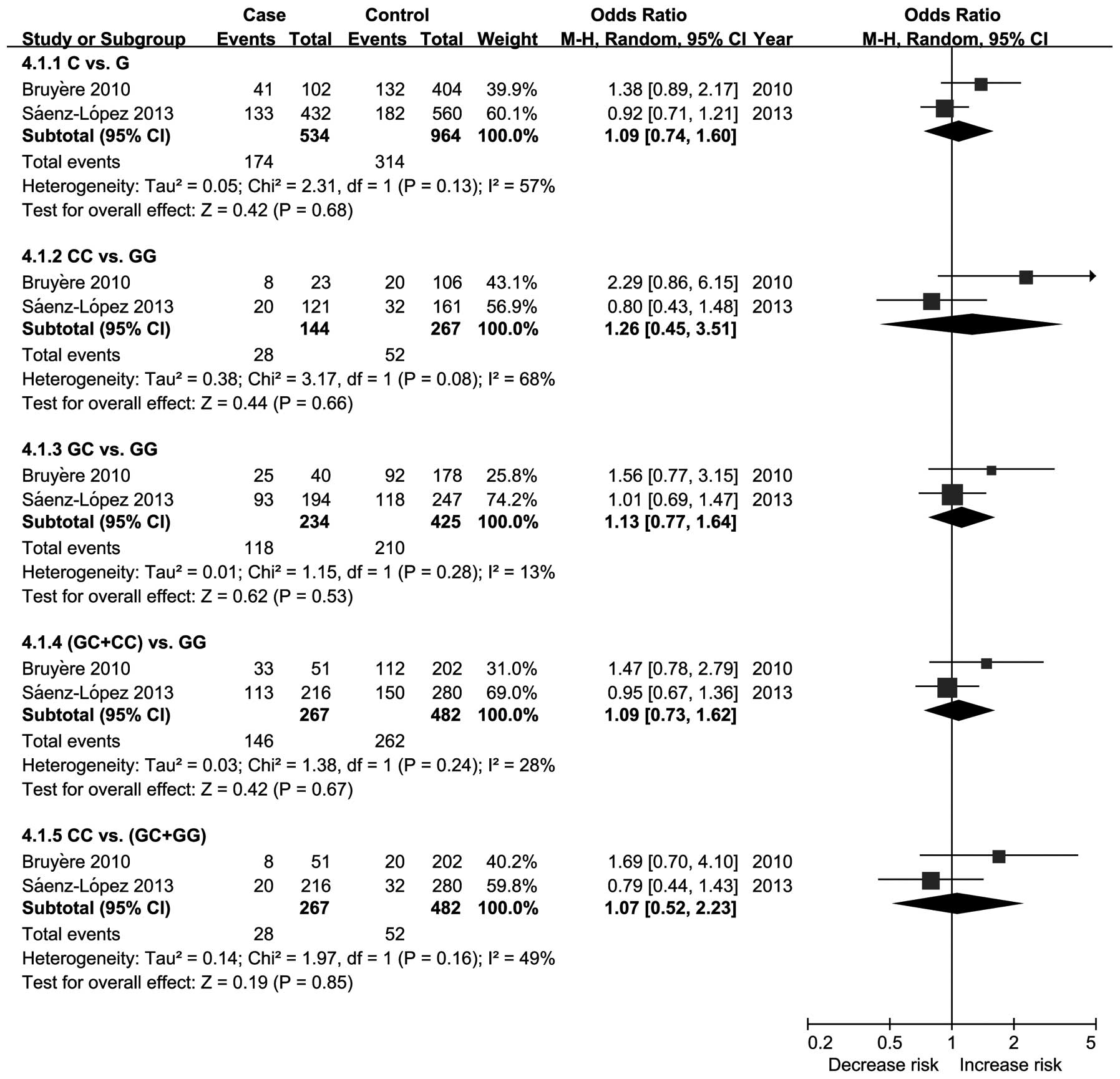
405G/C polymorphism and RCC
A total of two studies (20,22)
investigated the 405G/C polymorphism and RCC. Figs. 8 and 9 show the results of the meta-analysis
based on the fixed effects and random effects models, respectively.
The results indicate that the VEGF gene 405G/C polymorphism
exhibited a non-significant trend for an increased risk of RCC.
