Introduction
An ectopic pancreas is pancreatic tissue which lacks
anatomic and vascular continuity with the main body of the
pancreas, it is also known as an aberrant pancreas or heterotopia
of the pancreas (1–12). Although there are two different
hypotheses, the etiology of ectopic pancreas remains unclear
(10). An ectopic pancreas is a
developmental anomaly normally located in the gastrointestinal
tract, including the stomach, duodenum, jejunum and ileum (7,8). An
ectopic pancreas in the mediastinum is particularly uncommon. To
the best of our knowledge, since the existence of anterior
mediastinal ectopia of pancreatic tissue was verified
pathologically by Klob in 1859 for the first time (1), there are only 12 cases in the English
literature up to January 2013 (2–12).
Herein, we present the clinical, radiological and histopathological
findings of an uncommon ectopic pancreas in the anterior
mediastinum for a better understanding of this entity.
Case reports
Case 1
A 15-year-old male was referred to West China
Hospital, Sichuan University (Chengdu, China) with complaints of
chest pain, coughing and fever. There were no positive findings on
physical examination and laboratory studies. A contrast-enhanced
computed tomography (CT) scan was subsequently performed on the
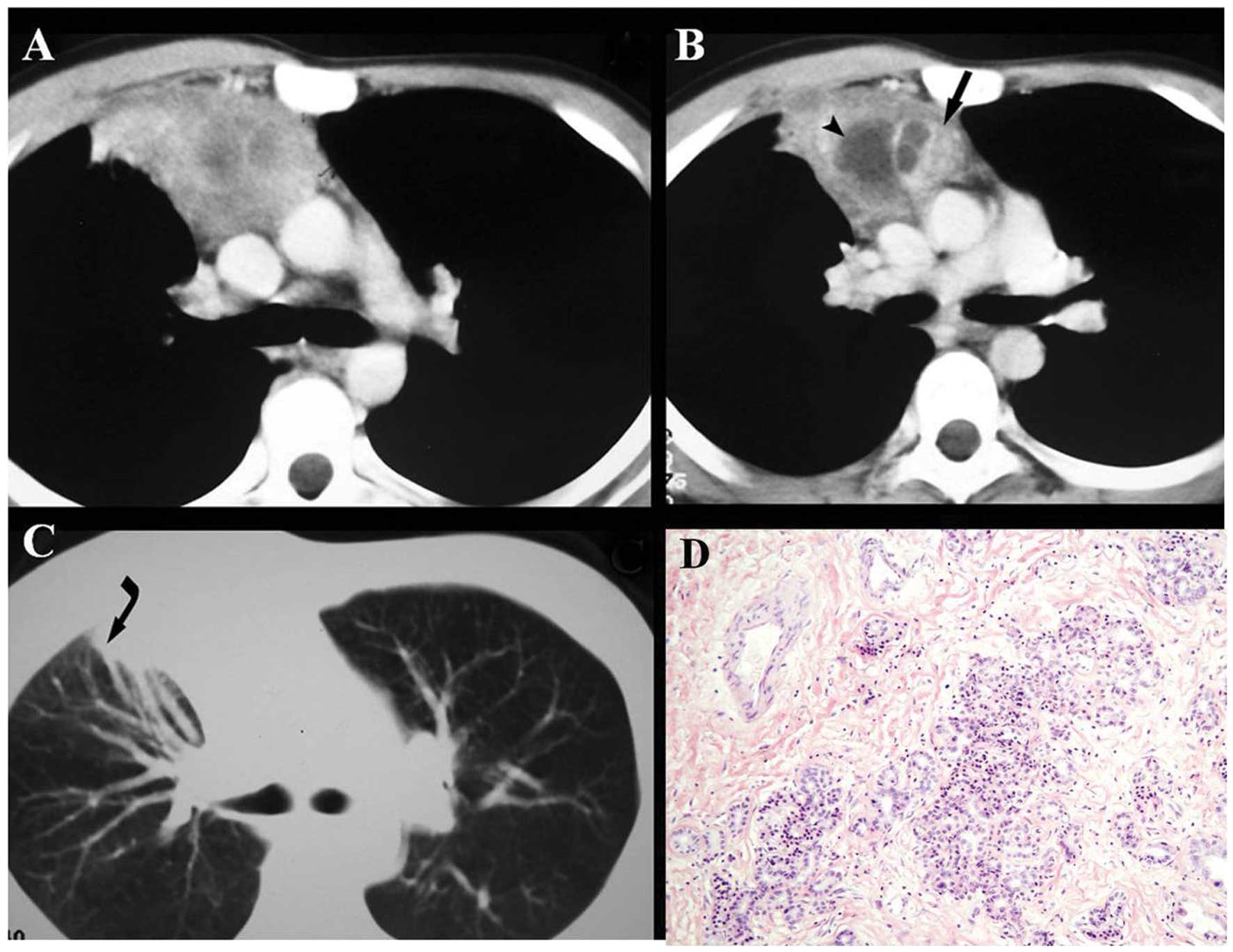
thorax. As shown on enhanced CT images, an irregular soft tissue
mass measuring 7.0×4.5 cm was identified in the anterior
mediastinum and extended to the anterior segment of the right upper
lung, with partial consolidation. The mass was markedly and
heterogeneously enhanced, whereas necrotic and liquefied
non-enhanced areas were observed in the center of the mass. The
lesion obscured the anterior chest wall and adjacent vascular
structures, including the ascending aorta and superior vena cava
(Fig. 1A–C). No destruction of the
sternum and ribs, and no pleural effusion were found. A provisional
diagnosis of thymoma was suspected.
