Introduction
Breast cancer is the leading malignant disease among
females in the industrialized world. Although its incidence has
increased over the past decade, there has been a significant
decline in mortality from the disease in Denmark, possibly due to
advances in screening programs, surgical techniques and adjuvant
treatment (1). Despite this
progress, a significant number of females experience systemic
spread of the disease. Brain metastases, in particular, remain a
major cause of morbidity and mortality.
The subset of patients with overexpression of human
epidermal growth factor receptor 2 (HER2) has been reported to have
a high incidence of brain metastases (25–36%), even following
adjuvant treatment with trastuzumab. Risk factors for the
development of brain metastases in these patients include, estrogen
receptor (ER)-negative tumor tissue, liver metastases, tissue
HER2-positive disease and age <50 years (2–4).
At present, breast cancer patients are only
evaluated for brain metastases in cases of symptom presentation and
the use of magnetic resonance imaging (MRI) for the early diagnosis
of subclinical brain metastases remains controversial (5). Miller et al found no
improvement in overall survival among patients with brain
metastases detected by screening (6). However, Niwińska et al
demonstrated that whole brain radiotherapy reduced the risk of
mortality due to progression within the brain from 48 to 16%,
comparing symptomatic brain metastases with occult brain metastases
detected by MRI screening (7).
However, there was no difference in overall survival between the
two groups of patients.
Overexpression of the HER2 protein and/or
amplification of the HER2 gene is detected in 15–20% of breast
cancer tumors, leading to increased tumor cell proliferation, and
is associated with aggressive tumor behavior and poor prognosis
(8,9). In addition, HER2 overexpression and/or
amplification predicts the effect of HER2-targeted therapeutics,
including trastuzumab (Herceptin®) and lapatinib
(Tyverb®) in metastatic and adjuvant settings (10–12).
HER2 (neu, ErbB2 or p185HER2) is a tyrosine kinase
receptor in the HER family, which includes HER1 (EGFR), HER2, HER3
and HER4. The HER2 gene is located on chromosome 17 and encodes
HER2, which is a 185-kDa glycoprotein composed of an intracellular
tyrosine kinase domain, a transmembrane domain and an extracellular
domain with an unknown ligand (13). Activation of the HER2 pathway is
presumably driven by heterodimerization of HER2 with HER1, HER3 or
HER4 and the subsequent activation of the downstream pathway
(14).
The extracellular domain may be cleaved and measured
in serum as ‘serum HER2’ by an enzyme-linked immunosorbent assay
(15). The two most common assays
used for monitoring serum HER2, HER2/neu ELISA (Oncogene Science,
Cambridge, MA, USA) and ADVIA Centaur Serum HER2/neu assay (Siemens
Healthcare Diagnostics, Deerfield, IL, USA), have a reference
cut-off of 15 ng/ml (16). Carney
et al demonstrated elevated serum HER2 in 18% (0–38%) of
patients with primary breast cancer and in 46% (23–80%) of patients
with metastatic breast cancer (17). A number of studies have reported a
correlation between elevated levels of serum HER2 and clinical
outcome (18–22). In addition, specific studies have
reported increasing serum HER2 levels prior to the relapse of
breast cancer. However, the potential clinical implications
associated with these observations remain to be shown (23–25).
S100B is a calcium binding protein specific to
nervous tissue, including glial and Schwann cells. The protein has
been revealed as a homo- or heterodimer consisting of two subunits
(A and B) and S100B includes S100BB and S100AB. Depending on the
concentration, S100B stimulates neurite outgrowth, survival of
neurons or the expression of inflammatory cytokines and induces
apoptosis (26). Since S100B is a
relatively small protein (9–13 kDa), it has been hypothesized to
pass through the intact blood-brain barrier. However, elevated
S100B is only measured in serum under pathological conditions that
also compromise the blood-brain barrier. Serum S100B is measured by
immunoassays; however, as there is no established cut-off, it is
currently being determined which commercial S100B assays are more
accurate (27,28). Yoon et al measured serum
S100B in 74 healthy controls by the Elecsys S100 Immunoassay. The
authors found a reference value for the 95th percentile of 0.12
μg/l, which is in accordance with the cut-off of 0.105 μg/l
reported by the manufacturer (29).
The clinical utility of S100B has been evaluated in
various studies, indicating a correlation between increased serum
S100B and poorer outcome in traumatic brain injury and subarachnoid
hemorrhage. A small study of 20 glioma patients by Vos et al
demonstrated a significantly shorter median survival (25 vs. 38
months) in patients with serum S100B levels >0.09 μg/l (30). A large retrospective multicenter
study of 692 malignant melanoma patients found that elevated serum
S100B correlated with inferior overall survival, but only in the
univariate analysis (31). Serum
S100B has also been evaluated as a screening tool for asymptomatic
brain metastases in 38 newly diagnosed non-small cell lung cancer
patients. The study identified elevated serum S100B (0.28±0.19
μg/l) in all 7 patients with brain metastases identified by MRI
(32).
