Introduction
Neuroendocrine tumors were first described by
Langhans in 1867 (1).
Neuroendocrine carcinoma (NEC) is a type of malignant tumor in
which cells often show amine precursor uptake and decarboxylation
to synthesize and secrete amine and polypeptide hormones. Gastric
neuroendocrine tumors (gastric carcinoids) have been classified on
the basis of pathogenesis and histomorphologic characteristics into
three types differing in biological behavior and prognosis. Gastric
neuroendocrine tumor types 1 and 2 are usually considered benign
with a low risk of malignancy. Type 3 gastric neuroendocrine tumors
are composed of different endocrine cells, including poorly
differentiated endocrine and exocrine cells, which grow
sporadically, irrespective of gastrin in an otherwise normal
mucosa. The majority of these tumors show a low- to high-grade
malignant transformation, already metastasizing at the time of
diagnosis Endocrine tumors, which primarily exist in the stomach,
account for only 2–6% of gastrointestinal endocrine tumors. Among
all gastric cancer types, endocrine tumors account for only
0.1–0.9% of cases (2). This report
presents a rare clinical case of three types of malignant tumors
localized in the stomach; NEC, moderately differentiated
adenocarcinoma and mucinous adenocarcinoma. Written informed
consent was obtained from the patient for publication of this case
report and any accompanying images.
Case report
Case presentation
A 65-year-old male patient presented with occasional
shortness of breath following activities and appeared weak 1 month
ago, with no evidence of underlying disease. The patient had no
history of lung disease and was negative for family hereditary
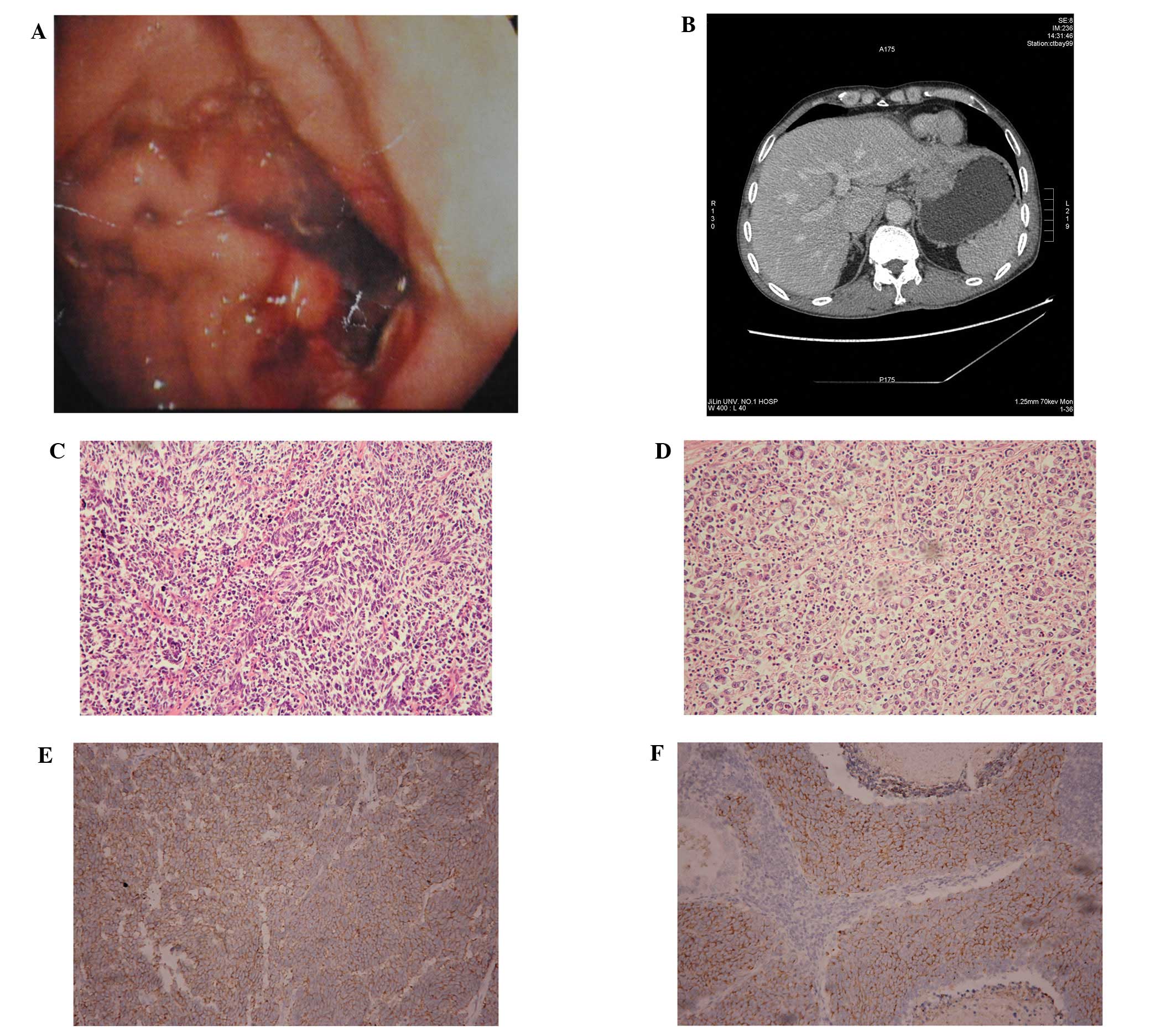
disease. Auxiliary examination consisted of contrast-enhanced
computed tomography (CT) of the stomach, which identified the
following: Lesser curvature of the stomach, obvious thickening of
the stomach angle, discontinuous mucous membrane layer and a coarse
serous membrane layer, part of which was not clearly divided from
the left side of the liver. Enhancement scanning showed uneven
obvious strengthening of the tumor in the lesser curvature of the
stomach. CT results identified that the staging of the tumor was
T3N3M0 (Fig. 1). Gastric fiberscopy
revealed that the tumor occupied the bottom of the stomach and the
diameter of its body curvature side was 1.5×1.5 cm, with central
depression and covered with ulcer and necrotic tissues.
