Introduction
Endoscopic retrograde cholangiopancreatography
(ERCP) is the mainstay treatment for numerous patients with
malignant obstructive jaundice. However, in specific cases, it is
difficult to perform when the main duodenal papilla infiltrated by
the tumor is endoscopically inaccessible. The main duodenal papilla
has been found inside a diverticulum in 5–23% of patients in an
ERCP study series (1). Therefore,
intradiverticular papillae are also one of the causes of the
endoscopic inaccessibility in the main duodenal papilla.
Percutaneous transhepatic biliary drainage (PTBD)
with stent insertion is an established procedure for the palliation
of patients with malignant biliary strictures. The current case
report describes percutaneous transhepatic biliary stenting (PTBS)
performed in two patients with malignant biliary strictures caused
by tumor infiltration of the major papilla and intradiverticular
papilla, a rarely reported situation.
Case report
Patient 1
The first patient was an 87-year-old male who
presented with a one-week history of obstructive jaundice.
Abdominal CT showed an ampullary mass surrounding the pancreatic
head with a large juxtapapillary diverticulum, as well as the
dilation of the extra- and intra-hepatic bile duct. ERCP revealed
intradiverticular papilla, bile flow into the diverticulum from the
major papilla and a nodular lesion around the diverticulum, with
the formation of a shallow ulcer. Cannulation of the major papilla
through ERCP failed. However, a biopsy was obtained from the nodule
lesion and a well-differentiated adenocarcinoma was confirmed by
pathological analysis. The patient was of advanced age and refused
surgery. PTBS was performed. The patient recovered well following
the procedure and was discharged from the hospital three days after
surgery.
Patient 2
The second patient was a 68-year-old female referred
to the Department of Interventional Radiology, Beijing Chaoyang
Hospital (Beijing, China) by an endoscopist following failed ERCP.
The patient refused surgery. Adenocarcinoma of the ampulla was
confirmed by biopsy. PTBS was performed to resolve obstructive
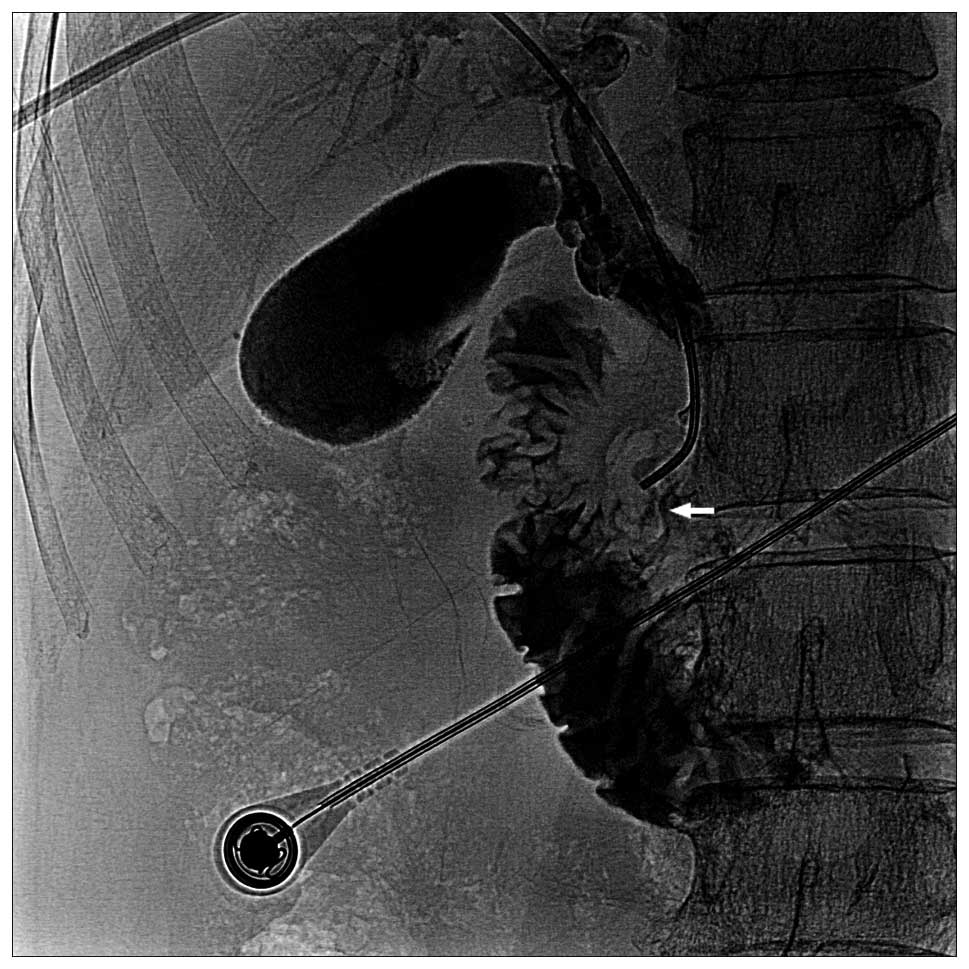
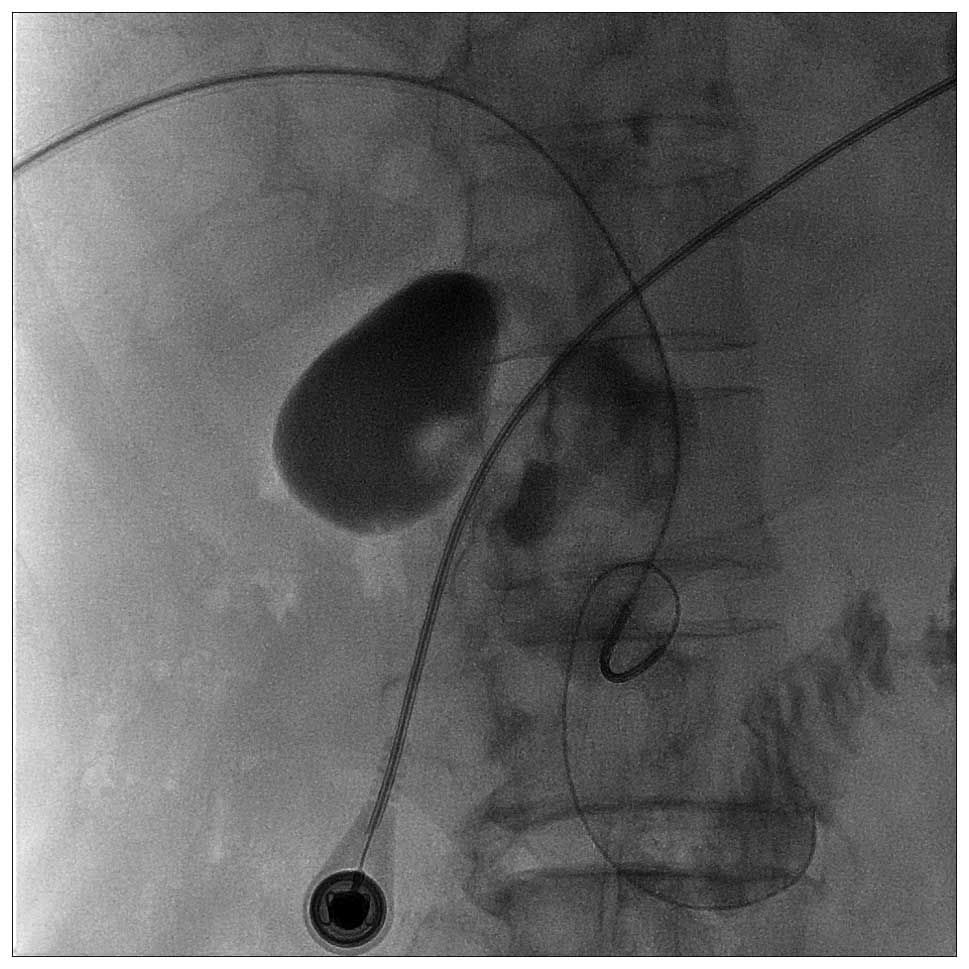
jaundice. The major papilla was located inside a large
juxtapapillary diverticulum during the procedure (Figs. 1–2).