At present, no studies have examined the association
between elevated serum S100B and brain metastases or the use of
serum S100B as a screening tool for brain metastases in breast
cancer. Therefore, it is important to clarify whether elevated
serum S100B alone or together with serum HER2 correlates with the
incidence of brain metastases to identify patients for later
intervention studies testing the clinical effect of early
HER2-targeted treatment and radiotherapy. The aim of the present
study was to address this issue.
Patients and methods
Study population and patient samples
Two cohorts of patients were obtained from two
prospective studies (TL and VSL) performed at a single center
cancer hospital (Vejle Hospital, Denmark). Serum HER2 levels were
analyzed every 6 months during routine follow-up after primary
surgery for stage I–IIIA breast cancer or stage IV metastatic
breast cancer in a total of 1,308 patients. Patients provided
written informed consent. The two studies were approved by the
Regional Scientific Ethical Committee for Southern Denmark (project
nos. S-VF-20040017 and S-VF-20040101).
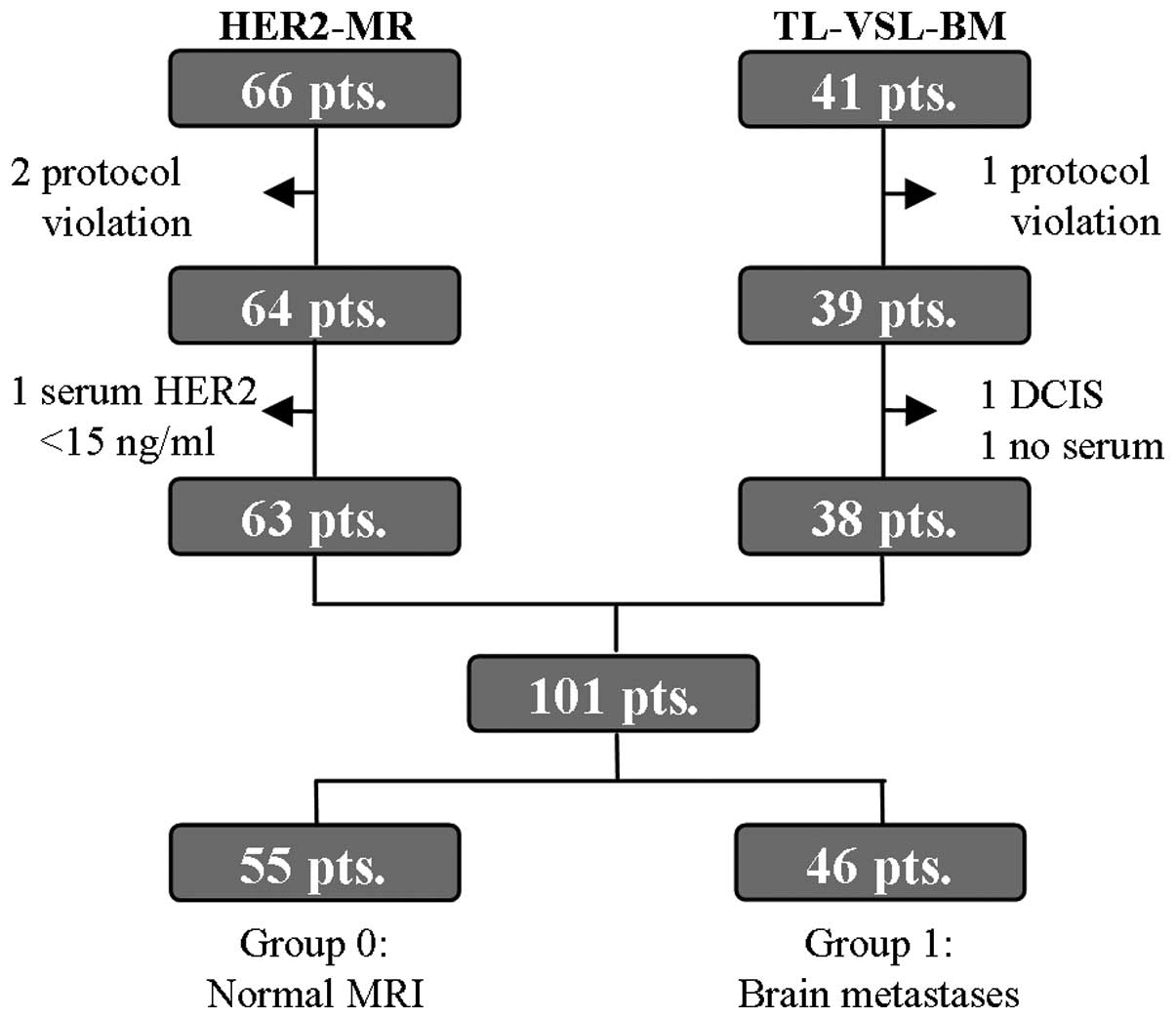
Sixty-six patients with elevated serum HER2 levels
>15 ng/ml during follow-up in the TL and VSL studies were
included in the HER2-MR protocol between 15 December, 2010 and 12
April, 2012. Individuals who provided written informed consent and
demonstrated no symptoms of brain metastases were eligible. Three
patients were excluded due to protocol violation or serum HER2
levels <15 ng/ml at the time of inclusion (Fig. 1). The remaining 63 patients (40
patients in follow-up after primary surgery and 23 with systemic
disease) underwent brain MRI and a computed tomography (CT) scan of
the thorax and abdomen if in follow-up without relapse. The MRI
scans were examined by two dedicated radiologists who reached
agreement in all cases. The CT scans were examined in a routine
setting. The protocol was approved by the Regional Scientific
Ethical Committee for Southern Denmark (project no.