Additionally, the mucosal lining was rough. These results showed
obvious congestion and edema. The elasticity of the inspected
tissue was stiff and hemorrhaged when touched. The tumor lied in
the lesser curvature of the lower part of the stomach and the body
of the stomach (Fig. 1A). Biopsy of
the stomach tissue specimens identified that several glands
exhibited severe dysplasia, not excluding well-differentiated
adenocarcinoma; therefore, advanced examination was suggested.
Laboratory examination showed anemia (hemoglobin level, 71 g/l).
The level of the tumor marker, CA72-4, in the blood was 9.8 U/ml
(normal range, 0–6.9 U/ml) and the carcinoembryonic antigen level
was 6.52 ng/ml (normal range, <3.4 ng/ml).
Surgery
The patient underwent a laparoscopic total
gastrectomy (Roux-en-Y anastomosis) under general anesthetic (D2
and R0 resection). During surgery two tumors were identified: Tumor
1 was located in the gastric curvature near the cardia, which was
~5×3.5×1 cm in size; tumor 2 was located in the back wall of the
gastric body and was ~8×4.5×2 cm in size. The two tumors were 5 cm
apart.
Pathological analysis
Postoperative pathological diagnosis found that
there were two independent and different morphological lesions in
the stomach. Tumor 1 included two types of carcinoma (Fig. 1C), NEC and moderately differentiated
adenocarcinoma, which can be referred to as mixed carcinoma or
collision carcinoma, invading the subserosal connective tissue.
Immunohistochemical results for NEC revealed: Chromogranin A (CgA;
+) (Fig. 1E), synaptophysin (Syn;
+) (Fig. 1F), vimentin (+), thyroid
transcription factor-1 (+), CD117 (+) and Ki67 (+ 80%); while those
for moderately differentiated adenocarcinoma were as follows: Ki67
(20%), epithelial membrane antigen (EMA; +), CK20 (+), CK7 (+) and
villin (+).
Tumor 2 was mucinous adenocarcinoma invading the
plasma membrane. The majority of cancer tissues were diffused by
individual cells, which were clumped together to create a mass
tumor, and only a few were physaliphorous cells. The vessel and
nerve were infiltrated with carcinoma. Immunohistochemical analysis
of the mucinous adenocarcinoma revealed: CK (+), EMA (+), Ki67 (+80
%) and vimentin (+). In the lesser curvature of the stomach, the
number of the metastasis lymph nodes was 2 out of 5 total lymph
nodes. All the metastasis lymph nodes were neuroendocrine
carcinoma.
Chemotherapy
The patient received six cycles of FOLFOX
chemotherapy regimen 3 weeks after surgery. Follow-up revealed that
the patient survived and was tumor-free 12 months after
surgery.
Discussion
The origin of mixed gland - NEC has not been fully
elucidated. The majority of scholars propose that NEC in the
digestive system originated in the neuroendocrine cells of the
digestive system, which were derived from the endoderm and,
therefore, have the same origin as gastrointestinal epithelium.
Both tumor types originate from totipotent stem cells. Under the
action of carcinogenic factors, totipotent stem cells undergo
malignant differentiation to produce NEC, squamous cell carcinoma
and adenocarcinoma. NEC and adenocarcinoma have the same risk
factors, including dietary, hereditary, environmental and
psychological factors. Gastric neuroendocrine tumors can be divided
into three types of tumors according to the World Health
Organization (WHO, 2000): Well-differentiated neuroendocrine tumor
(carcinoid), well-differentiated NEC and poorly differentiated NEC
(high-grade NEC; WHO, 2010) (3).