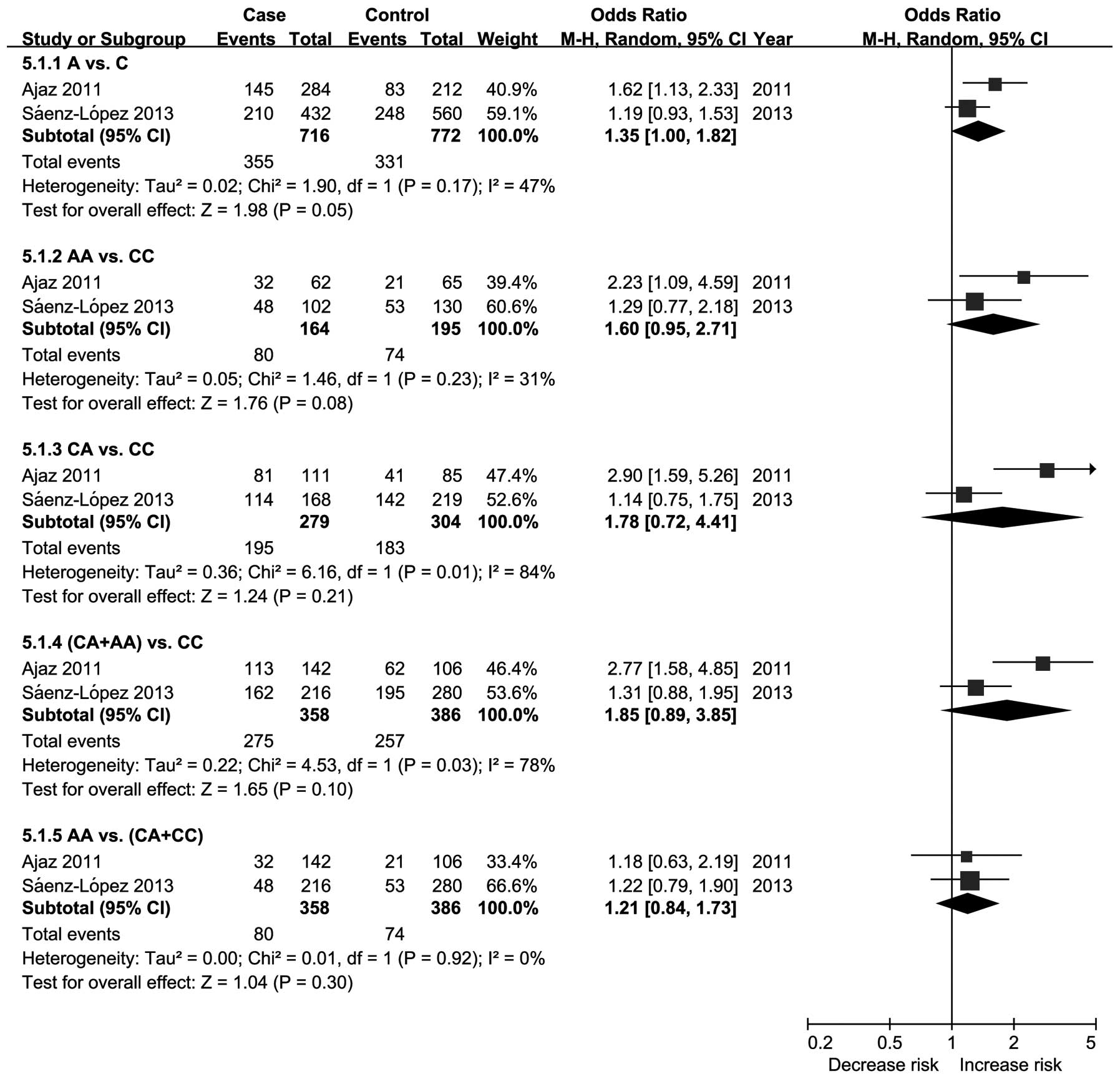
−2578C/A polymorphism and RCC
A total of two studies (21,22)
investigated the −2578C/A polymorphism and RCC. Based on the random
effects model, the results show that the genotype at the −2578C/A
polymorphism exhibited a non-significant trend for a significantly
increased risk of RCC, but that the A allele was associated with an
increased risk of RCC (Fig. 10).