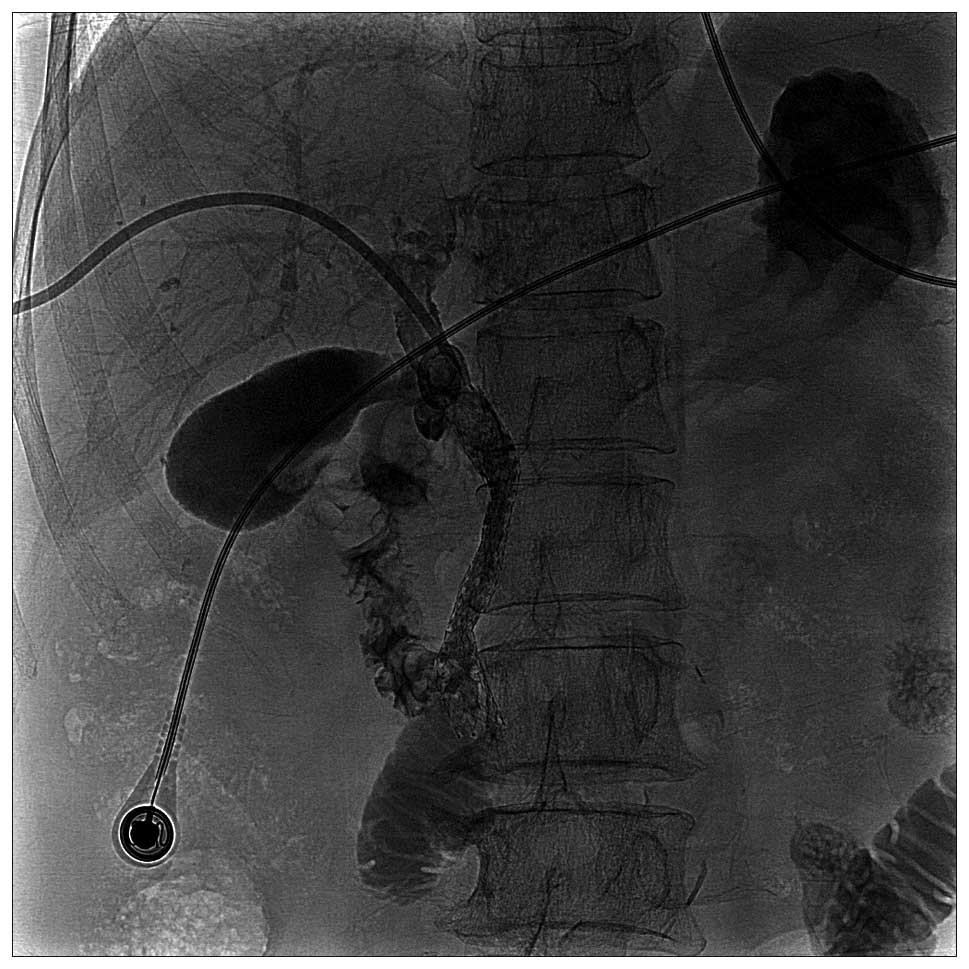
The biliary stent was implanted successfully to cover the stenotic
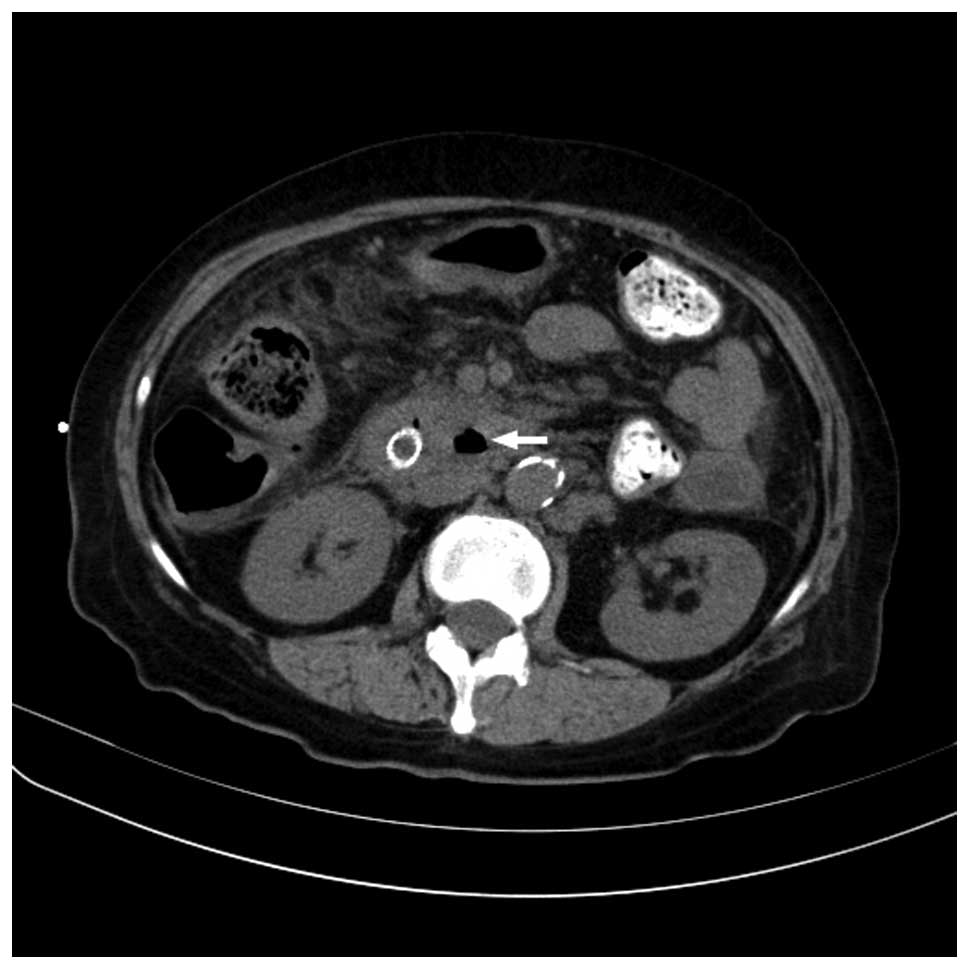
bile duct, with perfect cholangiographic results (Fig. 3). The patient experienced an
uneventful post-procedural outcome. CT performed 4 days after PTBS
showed the tumor surrounding the intradiverticular papilla
(Fig. 4).
PTBS
Written informed consent was obtained prior to the
interventional procedure in the two patients. PTBD was performed
using right lobe punctures under fluoroscopic guidance in each
patient. Access to the biliary tree was gained using standard
interventional techniques and a 7F sheath was inserted to
facilitate the following procedure. A 5F, 40-cm angled tip catheter
(Kumpe; William Cook Europe ApS, Bjaeverskov, Denmark) was used in
conjunction with a 0.035-inch hydrophilic guidewire (Radiofocus M;
Terumo Corporation, Tokyo, Japan) to advance through the papillary
stricture into the duodenum. The hydrophilic guidewire was
exchanged for a 0.035-inch stiff guidewire (Amplatz Super Stiff;
Boston Scientific, Natick, MA, USA). A 0.8×4.0-cm balloon (William
Cook Eurpoe ApS) was advanced over the guidewire towards the
duodenum to dilate the stricture and papilla orifice. Finally, a
self-expanding metallic stent (Zilver; William Cook Eurpoe ApS) was
inserted alongside the guidewire and through the papilla into the
duodenum.
PTBS was performed successfully without
procedure-associated complications in the two patients. The
patients remained well at the six-month post-procedure follow-up
visit.
Discussion
ERCP with endoscopic sphincterotomy is a
well-established procedure for the treatment of bile duct
strictures. ERCP with stent insertion in patients with malignant
pancreatic-biliary strictures has a success rate between 70 and 95%
(2). However, endoscopic stent
placement is difficult and in specific cases, is impossible in
patients who have intradiverticular papillae or tumor involvement
of the papillae (2). Failed
therapeutic ERCP due to deep cannulation of the obstructed bile
duct is precluded by severe duct angulation, a tight stricture or
infiltration by the tumor, and have been previously reported
(3,4). ERCP with modified techniques to treat
obstructive jaundice in patients with intradiverticular papilla has
been described in the literature (2,4–8).