The chest was opened by a median sternotomy
incision. A solid and hard mass in the anterior mediastinum had
firm adhesions to the superior vena cava, left brachiocephalic
vein, pericardium, the mediastinal pleura and anterior chest wall.
The anterior segment of the right upper lung was also invaded. The
mass and part of the anterior segment of the right upper lung were
together removed. Since no malignancy was reported from the
frozen-section of the lesion, no further dissection was
performed.
Histopathologically, the lesion exhibited abnormally
differentiated and disorganized pancreatic lobules with acini,
ducts, islets and malformed vessels. The pancreatic lobular
architectures of the lesion were sparser than that of the
pancreatic tissue located in the normal anatomic site (Fig. 1D). Therefore, an ectopic pancreas
with encapsulated fibrous tissue without clear boundary in the
anterior mediastinum was confirmed. Following surgery, the patient
remained well and was asymptomatic with no evidence of recurrence
or metastasis during a follow-up period of eight years.
Case 2
A 16-year-old female with a six-month history of
throat discomfort and neck swelling was referred to West China
Hospital for further evaluation. Physical examination revealed that
the soft tissue mass arising from the abdomen was soft, and the
patient experienced tenderness on deep palpation. Routine
laboratory findings were within normal range.
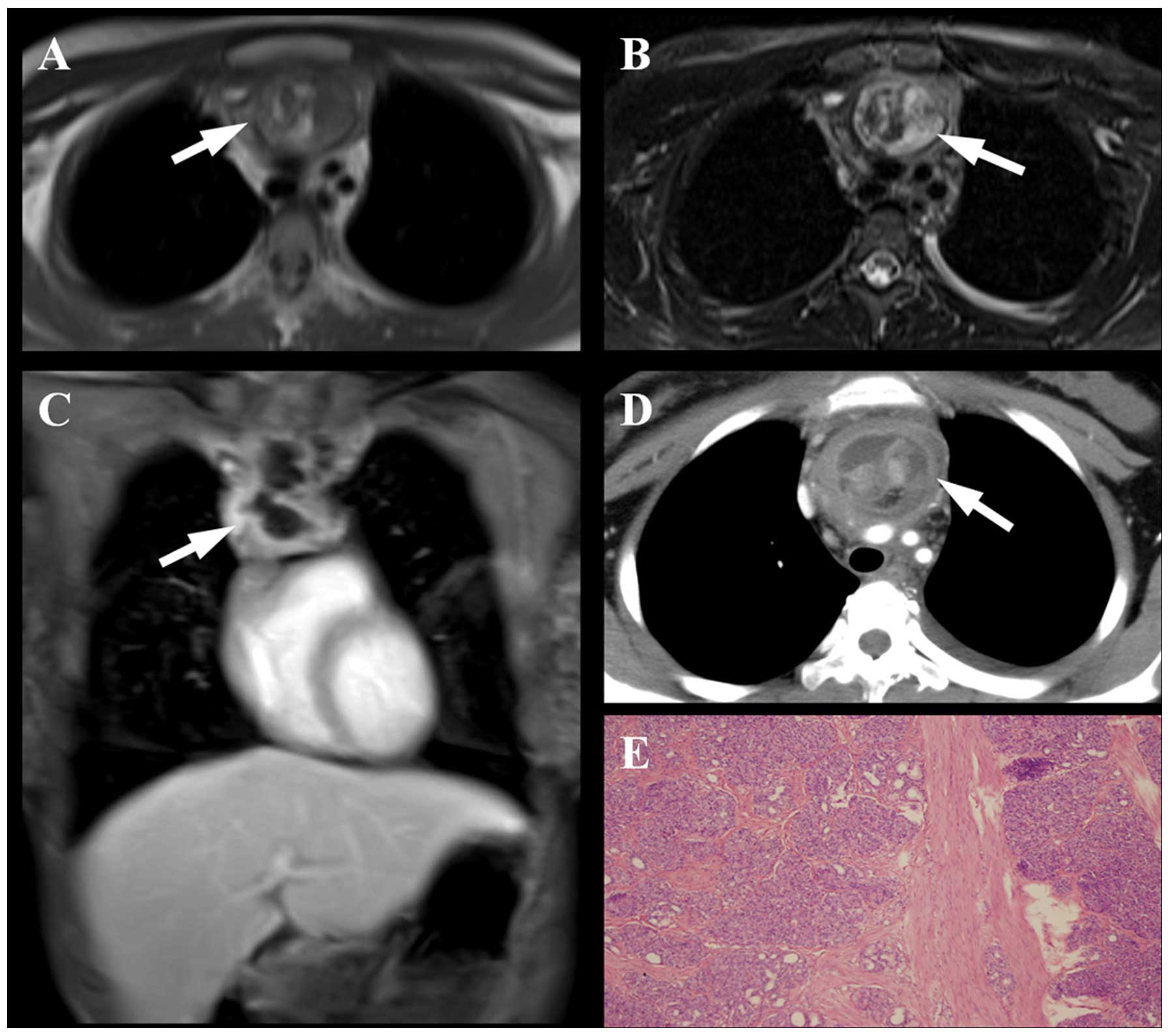
Chest radiograph demonstrated a soft tissue mass in
the anterior mediastinum. Unenhanced CT findings revealed a 6-cm
heterogeneous mass at the region of the anterior mediastinum.
Within the mass, there was an area of adipose tissue. There was no
calcification in the mass. The mass enhanced slightly following
intravenous administration of contrast material. MRI showed a
heterogeneous anterior mediastinum mass with fat, solid and cystic
components (Fig. 2A–D). The thymus
itself was not identified. The poorly circumscribed mass invaded
the adjacent structures, including the pericardium, mediastinal
vessels, anterior tracheal wall and the lower pole of the thyroid.
A small amount of pleural effusion was found. No sign of bony
involvement was revealed. A tentative pre-operative diagnosis of a
malignant tumor of undetermined origin, teratoma or invasive
thymoma was considered on the basis of the imaging findings.
Surgical resection was then performed under anesthesia. A mass
located posterior to the sternum was found, which adhered to the
superior vena cava, innominate vein, the adjacent pericardium and