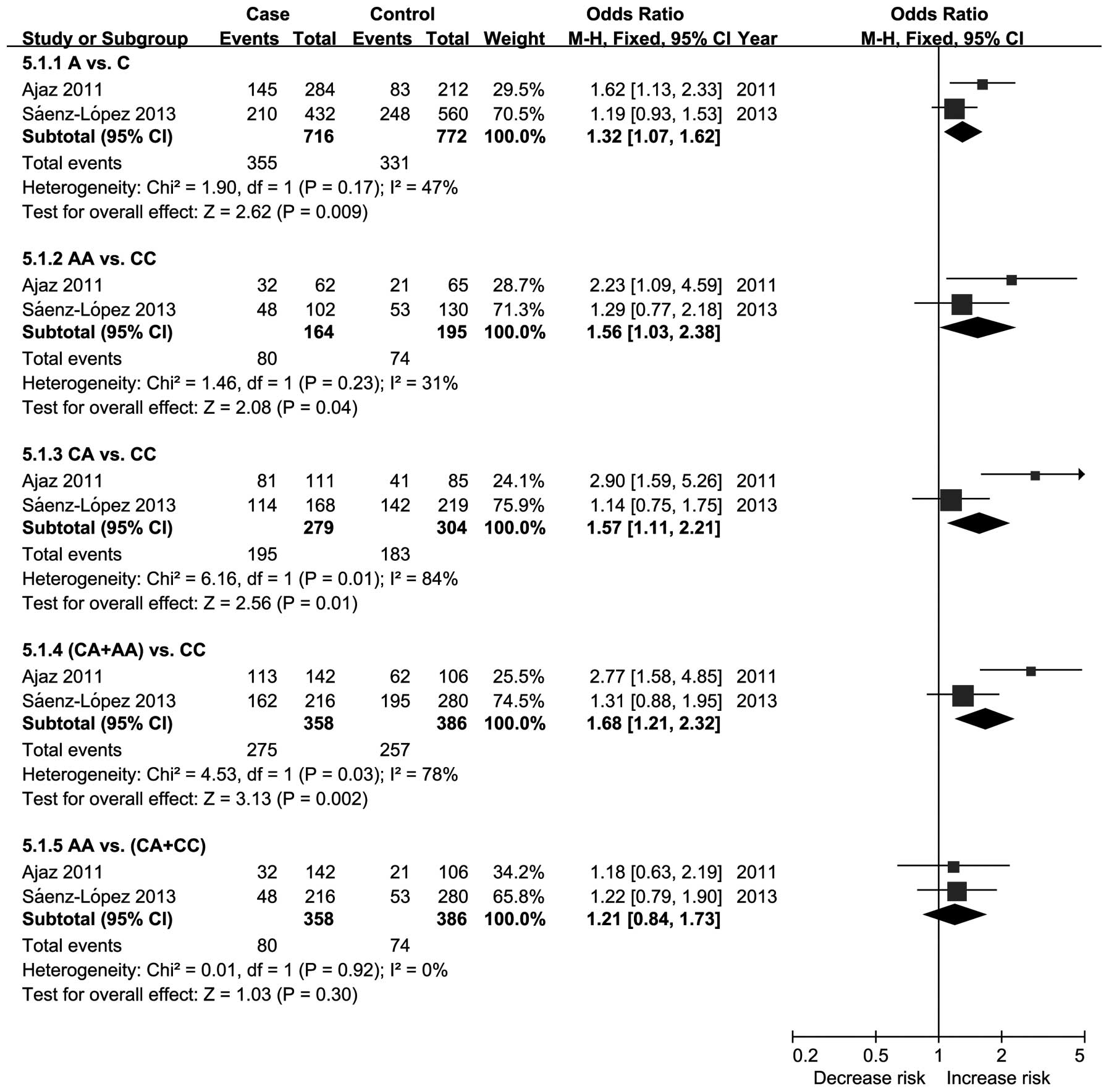
However, when switched to the fixed effects model, the results show
that the genotype at the −2578C/A polymorphism exhibited a
significant trend for an increased risk of RCC (Fig. 11).