PTBD with stent insertion is a well-established
technique for treatment of malignant biliary obstructions (9). Identification and selective
cannulation of the papillary orifice via the percutaneous
transhepatic route is a relatively simple process even when biliary
obstruction due to tumor infiltration occurs. The distortion of the
lower common bile duct caused by the duodenal diverticulum enables
the duct to form an acute angle as it enters the duodenum.
Technical modification and careful manipulation is required to
ensure success and avoid complications when malignant obstructive
jaundice caused by ampullary carcinoma is combined with
intradiverticular papillae. The present case report of two patients
describes the interventional procedures to gain access to the bile
duct. A 5F angled tip catheter used in conjunction with a soft,
angled tip guidewire allows successful cannulation of the
intradiverticular papilla, while reducing the risk of diverticular
perforation. A stiff guidewire was exchanged to allow the exertion
of greater force and to facilitate the insertion of balloon
catheter and stent catheter for balloon dilation and stent
insertion. Duodenal mucosa opacification inside the diverticulum
and duodenum is necessary to confirm the correct location and route
of the catheter (Fig. 1).
No case of PTBS has been reported in the literature
in patients with intradiverticular papilla and malignant
obstructive jaundice caused by ampullary carcinoma.
Intradiverticular papillae are not uncommon and must have been
identified during previous PTBD or PTBS procedures, however, to the
best of our knowledge, there is no prior case report of this event.
This may be due to the relative feasibility and safety of the
procedure with percutaneous transhepatic methods to pass the
intradiverticular papilla. PTBS appears to be forgotten in the
literature on treatment of malignant obstructive jaundice with
intradiverticular papilla in the era of endoscopy.
An advantage of endoscopic biliary drainage compared
with external PTBD is an improved quality of life due to the
internal placement of the stent (2). However, the quality of life of
patients with PTBS is comparable to that of patients undergoing
ERCP, since internal drainage through biliary stent insertion may
be performed. Further comparative study of PTBS verses ERCP is
required to evaluate the technical and treatment outcomes.
In conclusion, PTBS is potentially a safe and
feasible technique for patients with an endoscopically inaccessible
intradiverticular papilla and malignant obstructive jaundice caused
by ampullary carcinoma. Endoscopists and interventional
radiologists must be aware of this under-reported occurrence and
offer appropriate management options to patients.
References
|
1
|
Külling D and Haskell E: Double endoscope
method to access intradiverticular papilla. Gastrointest Endosc.
62:811–812. 2005.PubMed/NCBI
|
|
2
|
Tarantino I, Barresi L, Fabbri C and
Traina M: Endoscopic ultrasound guided biliary drainage. World J
Gastrointest Endosc. 4:306–311. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Brauer BC, Chen YK, Fukami N and Shah RJ:
Single-operator EUS-guided cholangiopancreatography for difficult
pancreaticobiliary access (with video). Gastrointest Endosc.
70:471–479. 2009. View Article : Google Scholar
|
|
4
|
Mallery S, Matlock J and Freeman ML:
EUS-guided rendezvous drainage of obstructed biliary and pancreatic
ducts: report of 6 cases. Gastrointest Endosc. 59:100–107. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Burmester E, Niehaus J, Leineweber T and
Huetteroth T: EUS-cholangio-drainage of the bile duct: report of 4
cases. Gastrointest Endosc. 57:246–251. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kahaleh M, Wang P, Shami VM, Tokar J and
Yeaton P: EUS-guided transhepatic cholangiography: report of 6
cases. Gastrointest Endosc. 61:307–313. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim YS, Gupta K, Mallery S, Li R, Kinney T
and Freeman ML: Endoscopic ultrasound rendezvous for bile duct
access using a transduodenal approach: cumulative experience at a
single center. A case series. Endoscopy. 42:496–502. 2010.
View Article : Google Scholar
|
|
8
|
Rajnakova A, Goh PM, Ngoi SS and Lim SG:
ERCP in patients with periampullary diverticulum.
Hepatogastroenterology. 50:625–628. 2003.PubMed/NCBI
|
|
9
|
Garcarek J, Kurcz J, Guzinski M, Janczak D
and Sasiadek M: Ten years single center experience in percutaneous
transhepatic decompression of biliary tree in patients with
malignant obstructive jaundice. Adv Clin Exp Med. 21:621–632.
2012.
|