Introduction
Periosteal chondrosarcoma is an extremely rare and
low-grade malignant cartilaginous tumor arising from the external
surface of bones (1), and it
accounts for <2% of all chondrosarcomas (2). Wide resection is the only recommended
treatment, as it minimizes the potential for recurrence and
metastases (3–6). Therefore, the pre-operative diagnosis
of periosteal chondrosarcoma is important. However, periosteal
chondrosarcomas can be difficult to differentiate from benign
periosteal chondromas, since these two conditions share features on
imaging and histological examination (5).
Fluorine-18 fluorodeoxyglucose (18F-FDG)
positron emission tomography (PET) is a diagnostic imaging
technique that detects glucose uptake by cells with high metabolic
activity, including the heart, brain and tumor cells. The
usefulness of PET has been reported in diagnosing malignant
cartilaginous tumors, particularly those with borderline
histological, imaging and clinical characteristics (7–9).
Feldman et al (7) reported
that a maximum standard uptake value (SUVmax) cut-off of
2.0 could be used to distinguish benign from malignant
cartilaginous tumors. However, there have been no reports on the
use of PET for diagnosing periosteal chondrosarcoma due to the
rarity of this condition.
The present study reports a case of femoral
periosteal chondrosarcoma that was diagnosed by PET/computed
tomography (CT). Written consent was obtained from the patient and
the patient’s family for the publication of this study.
Case report
A 40-year-old female presented with an 18-month
history of a tender mass in the left distal femur. Physical
examination revealed a bony hard mass in the medial aspect of the
metaphysis in the distal femur.
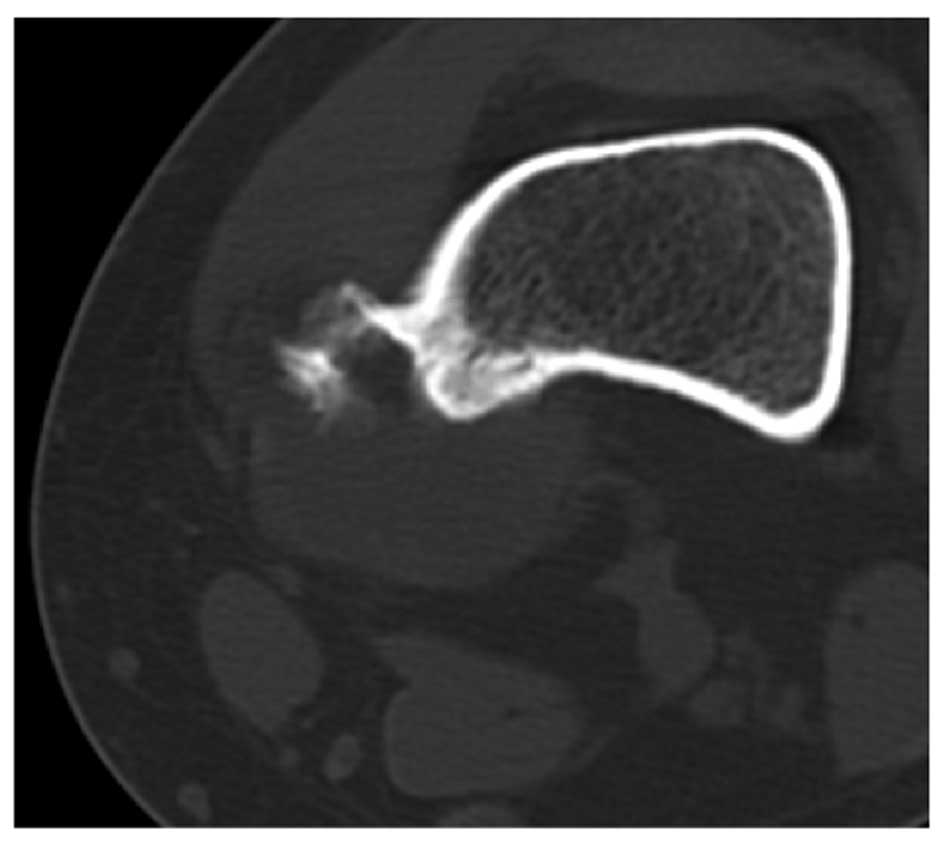
Radiography revealed a well formed sclerotic
periosteal reaction, indicating periosteal buttressing (Fig. 1). CT images clearly revealed a tumor
containing calcific densities characteristic of the external bone
surface, which was a juxtacortical lesion associated with a
thickened cortex. The tumor had no connection with bone marrow and
a periosteal tumor was suspected (Fig.