Discussion
The human VEGF gene is localized in chromosome
6p21.3 (23) and comprises a 14-kb
coding region organized in eight exons, which are separated by
seven introns (24). Experiments
have shown that increased VEGF expression is associated with tumor
growth and metastasis, and the inhibition of VEGF signaling has
been shown to suppress tumor-induced angiogenesis and tumor growth
(25). The VEGF gene includes at
least three polymorphisms that are relatively common and may affect
VEGF expression. The insertion/deletion polymorphism (I/D) at the
−2549 position of the promoter region and the −634G/C (rs2010963)
polymorphism located in the 5′-UTR have been considered to be
associated with increased VEGF expression (26,27).
The 936C/T (rs3025039) polymorphism located in the 3′-UTR is
associated with substantially increased serum VEGF levels (28,29).
However, there are at least 30 single nucleotide polymorphisms in
the VEGF gene that have been described (30). In addition, the VEGF family includes
five VEGF ligands (VEGF-A, -B, -C and -D and platelet-derived
growth factor), and three tyrosine kinase receptors (VEGFR-1, -2
and -3), which are involved in signaling pathways for angiogenesis
and/or lymphangiogenesis (31).
Therefore, an improved understanding of these markers is expected
to reveal significant information with regard to the outcome and
therapeutic efficacy in RCC. The present systematic review and
meta-analysis was performed to investigate whether these three
polymorphisms, and others, are associated with RCC.
This systematic review and meta-analysis addresses
the association between eight VEGF gene polymorphisms and RCC
susceptibility. Data from published studies were combined to
evaluate the genetic associations between VEGF and the studied
polymorphisms of the VEGF gene, namely, the 936C/T, 1612G/A,
702C/T, −1154G/A, −2549I/D, −460T/C, 405G/C and −2578C/A
polymorphisms. No associations were identified between the 936C/T,
1612G/A, −1154G/A, −2549I/D, −460T/C and 405G/C polymorphisms and
RCC. However, the results did reveal a significant association
between the D allele of the −2549I/D polymorphism and RCC. The
−2578C/A polymorphism may be associated with RCC. For the 702C/T
polymorphism and RCC, the results showed that there was no
polymorphism in 702C/T in either the case group or the control
group. The results indicate that the −2578C/A polymorphism may be a
risk factor for RCC susceptibility.
The present systematic review and meta-analysis has
the following strengths. Firstly, the study is methodologically
rigorous. The Q and I2 statistics were checked; the
I2 statistic is more stable and is not affected as much
by sample size (18). In the pooled
analyses, fixed and random effects models were used to ensure the
robustness of the estimates. Secondly, analysis comparisons of all
five genetic models were performed, which provided enough
information to detect the association. Finally, the literature
search was extensive, locating all studies that had been published
with regard to VEGF gene polymorphisms and RCC. Eight polymorphisms
were identified, which is essential for the integrity of a
comprehensive understanding of the correlation between VEGF gene
polymorphisms and RCC.
This systematic review and meta-analysis has certain
implications. Firstly, there was no polymorphism in 702C/T in
either the RCC group or the control group. Therefore, further
studies have not been required to investigate this polymorphism and
RCC. In fact, since the study by Abe et al(15) in 2002, no subsequent studies have
investigated the VEGF gene 702C/T polymorphism and RCC. Secondly,
the −2578C/A polymorphism was associated with RCC risk in the fixed
effects model, but heterogeneity was present and the credibility of
the result was undermined. However, one of the included studies
revealed an increased trend in the RCC risk and another indicated a
statistically significant increased trend. Since the number and
sample sizes of the two included studies were small, further
studies that focus on this polymorphism are required. Thirdly, the
result from the VEGF gene −2549I/D polymorphism exhibited a
non-significant trend for an increased RCC risk in the DD vs. II,
DI vs. II, DI+DD vs. II and DD vs. II+ID genetic models; however,
the D allele was significantly associated with an increased RCC
risk (OR, 1.62; 95% CI, 1.04–2.53; P=0.03). Only one study
(20) detected the −2549I/D
polymorphism and only two genetic models (D vs. I and DD vs. II)
showed a significant difference. Further studies with regard to
this polymorphism and RCC are required. Fourthly, there was no
association between the 936C/T, 1612G/A, −1154G/A, −2549I/D,
−460T/C and 405G/C polymorphisms and the risk of RCC, based on the
fixed effects or random effects models. The meta-analysis included
only three studies and further analyses are required to investigate
these polymorphisms. Finally, in gene-targeted therapy (32), an assessment of the effectiveness of
VEGF antibodies, including bevacizumab (33) and new VEGF inhibitor drugs for RCC
are required.