S-20100080).
Forty-one patients (referred to as TL-VSL-BM),
treated with radiotherapy for MRI- or CT-verified brain metastases
between 25 August, 2005 and 20 June, 2011, were included if the
individual had received a serum HER2 test under the TL or VSL
protocol within 3 months prior to being diagnosed with brain
metastases. Three patients were excluded due to protocol violation,
only ductal carcinoma in situ (DCIS) at the primary surgery
or no serum remaining for analysis, leaving 38 patients for further
investigation. The additional analysis of serum S100B was also
approved by the Regional Scientific Ethical Committee for Southern
Denmark.
The remaining 101 patients were divided into two
groups: Group 0, the control group (n=55), consisting of patients
with normal MRI results and without symptoms of brain metastases;
and group 1 (n=46; 38 TL-VSL-BM and 8 HER2-MR patients), comprising
patients with MRI- or CT-verified meningeal and/or brain metastases
(Fig. 1). The two groups were
analyzed for serum HER2 and S100B levels prior to MRI or CT. Serum
samples were stored in a local biobank at −80°C.
Clinical and histopathological data
Histopathological data were obtained from the Danish
Breast Cancer Cooperative Group (DBCG) and verified in the local
database at the Department of Pathology, Vejle Hospital (Vejle,
Denmark). Clinical patient data were obtained from the local
electronic health record and complemented with data from the
nationwide online electronic health record containing data from all
Danish hospitals.
Biochemical and histopathological
methods
Tissue HER2 status was determined on
paraffin-embedded tumor tissue by immunohistochemistry (IHC) and
fluorescence in situ hybridization (FISH). The tumors were
considered to be HER2-positive when IHC3+ or IHC2+ with FISH ≥2.
IHC analysis was assessed by HerceptestTM
(DakoCytomation, Glostrup, Denmark), according to the
manufacturer’s instructions. IHC0 and IHC1+ were considered to
represent HER2-negative, whereas IHC3+ was defined as
HER2-positive. IHC2+ was considered to represent borderline and
therefore, to determine HER2 status, the HER2 FISH
pharmDxTM kit (DakoCytomation) was used. The threshold
for HER2 amplification was a ratio of ≥2.0 between HER2 gene copy
number and chromosome 17 centromere.
ER staining was performed on paraffin-embedded tumor
tissue using an anti-human ER monoclonal antibody (clone 1D5;
DakoCytomation) and visualized by the SuperSensitiveTM
Polymer-HRP IHC detection system (Biogenex, Fremont, CA, USA).
Tumors with nuclei staining ≥10% were considered to represent
ER-positive samples according to the contemporary DBCG
guidelines.
Serum HER2 was measured using the ADVIA Centaur HER2
Immunoassay (Siemens Healthcare Diagnostics). The assay is an
automated sandwich immunoassay using two monoclonal antibodies
against the extracellular domain of HER2 to detect serum HER2 by
direct chemiluminescent technology (33). The assay was controlled by an
in-house serum pool at 8 ng/ml and two commercial controls (Siemens
Healthcare Diagnostics) at 14 and 113 ng/ml. The inter-assay
coefficients of variation (CV) of these controls were 10.7, 5.8 and
4.6%, respectively.
Serum S100B was measured using the Elecsys S100
Immunoassay (Roche Diagnostics GmbH, Mannheim, Germany). The assay
is an automated sandwich immunoassay using two monoclonal
antibodies against S100B forming a complex to be measured by direct
chemiluminescent technology. Serum specimens were measured
according to the manufacturer’s instructions. The lower detection
limit was 0.005 μg/l and the assay was controlled by commercial
controls at 0.176 and 2.28 μg/l with an inter-assay CV between 1.3
and 3.6%.
Statistical methods
Statistical analyses were performed using STATA 11
(Statacorp, College Station, TX, USA). Fisher’s exact and Pearson’s
χ2 tests were used to compare categorical data.
Continuous variables were compared using the Mann-Whitney U test. A
multivariate logistic regression analysis was used for the
prognostic factors of brain metastases with dichotomized exposure
variables. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
Final analysis included 101 patients divided into
two groups: Group 0 (control group; n=55), patients with normal MRI
results and no symptoms of brain metastases; and group 1 (n=46),
patients with MRI- or CT-verified meningeal and/or brain
metastases. Table I outlines the
patient demographics and clinical characteristics of the two
groups. Clinical prognostic factors were significantly better in
group 0 when compared with that of group 1 with regard to axillary
nodal status (P=0.001) and systemic disease (P<0.001). In
addition, an increased number of patients in group 1 compared with
that of group 0 had systemic disease at the time of diagnosis. In
the two groups, a high proportion of tissue HER2-positive
individuals were identified. Similarly, differences in adjuvant and
palliative treatment were observed. As expected, a significantly
greater number of patients in group 1, when compared with that of
group 0, received palliative treatment instead of adjuvant therapy;
this was due to a greater number of patients in group 1 exhibiting
systemic disease at the time of diagnosis.