pleura. There was no evidence of abnormal lymph nodes or lung
involvement.
Histologically, the mass was finally diagnosed as an
ectopic pancreas in the mediastinum (Fig. 2E). Postoperatively, the patient
recovered uneventfully and no recurrence or metastasis was observed
during the six months of follow-up.
This study was approved by the Institutional Review
Board of Sichuan University (Chengdu, China). Written informed
consent was obtained from both patients.
Discussion
Ectopic pancreas, also named aberrant pancreas or
heterotopia of the pancreas, is defined as pancreatic tissue
lacking anatomic and vascular continuity with the main body of the
pancreas. Ectopia of the pancreatic tissue is a developmental
anomaly found in ~2% of all autopsies, and 70~90% of these
anomalies are located in the gastrointestinal tract (10). Mediastinal localization of ectopic
pancreas is extremely rare. According to previous reports (2–12) and
the present cases, mediastinal ectopic pancreas can have a number
of common characteristics, as follows: i) of the twelve cases, nine
females and three males, all ectopias of the pancreas occurred in
the anterior mediastinum; ii) the symptoms of the patients were
nonspecific; iii) the masses were usually large with cystic changes
due to failing to drain the exocrine fluid, inflammatory exudate
and bleeding in ectopic pancreas (7); and iv) the majority of cases had a
good prognosis following surgery.
As a developmental anomaly, the histogenesis of
ectopic pancreas is not clear. There are two different theories on
the embryogenesis of this anomalous development (10). First, ectopic pancreatic tissue in
the mediastinum may be the result of the abnormal differentiation
of the pluripotent epithelial cells of the ventral primary foregut,
since the pancreas and the lower respiratory tract share a common
embryologic origin, the primitive foregut. Second, a number of
cells from the pancreatic bud may migrate and locate at a different
site.
As for the symptoms, they are related to the size
and location of the lesion, as well as whether an inflammation
developed or not. The patient in case 1 of the present study had
chest pain, cough and fever. We speculate that the symptoms
resulted from the compression of the large mass and infiltrative
inflammation of the ectopic pancreas, since the patient remained
asymptomatic following surgery. According to the present
perspective, as long as there is an ectopic pancreas present, it
should be managed by surgery to prevent cystic and malignant
changes, or to stop it affecting surrounding organs and tissues
(7,13).