However, the present results should be interpreted
with caution due to the limitations apparent in this systematic
review and meta-analysis. Firstly, only published studies were
included in the study, therefore, publication bias may have
occurred. Secondly, the number of studies and the sample sizes of
each polymorphism were small, therefore, the statistical power is
affected. Thirdly, the subjects in the present meta-analysis may be
regarded as heterogeneous, as indicated by the heterogeneity test
that made the reliable estimates should be discounted. Fourthly,
this study is based on unadjusted estimates, while a more precise
analysis may be performed if individual data were available.
Finally, gene-gene and gene-environment interactions were not
investigated due to a lack of such information in the included
studies.
In conclusion, this systematic review and
meta-analysis suggests that the VEGF 936C/T, 1612G/A, −1154G/A,
−2549I/D, −460T/C and 405G/C gene polymorphisms are not associated
with the risk of RCC. There is no 702C/T polymorphism in RCC and
the −2578C/A gene polymorphism may be associated with an increased
risk of RCC. Due to the limitations of the present study, further
high quality case-control studies are warranted to confirm these
findings.
Acknowledgements
The authors would like to thank Dr Xian-Tao Zeng
(Department of Stomatology, Taihe Hospital, Hubei University of
Medicine) for the invaluable discussions about the study design and
statistical analyses.
References
|
1
|
Rini BI, Campbell SC and Escudier B: Renal
cell carcinoma. Lancet. 373:1119–1132. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gupta K, Miller JD, Li JZ, Russell MW and
Charbonneau C: Epidemiologic and socioeconomic burden of metastatic
renal cell carcinoma (mRCC): a literature review. Cancer Treat Rev.
34:193–205. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hunt JD, van der Hel OL, McMillan GP,
Boffetta P and Brennan P: Renal cell carcinoma in relation to
cigarette smoking: meta-analysis of 24 studies. Int J Cancer.
114:101–108. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bellocco R, Pasquali E, Rota M, et al:
Alcohol drinking and risk of renal cell carcinoma: results of a
meta-analysis. Ann Oncol. 23:2235–2244. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bjørge T, Tretli S and Engeland A:
Relation of height and body mass index to renal cell carcinoma in
two million Norwegian men and women. Am J Epidemiol. 160:1168–1176.
2004.PubMed/NCBI
|
|
6
|
Bergström A, Hsieh CC, Lindblad P, Lu CM,
Cook NR and Wolk A: Obesity and renal cell cancer - a quantitative
review. Br J Cancer. 85:984–990. 2001.
|
|
7
|
McLaughlin JK, Chow WH, Mandel JS, et al:
International renal-cell cancer study. VIII Role of diuretics,
other anti-hypertensive medications and hypertension. Int J Cancer.
63:216–221. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ferrara N: Vascular endothelial growth
factor. Trends Cardiovasc Med. 3:244–250. 1993. View Article : Google Scholar
|
|
9
|
Ferrara N and Davis-Smyth T: The biology
of vascular endothelial growth factor. Endocr Rev. 18:4–25. 1997.
View Article : Google Scholar
|
|
10
|
Zhou LP, Luan H, Dong XH, Jin GJ, Man DL
and Shang H: Vascular endothelial growth factor +936C/T
polymorphism and gastric cancer risk: A meta-analysis. Exp Ther
Med. 2:931–936. 2011.
|
|
11
|
Kleinrouweler CE, Wiegerinck MM,
Ris-Stalpers C, et al; EBM CONNECT Collaboration. Accuracy of
circulating placental growth factor, vascular endothelial growth
factor, soluble fms-like tyrosine kinase 1 and soluble endoglin in
the prediction of pre-eclampsia: a systematic review and
meta-analysis. BJOG. 119:778–787. 2012. View Article : Google Scholar
|
|
12
|
Toulis KA, Goulis DG, Mintziori G, et al:
Meta-analysis of cardiovascular disease risk markers in women with
polycystic ovary syndrome. Hum Reprod Update. 17:741–760. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lambrechts D, Poesen K, Fernández-Santiago
R, et al: Meta-analysis of vascular endothelial growth factor
variations in amyotrophic lateral sclerosis: increased
susceptibility in male carriers of the −2578AA genotype. J Med
Genet. 46:840–846. 2009.PubMed/NCBI
|
|
14
|
Banumathy G and Cairns P: Signaling
pathways in renal cell carcinoma. Cancer Biol Ther. 10:658–664.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Abe A, Sato K, Habuchi T, et al: Single
nucleotide polymorphisms in the 3′ untranslated region of vascular
endothelial growth factor gene in Japanese population with or
without renal cell carcinoma. Tohoku J Exp Med. 198:181–190.