 | Table IPatient demographics and clinical
characteristics. |
Table I
Patient demographics and clinical
characteristics.
| Group 0a (n=55) | Group 1b (n=46) | |
|---|
|
|
| |
|---|
| Characteristic | n | % | n | % | P-value |
|---|
| Age, years |
| <40 | 3 | 5.5 | 6 | 13.0 | |
| 40–59 | 35 | 63.6 | 23 | 50.0 | |
| ≥60 | 17 | 30.9 | 17 | 37.0 | 0.238 |
| Type of surgery |
| Breast
conserving | 37 | 67.3 | 14 | 30.4 | |
| Mastectomy | 12 | 21.8 | 16 | 34.8 | |
| Neoadjuvant
chemo | 3 | 5.5 | 1 | 2.2 | |
| Primary systemic
BC | 3 | 5.5 | 15 | 32.6 |
<0.001 |
| Tumor type |
| Ductal | 46 | 83.6 | 33 | 71.7 | |
| Lobular | 1 | 1.8 | 2 | 4.3 | |
| Othersc | 8 | 14.5 | 11 | 23.9 | 0.372 |
| Tumor grade |
| 1 | 9 | 16.4 | 2 | 4.3 | |
| 2 | 20 | 36.4 | 17 | 37.0 | |
| 3 | 18 | 32.7 | 15 | 32.6 | |
| Unknownc | 8 | 14.5 | 12 | 26.1 | 0.170 |
| Tumor size |
| T1 | 22 | 40.0 | 16 | 34.8 | |
| T2 | 31 | 56.4 | 24 | 52.2 | |
| T3 | 2 | 3.6 | 6 | 13.0 | 0.254 |
| Nodal status |
| N0 | 27 | 49.1 | 8 | 17.4 | |
| N1 | 15 | 27.3 | 9 | 19.6 | |
| N2 | 4 | 7.3 | 11 | 23.9 | |
| N3 | 4 | 7.3 | 7 | 15.2 | |
| Multiple on
US/CTd | 5 | 9.1 | 11 | 23.9 | 0.001 |
| ER status |
| Negative | 18 | 32.7 | 17 | 37.0 | |
| Positive | 37 | 67.3 | 29 | 63.0 | 0.407 |
| HER2 IHC/FISH |
| Negative | 25 | 45.5 | 20 | 43.5 | |
| Positive | 30 | 54.5 | 26 | 56.5 | 1.000 |
| Systemic
disease |
| No | 40 | 72.7 | 2 | 4.3 | |
| Yes | 15 | 27.3 | 44 | 95.7 |
<0.001 |
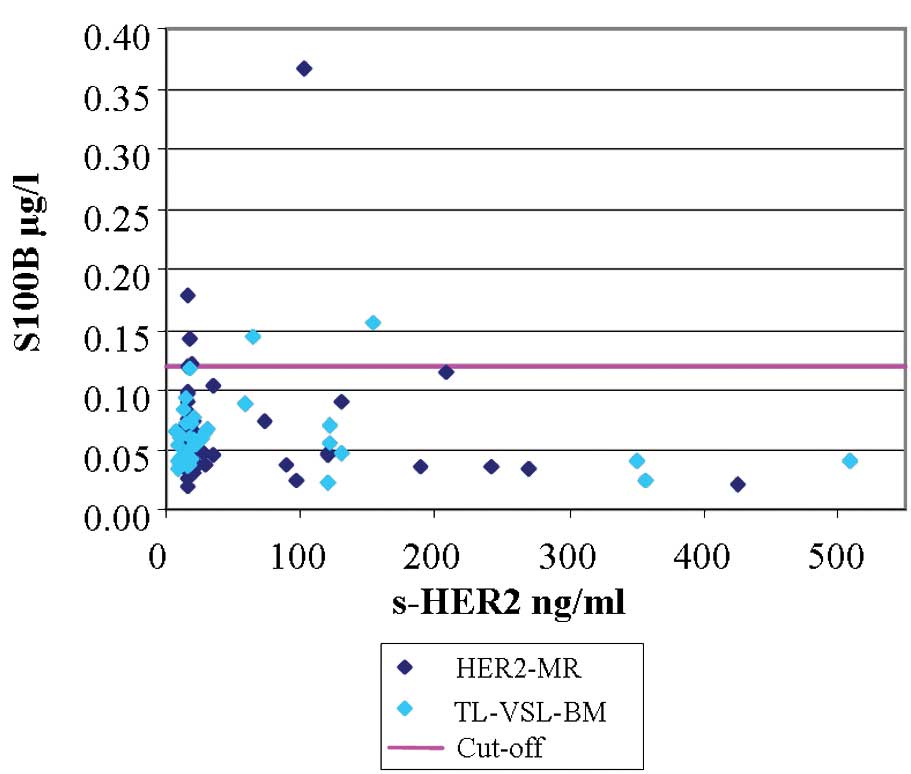
Serum S100B
Fig. 2 demonstrates
that no correlation was found between serum HER2 and S100B levels
with a correlation coefficient (r) of 0.077. Only four out of 63
patients from the HER2-MR protocol had a serum S100B value
exceeding the cut-off of 0.120 μg/l. Similarly, only two out of 38
TL-VSL-BM patients had a serum S100B value exceeding the cut-off.