The differentiation of gastric neuroendocrine tumors has been
reported as a step-by-step process: i) gastric endocrine cell
hyperplasia; ii) dysplasia; iii) gastric carcinoid
(well-differentiated); iv) atypical carcinoid (intermediately
differentiated); and v) NEC (poorly differentiated) (4). Gastric tumors have been mainly
detected by gastric endoscopy (5).
NEC and adenocarcinoma are difficult to diagnose and identify by
gastroscopy or ultrasound. Therefore, clarifying a diagnosis can
rely on histopathological examination, and immunohistochemistry is
the most common method. The widely used indicators for
immunohistochemistry are QrA, Syn and neuron-specific enolase,
while CgA and Syn have high specificity (6,7). MEN1
gene detection from blood samples and positron emission tomography
CT scanning have been reported as advanced methods for the
diagnosis of NEC and adenocarcinoma. The treatment of NEC includes
surgery, radiotherapy, systemic chemotherapy, biological therapy
and targeted drug therapy (8).
The present report demonstrated a case of three
types of malignant tumors localized in the stomach, including NEC,
moderately differentiated adenocarcinoma and mucinous
adenocarcinoma. NEC and moderately differentiated adenocarcinoma
existed simultaneously in the same lesion, and the cells were
intermixed. To the best of our knowledge, this was the first case
report of three types of malignant tumors existing in the stomach
at the same time. According to the grading standard of the European
Neuroendocrine Tumor Association (9), gastric NEC in this case was T2N1M0,
stage IIIB stomach cancer; and the mucinous gastric carcinoma was
T4aN3M0, stage IV stomach cancer. The three types of malignant
tumors, including NEC, existing in one stomach, were highly
malignant and the patient had a poor prognosis. The patient
underwent laparoscopic-assisted D2 radical total gastrectomy and
Roux-en-Y esophagus-jejunum anastomosis. The surgery was
successful. The patient also received FOLFOX chemotherapy for six
cycles 3 weeks after surgery. Follow-up determined that the patient
survived and was tumor-free 12 months after surgery. According to
this case report, radical surgery combined with chemotherapy can
effectively improve the prognosis of patients with these three
specific tumor types simultaneously in the stomach.
References
|
1
|
Langhans T: Ueber einen drüsenpolyp im
Ileum. Virchows Arch Pathol Anat. 38:550–560. 1867.(In German).
|
|
2
|
Hirano Y, Hara T, Nozawa H, et al:
Combined choriocarcinoma, neuroendocrine cell carcinoma and tubular
adenocarcinoma in the stomach. World J Gastroenterol. 14:3269–3272.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sata N, Tsukahara M, Koizumi M, et al:
Primary small-cell neuroendocrine carcinoma of the duodenum- a case
report and review of literature. World J Surg Oncol. 2:282004.
View Article : Google Scholar
|
|
4
|
Kuroda N, Oonishi K, Iwamura S, Ohara M,
Hirouchi T, Mizumo K, Miyazaki E and Enzan H: Gastric
carcinosarcoma with neuroendocrine differentiation as the carcinoma
component and leiomyosarcomatous and myofibroblastic
differentiation as the sarcomatous component. APMIS. 114:234–238.
2006. View Article : Google Scholar
|
|
5
|
Shpaner A and Yusuf TE: Primary gastric
small cell neuroendocrine carcinoma. Endoscopy. 39(Suppl 1):
E310–E311. 2007. View Article : Google Scholar
|
|
6
|
Nassar H, Albores-Saavedra J and Klimstra
DS: High-grade neuroendocrine carcinoma of the ampulla of vater: a
clinicopathologic and immunohistochemical analysis of 14 cases. Am
J Surg Pathol. 29:588–594. 2005. View Article : Google Scholar
|
|
7
|
Moran CA and Suster S: Neuroendocrine
carcinomas (carcinoid, atypical carcinoid, small cell carcinoma,
and large cell neuroendocrine carcinoma): current concepts. Hematol
Oncol Clin North Am. 21:395–407. 2007. View Article : Google Scholar
|
|
8
|
Hosoya Y, Nagai H, Koinuma K, Yasuda Y,
Kaneko Y and Saito K: A case of aggressive neuroendocrine carcinoma
of the stomach. Gastric Cancer. 6:55–59. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rindi G, Klöppel G, Alhman H, et al: TNM
staging of foregut (neuro)endocrine tumors: a consensus proposal
including a grading system. Virchows Arch. 449:395–401. 2006.
View Article : Google Scholar
|