2002.
|
|
16
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group. Preferred reporting items for systematic reviews
and meta-analyses: the PRISMA statement. BMJ. 339:b25352009.
View Article : Google Scholar
|
|
17
|
Higgins JP and Thompson SG: Quantifying
heterogeneity in a meta-analysis. Stat Med. 21:1539–1558. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ricketts C, Zeegers MP, Lubinski J and
Maher ER: Analysis of germline variants in CDH1, IGFBP3, MMP1,
MMP3, STK15 and VEGF in familial and sporadic renal cell carcinoma.
PLoS One. 4:e60372009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bruyère F, Hovens CM, Marson MN, et al:
VEGF polymorphisms are associated with an increasing risk of
developing renal cell carcinoma. J Urol. 184:1273–1278.
2010.PubMed/NCBI
|
|
21
|
Ajaz S, Khaliq S, Abid A, et al:
Association of a single-nucleotide polymorphism in the promoter
region of the VEGF gene with the risk of renal cell carcinoma.
Genet Test Mol Biomarkers. 15:653–657. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sáenz-Lopez P, Vazquez F, Cozar JM,
Carretero R, Garrido F and Ruiz-Cabello F: VEGF polymorphisms are
not associated with an increased risk of developing renal cell
carcinoma in Spanish population. Hum Immunol. 74:98–103. 2013.
|
|
23
|
Lutty GA, McLeod DS, Merges C, Diggs A and
Plouét J: Localization of vascular endothelial growth factor in
human retina and choroid. Arch Ophthalmol. 114:971–977. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Vincenti V, Cassano C, Rocchi M and
Persico MG: Assignment of the vascular endothelial growth factor
gene to human chromosome 6p21.3. Circulation. 93:1493–1495. 1996.
View Article : Google Scholar
|
|
25
|
Neufeld G, Cohen T, Gengrinovitch S and
Poltorak Z: Vascular endothelial growth factor (VEGF) and its
receptors. FASEB J. 13:9–22. 1999.PubMed/NCBI
|
|
26
|
Shahbazi M, Fryer AA, Pravica V, et al:
Vascular endothelial growth factor gene polymorphisms are
associated with acute renal allograft rejection. J Am Soc Nephrol.
13:260–264. 2002.PubMed/NCBI
|
|
27
|
Lambrechts D, Storkebaum E, Morimoto M, et
al: VEGF is a modifier of amyotrophic lateral sclerosis in mice and
humans and protects motoneurons against ischemic death. Nat Genet.
34:383–394. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Renner W, Kotschan S, Hoffmann C,
Obermayer-Pietsch B and Pilger E: A common 936 C/T mutation in the
gene for vascular endothelial growth factor is associated with
vascular endothelial growth factor plasma levels. J Vasc Res.
37:443–448. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Krippl P, Langsenlehner U, Renner W, et
al: A common 936 C/T gene polymorphism of vascular endothelial
growth factor is associated with decreased breast cancer risk. Int
J Cancer. 106:468–471. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Watson CJ, Webb NJ, Bottomley MJ and
Brenchley PE: Identification of polymorphisms within the vascular
endothelial growth factor (VEGF) gene: correlation with variation
in VEGF protein production. Cytokine. 12:1232–1235. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lam JS, Leppert JT, Figlin RA and
Belldegrun AS: Role of molecular markers in the diagnosis and
therapy of renal cell carcinoma. Urology. 66:1–9. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Haviv YS and Curiel DT: Gene therapy for
renal cancer. Contrib Nephrol. 159:135–150. 2008. View Article : Google Scholar
|
|
33
|
Hainsworth JD, Sosman JA, Spigel DR,
Edwards DL, Baughman C and Greco A: Treatment of metastatic renal
cell carcinoma with a combination of bevacizumab and erlotinib. J
Clin Oncol. 23:7889–7896. 2005. View Article : Google Scholar : PubMed/NCBI
|