Table II demonstrates the
sensitivity, specificity and positive and negative predictive value
of serum S100B. A total of four out of 46 patients with brain
metastases had a serum S100B level exceeding the cut-off of 0.120
μg/l, resulting in a sensitivity of 8.7% (95% CI, 3.2–14.2%).
| Table IISerum S100B prior to CT or MRI of the
brain. |
Table II
Serum S100B prior to CT or MRI of the
brain.
| Serum S100B | Group 0a | Group 1b | Total |
|---|
| Elevated (>0.120
μg/l) | 2 | 4 | 6 |
| Normal (≤0.120
μg/l) | 53 | 42 | 95 |
| Total | 55 | 46 | 101 |
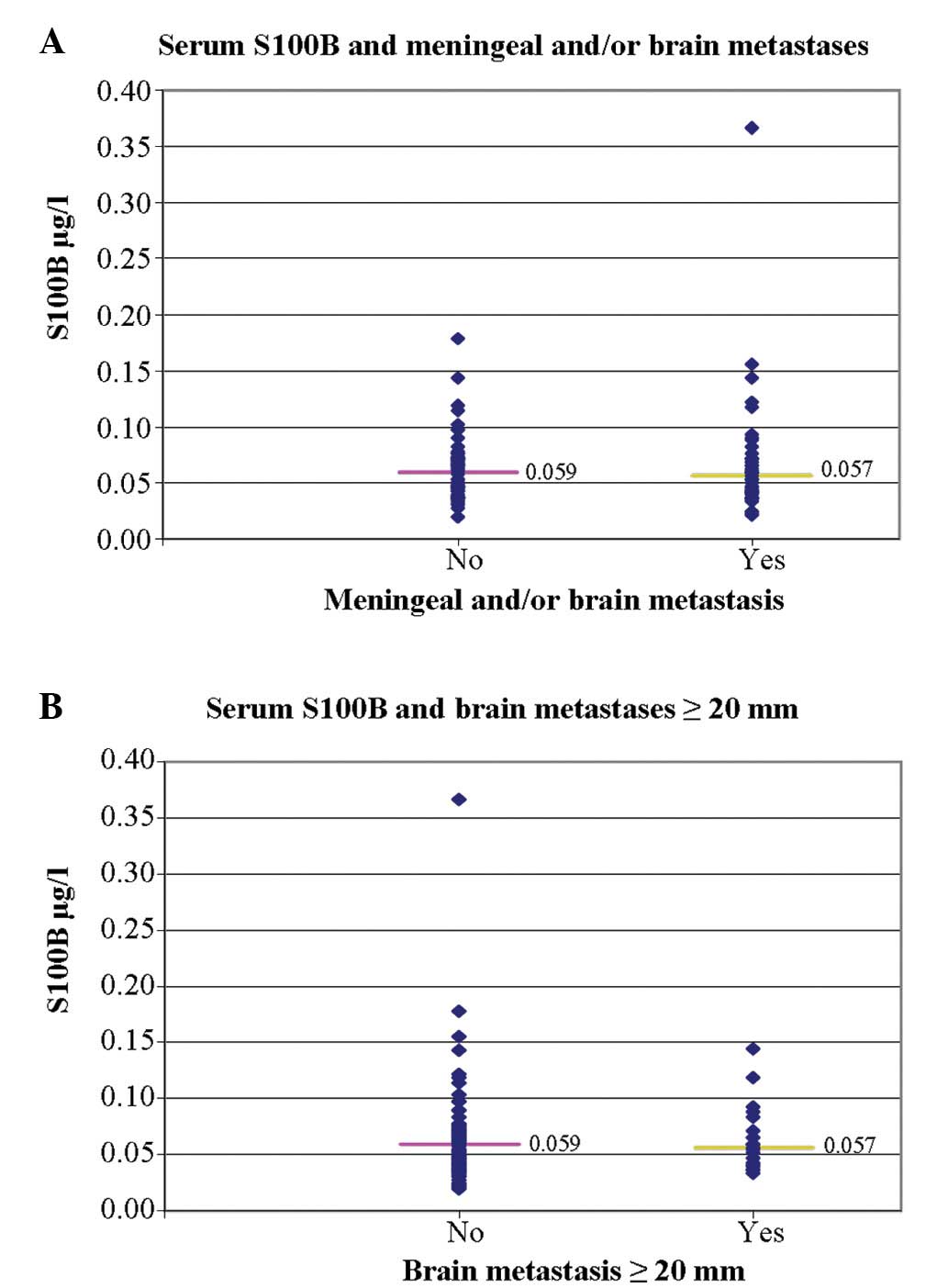
As presented in Fig.