In contrast to the other cases reported, where the
mass usually presents with cystic changes (2,6,7,9,10),
the masses in the present study were markedly and heterogeneously
enhanced, whereas necrotic and liquefied non-enhanced areas were
found in the center of the mass with an irregular, well-defined
margin. CT manifestations of this lesion resembled that of other
neoplasms located in the anterior mediastinum, such as
intrathoracic goiter, malignant thymic neoplasm and teratoma. It is
difficult to differentiate between these lesions on CT. Malignant
thymic neoplasm often appears as a solid mass without cystic
changes and result in pleural or pericardiac effusion due to
invasion of the tumor (14).
Intrathoracic heterotopic thyroid gland and teratoma have similar
CT features to ectopic pancreas, which appear as clear enhancement
(15). Although, the goiter is
derived from cervical thyroid gland, and the majority is located at
a relatively high level in the anterosuperior mediastinum, and
tends to extend to one side of the mediastinum (15). The anatomic association between the
intrathoracic mass and the cervical thyroid gland may be confirmed
through a cervicothoracic serial scan. However, teratoma is derived
from pluripotent germ cells. Benign teratoma is often cystic, while
malignant teratoma is usually solid. There are numerous components
in a teratoma due to its various blastodermal origins, including
lipids, bone tissues, teeth and hair. Therefore, a final diagnosis
of teratoma can be made when these tissues are observed in the
tumor (6).
In conclusion, ectopic pancreas in the mediastinum
is extremely rare. When there is a mass in the anterior mediastinum
with marked and heterogeneous enhancement, along with necrotic and
liquefied non-enhanced areas in the center, ectopic pancreas should
be considered and differentiated from other neoplasms in this
region.
References
|
1
|
Klob J: Pancreas accessorium. Zeitschrift
der Kaiserl. Königl. Gesellschaft der Aerzte zu Wien.
15:7321859.(In German).
|
|
2
|
Szabados S, Lénárd L, Tornóczky T, et al:
Ectopic pancreas tissue appearing in a mediastinal cyst. J
Cardiothorac Surg. 7:222012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Byun CS, Park IK, Kim H and Yu W: Ectopic
pancreas with hemorrhagic cystic change in the anterior
mediastinum. Korean J Thorac Cardiovasc Surg. 45:131–133. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
St Romain P, Muehlebach G, Damjanov I and
Fan F: Adenocarcinoma arising in an ectopic mediastinal pancreas.
Ann Diagn Pathol. 16:494–497. 2012.PubMed/NCBI
|
|
5
|
Takemura M, Yoshida K and Morimura K:
Thoracoscopic resection of thoracic esophageal duplication cyst
containing ectopic pancreatic tissue in adult. J Cardiothorac Surg.
6:1182011. View Article : Google Scholar
|
|
6
|
Chen ZH, Yu RS, Dong F and Wang XJ: CT
findings of an ectopic pancreas in the anterior mediastinum. Korean
J Radiol. 10:527–530. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang W, Li K, Qin W, et al: Ectopic
pancreas in mediastinum: report of two cases and review of the
literature. J Thorac Imaging. 22:256–258. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Al-Salam S and Al Ashari M: Ectopic
pancreatic tissue in the anterior mediastinum. Virchows Arch.
448:661–663. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tamura Y, Takahama M, Kushibe K and
Taniguchi S: Ectopic pancreas in the anterior mediastinum. Jpn J
Thorac Cardiovasc Surg. 53:498–501. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cagirici U, Ozbaran M, Veral A and
Posacioglu H: Ectopic mediastinal pancreas. Eur J Cardiothorac
Surg. 19:514–515. 2001. View Article : Google Scholar
|
|
11
|
Perez-Ordonez B, Wesson DE, Smith CR and
Asa SL: A pancreatic cyst of the anterior mediastinum. Mod Pathol.
9:210–214. 1996.PubMed/NCBI
|
|
12
|
Carr MJ, Deiraniya AK and Judd PA:
Mediastinal cyst containing mural pancreatic tissue. Thorax.
32:512–516. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Makhlouf HR, Almeida JL and Sobin LH:
Carcinoma in jejunal pancreatic heterotopias. Arch Pathol Lab Med.
123:707–711. 1999.PubMed/NCBI
|
|
14
|
Benveniste MF, Rosado-de-Christenson ML,
Sabloff BS, et al: Role of imaging in the diagnosis, staging, and
treatment of thymoma. Radiographics. 31:1847–1861. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Laurent F, Latrabe V, Lecesne R, et al:
Mediastinal masses: diagnostic approach. Eur Radiol. 8:1148–1159.
1998. View Article : Google Scholar : PubMed/NCBI
|