3A, no significant differences were identified between serum
S100B levels of the 46 patients in group 1 with brain metastases
(median, 0.057 μg/l; range, 0.021–0.367 μg/l) and the 55 patients
in group 0 without brain metastases (median, 0.059 g/l; range,
0.020–0.178 μg/l) (P=0.623). Similarly, no significant differences
were identified between the 20 patients with brain metastases
>20 mm and the 81 patients with smaller or no brain metastases
(P=0.785; Fig. 3B). In addition, no
significant differences were identified in serum S100B levels
between the 59 patients with systemic disease (median, 0.054 μg/l)
and the 42 patients without systemic disease (median, 0.062 μg/l)
(P=0.241).
Serum HER2
No significant differences were identified in serum
HER2 levels between the 46 patients in group 1 with brain
metastases (median, 21.3 ng/ml; range, 7.6–508.7 ng/ml) and the 55
patients in group 0 without brain metastases (median, 16.5 ng/ml;
range, 15.1–207.8 ng/ml) (P=0.0598). This was also true when
investigating the difference between the 20 patients with the
largest brain metastases, >20 mm, compared with the 81 patients
with smaller or no brain metastases (P=0.8579).
The median value of serum HER2 was significantly
higher in the 59 patients with systemic disease, 44 with and 15
without brain metastases (median, 21.5 ng/ml), compared with the 42
patients without systemic disease (median, 16.0 ng/ml)(P=0.0002).
In addition, serum HER2 was significantly higher in the 31 patients
with liver metastases (median, 30.4 ng/ml) than in the 70 patients
without liver metastases (median, 16.7 ng/ml) (P=0.0011), and in
the 56 tissue HER2-positive patients (median, 19.6 ng/ml) compared
with the 45 tissue HER2-negative patients (median, 16.0 ng/ml;
P=0.0009) (data not shown).
Univariate and multivariate analysis of
the prognostic factors of brain metastases
In the current study, a univariate analysis of the
following variables was performed: Systemic disease (no/yes), age
(<60/≥60 years-old), tumor grade (1/2,3 and unknown, with
unknown grade corresponding to systemic disease at diagnosis),
tumor size (≤20/>20 mm), axillary lymph node metastases
(no/yes), ER status (negative/positive), serum HER2 (<30/≥30
ng/ml) and serum S100B (<0.072/≥0.072 μg/l). For serum HER2 and
S100B levels, the upper quadrant was compared with lower serum
levels, as we hypothesized that the highest serum levels correlated
with a poorer outcome and the possible differences, regardless of
known cut-off values, were to be analyzed in the present study.
Table III presents
the results of the univariate analysis, identifying systemic
disease (P<0.001), axillary lymph node metastases (P=0.001) and
serum HER2 (P=0.002) as statistically significant prognostic
factors of brain metastases. Levels of serum S100B were not
statistically significant in the univariate analysis (P=0.662).
| Table IIIUnivariate analysis of prognostic
factors of brain metastasis. |
Table III
Univariate analysis of prognostic
factors of brain metastasis.
| Factor | P-value |
|---|
| Systemic disease,
no/yes | <0.001 |
| Age, </≥60
years | 0.522 |
| Tumor grade,
</≥grade 2a | 0.054 |
| Tumor size,
≤/>20 mm | 0.590 |
| Lymph nodes,
−/+ | 0.001 |
| ER status, −/+ | 0.656 |
| HER2 IHC/FISH,
−/+ | 0.842 |
| Serum HER2,
</≥30 ng/ml | 0.002 |
| S100B, </≥0.072
μg/l | 0.662 |
The multivariate analysis was performed with the
four variables from the univariate analysis that resulted in
P<0.100. Only systemic disease (P<0.001) remained an
independent prognostic factor of brain metastases, whereas tumor
grade (P=0.095), axillary lymph node metastases (P=0.113) and serum
HER2 (P=0.894) were not statistically significant in the
multivariate analysis.
Discussion
In the current study, an extremely low number of
patients had serum S100B levels exceeding the cut-off value.
Subsequently, there was no difference in serum S100B between the
patients with and without brain metastases. In addition, patients
with the largest brain metastases, >20 mm and smaller or no
brain metastases were not found to have different S100B serum
levels. The comparison was based on the assumption that the largest
brain metastases would cause the greatest damage to the brain
tissue and the blood-brain barrier and subsequently have the
highest levels of serum S100B. These observations may have several
explanations.
Eigentler et al reported that serum S100B may
be elevated in patients with brain metastases from malignant
melanoma (31). However, in
contrast to breast cancer, there is an overexpression of S100B in
melanoma cells, which may explain the higher level of serum S100B
in the brain metastases from malignant melanoma (34). In addition, Vos et al
reported elevated serum S100B levels in patients with poorer
outcome of primary gliomas of the brain as S100B is also expressed
in gliomas (30). Korfias et
al demonstrated elevated serum S100B in patients with traumatic
head injury, where more diffuse damage to the glial cells is
expected when compared with that of the damage caused by relatively
slow growing metastases from breast cancer (26).
The current study did not find a significant
difference in the levels of serum HER2 between patients with and
without brain metastases; however, in the univariate analysis,
serum HER2 levels >30 ng/ml were identified as a prognostic
factor of brain metastases. These observations are consistent with
a study by Sørensen et al reporting that the predictive
value of serum HER2 to systemic relapse may be optimized with a
cut-off value between 25 and 32 ng/ml in tissue HER2-negative and
-positive patients, respectively (25). This may explain why no relapses in
the group of patients were reported during the follow-up, as serum
HER2 levels were only slightly >15 ng/ml.
The lack of differences in serum HER2 levels between
patients with and without brain metastases may be the result of
performing only one MRI screen during the current study in
connection with elevated serum HER2 levels in the HER2-MR protocol.
Therefore, it is possible that the new, smallest brain metastases,
not yet visible by MRI, were not detected, but elevated the serum
HER2 levels. However, we would expect relapse in certain cases if
there was a strong correlation, as the mean time from measurement
of elevated serum HER2 to MRI in this study was 71±58 days
(standard deviation). In future studies, sequential MRI must be
performed to identify a possible lead time from elevated serum HER2
levels to visible metastases by MRI, provided that the smallest
brain metastases have the capacity to cause elevated serum
HER2.
In the HER2-MR protocol, meningeal and/or brain
metastases were identified in eight out of 23 patients with known
systemic disease and six of these had tissue HER2-positive disease.
In future studies, when evaluating MRI screening for brain
metastases, it may be advantageous to focus on the tissue
HER2-positive patients with the highest serum HER2 levels in cases
of otherwise stable systemic disease. Alternatively, all patients
with tissue HER2-positive systemic disease must be offered MRI
screening for brain metastases, as it is anticipated that, in the
near future, improved targeted therapies are likely to be offered
to these patients.
In conclusion, the present study demonstrates that
quantitative measurement of serum S100B and serum HER2 cannot be
used to identify patients with an increased risk of brain
metastases. However, in the univariate analysis, serum HER2 levels
>30 ng/ml were found to correlate with an increased risk of
brain metastases, which warrants further investigation.
Acknowledgements
This study was financed by the Vejle Hospital
Research Foundation. HER2 kits were granted by Siemens Healthcare
Diagnostics. The authors thank Jens Hastrup, Pia Groth, Mette
Konradi, Sara Egsgaard and Camilla Davidsen for their excellent
laboratory work and Karin Larsen for proofreading. Ivan Brandslund
and Troels Bechmann have received remuneration for two lectures on
serum-HER2 from Siemens Healthcare Diagnostics.
References
|
1
|
NORDCAN. Cancer incidence, mortality,
prevalence and survival in the nordic countries, version 51. March.
2012, Association of the Nordic Cancer Registries. Danish Cancer
Society. http://www-dep.iarc.fr/NORDCAN/DK/StatsFact.asp?cancer=180&country=208.
Accessed November 28, 2012
|
|
2
|
Bendell JC, Domchek SM, Burstein HJ, et
al: Central nervous system metastases in women who receive
trastuzumab-based therapy for metastatic breast carcinoma. Cancer.
97:2972–2977. 2003. View Article : Google Scholar
|
|
3
|
Clayton AJ, Danson S, Jolly S, et al:
Incidence of cerebral metastases in patients treated with
trastuzumab for metastatic breast cancer. Br J Cancer. 91:639–643.
2004.PubMed/NCBI
|
|
4
|
Ono M, Ando M, Yunokawa M, et al: Brain
metastases in patients who receive trastuzumab-containing
chemotherapy for HER2-overexpressing metastatic breast cancer. Int
J Clin Oncol. 14:48–52. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Aukema TS, Olmos RA, Korse CM, et al:
Utility of FDG PET/CT and brain MRI in melanoma patients with
increased serum S100B level during follow-up. Ann Surg Oncol.
17:1657–1661. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miller KD, Weathers T, Haney LG, et al:
Occult central nervous system involvement in patients with
metastatic breast cancer: prevalence, predictive factors and impact
on overall survival. Ann Oncol. 14:1072–1077. 2003. View Article : Google Scholar
|
|
7
|
Niwińska A, Tacikowska M and Murawska M:
The effect of early detection of occult brain metastases in
HER2-positive breast cancer patients on survival and cause of
death. Int J Radiat Oncol Biol Phys. 77:1134–1139. 2010.PubMed/NCBI
|
|
8
|
Pauletti G, Dandekar S, Rong H, et al:
Assessment of methods for tissue-based detection of the HER-2/neu
alteration in human breast cancer: a direct comparison of
fluorescence in situ hybridization and immunohistochemistry. J Clin
Oncol. 18:3651–3664. 2000.
|
|
9
|
Slamon DJ, Clark GM, Wong SG, et al: Human
breast cancer: correlation of relapse and survival with
amplification of the HER-2/neu oncogene. Science. 235:177–182.
1987. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Slamon DJ, Leyland-Jones B, Shak S, et al:
Use of chemotherapy plus a monoclonal antibody against HER2 for
metastatic breast cancer that overexpresses HER2. N Engl J Med.
344:783–792. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Piccart-Gebhart MJ, Procter M,
Leyland-Jones B, et al; Herceptin Adjuvant (HERA) Trial Study Team.
Trastuzumab after adjuvant chemotherapy in HER2-positive breast
cancer. N Engl J Med. 353:1659–1672. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Romond EH, Perez EA, Bryant J, et al:
Trastuzumab plus adjuvant chemotherapy for operable HER2-positive
breast cancer. N Engl J Med. 353:1673–1684. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kurebayashi J: Biological and clinical
significance of HER2 overexpression in breast cancer. Breast
Cancer. 8:45–51. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Carney WP, Neumann R, Lipton A, et al:
Potential clinical utility of serum HER-2/neu oncoprotein
concentrations in patients with breast cancer. Clin Chem.
49:1579–1598. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Leitzel K, Teramoto Y, Sampson E, et al:
Elevated soluble c-erbB-2 antigen levels in the serum and effusions
of a proportion of breast cancer patients. J Clin Oncol.
10:1436–1443. 1992.
|
|
16
|
Molina R, Escudero JM, Muñoz M, et al:
Circulating levels of HER-2/neu oncoprotein in breast cancer. Clin
Chem Lab Med. 50:5–21. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Carney WP, Neumann R, Lipton A, et al:
Monitoring the circulating levels of the HER2/neu oncoprotein in
breast cancer. Clin Breast Cancer. 5:105–116. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Finn RS, Gagnon R, Di LA, et al:
Prognostic and predictive value of HER2 extracellular domain in
metastatic breast cancer treated with lapatinib and paclitaxel in a
randomized phase III study. J Clin Oncol. 27:5552–5558. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Esteva FJ, Cheli CD, Fritsche H, et al:
Clinical utility of serum HER2/neu in monitoring and prediction of
progression-free survival in metastatic breast cancer patients
treated with trastuzumab-based therapies. Breast Cancer Res.
7:R436–R443. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bramwell VH, Doig GS, Tuck AB, et al:
Changes over time of extracellular domain of HER2 (ECD/HER2) serum
levels have prognostic value in metastatic breast cancer. Breast
Cancer Res Treat. 114:503–511. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lipton A, Ali SM, Leitzel K, et al:
Elevated serum Her-2/neu level predicts decreased response to
hormone therapy in metastatic breast cancer. J Clin Oncol.
20:1467–1472. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ali SM, Carney WP, Esteva FJ, et al: Serum
HER-2/neu and relative resistance to trastuzumab-based therapy in
patients with metastatic breast cancer. Cancer. 113:1294–1301.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Molina R, Jo J, Filella X, et al:
C-erbB-2, CEA and CA 15.3 serum levels in the early diagnosis of
recurrence of breast cancer patients. Anticancer Res. 19:2551–2555.
1999.PubMed/NCBI
|
|
24
|
Fehm T, Gebauer G and Jäger W: Clinical
utility of serial serum c-erbB-2 determinations in the follow-up of
breast cancer patients. Breast Cancer Res Treat. 75:97–106. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sørensen PD, Jakobsen EH, Langkjer ST, et
al: Serum HER-2 concentrations for monitoring women with breast
cancer in a routine oncology setting. Clin Chem Lab Med.
47:1117–1123. 2009.PubMed/NCBI
|
|
26
|
Korfias S, Stranjalis G, Papadimitriou A,
et al: Serum S100B protein as a biochemical marker of brain injury:
a review of current concepts. Curr Med Chem. 13:3719–3731. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Erickson JA and Grenache DG: Comparison of
three assays for quantifying S100B in serum. Clin Chim Acta.
412:2122–2127. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Smit LH, Korse CM and Bonfrer JM:
Comparison of four different assays for determination of serum
S100B. Int J Biol Markers. 20:34–42. 2005.PubMed/NCBI
|
|
29
|
Yoon SM, Choi YJ, Kim HJ, et al:
Prognostic value of serum s100 protein by elecsys s100 immunoassay
in patients with spontaneous subarachnoid and intracerebral
hemorrhages. J Korean Neurosurg Soc. 44:308–313. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Vos MJ, Postma TJ, Martens F, et al: Serum
levels of S100B protein and neuron-specific enolase in glioma
patients: a pilot study. Anticancer Res. 24:2511–2514.
2004.PubMed/NCBI
|
|
31
|
Eigentler TK, Figl A, Krex D, et al;
Dermatologic Cooperative Oncology Group and the National
Interdisciplinary Working Group on Melanoma. Number of metastases,
serum lactate dehydrogenase level and type of treatment are
prognostic factors in patients with brain metastases of malignant
melanoma. Cancer. 117:1697–1703. 2011. View Article : Google Scholar
|
|
32
|
Vogelbaum MA, Masaryk T, Mazzone P, et al:
S100beta as a predictor of brain metastases: brain versus
cerebrovascular damage. Cancer. 104:817–824. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Olsen DA, Østergaard B, Bokmand S, et al:
HER-2 protein concentrations in breast cancer cells increase before
immunohistochemical and fluorescence in situ hybridization
analysis turn positive. Clin Chem Lab Med. 45:177–182. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cross SS, Hamdy FC, Deloulme JC and Rehman
I: Expression of S100 proteins in normal human tissues and common
cancers using tissue microarrays: S100A6, S100A8, S100A9 and
S100A11 are all overexpressed in common cancers. Histopathology.
46:256–269. 2005. View Article : Google Scholar
|