2). Magnetic resonance imaging (MRI) revealed a sharply
delineated mass at the bone surface, measuring 3 cm in diameter. An
area of low to intermediate signal intensity was present on
T1-weighted images. On T2-weighted images, the tumor had a bright
signal and an associated lobulated structure with hypo-intense
septa. Gadolinium-enhanced T1-weighted images revealed peripheral
and septal enhancement. No intramedullary extension or edema was
identified. MRI findings indicated a chondrogenic tumor at the
external bone surface, which again suggested a periosteal chondroma
or a periosteal chondrosarcoma (Fig.
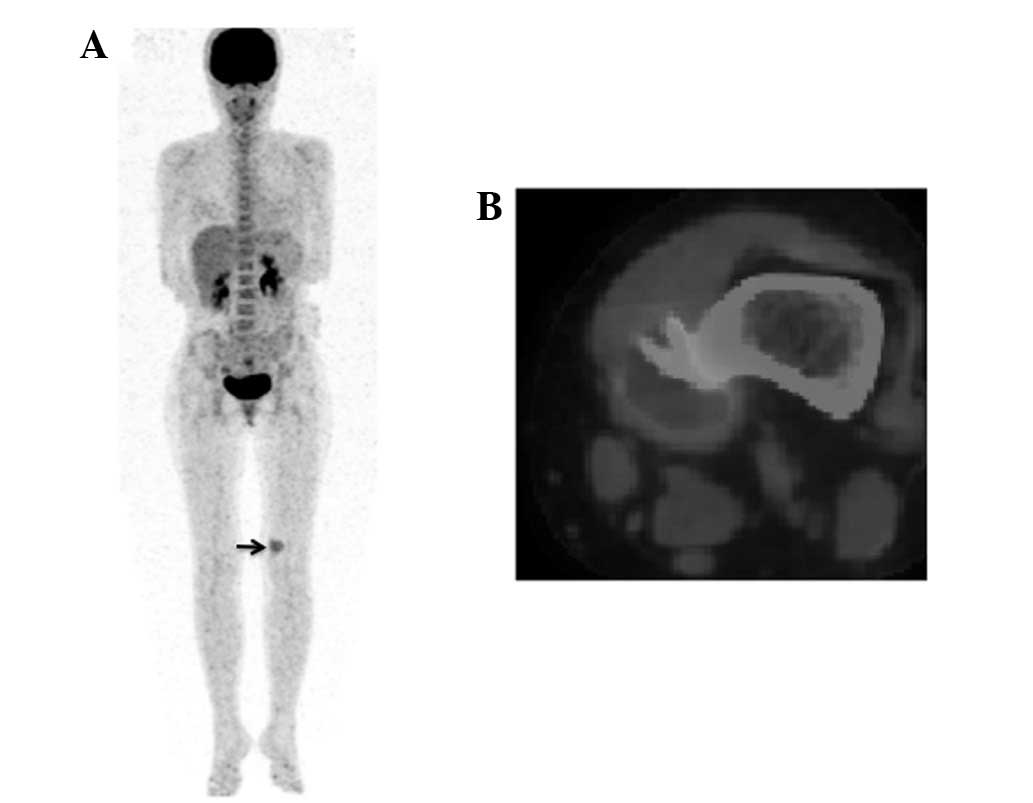
3). PET images revealed abnormal 18F-FDG uptake in
the distal aspect of the femur. Furthermore, PET/CT images clearly
demonstrated periosteal buttressing with an abnormal
18F-FDG SUVmax of 2.7, indicating a malignant
tumor of the bone surface in the distal femur. In addition, no
evidence of distant metastases was identified (Fig. 4).
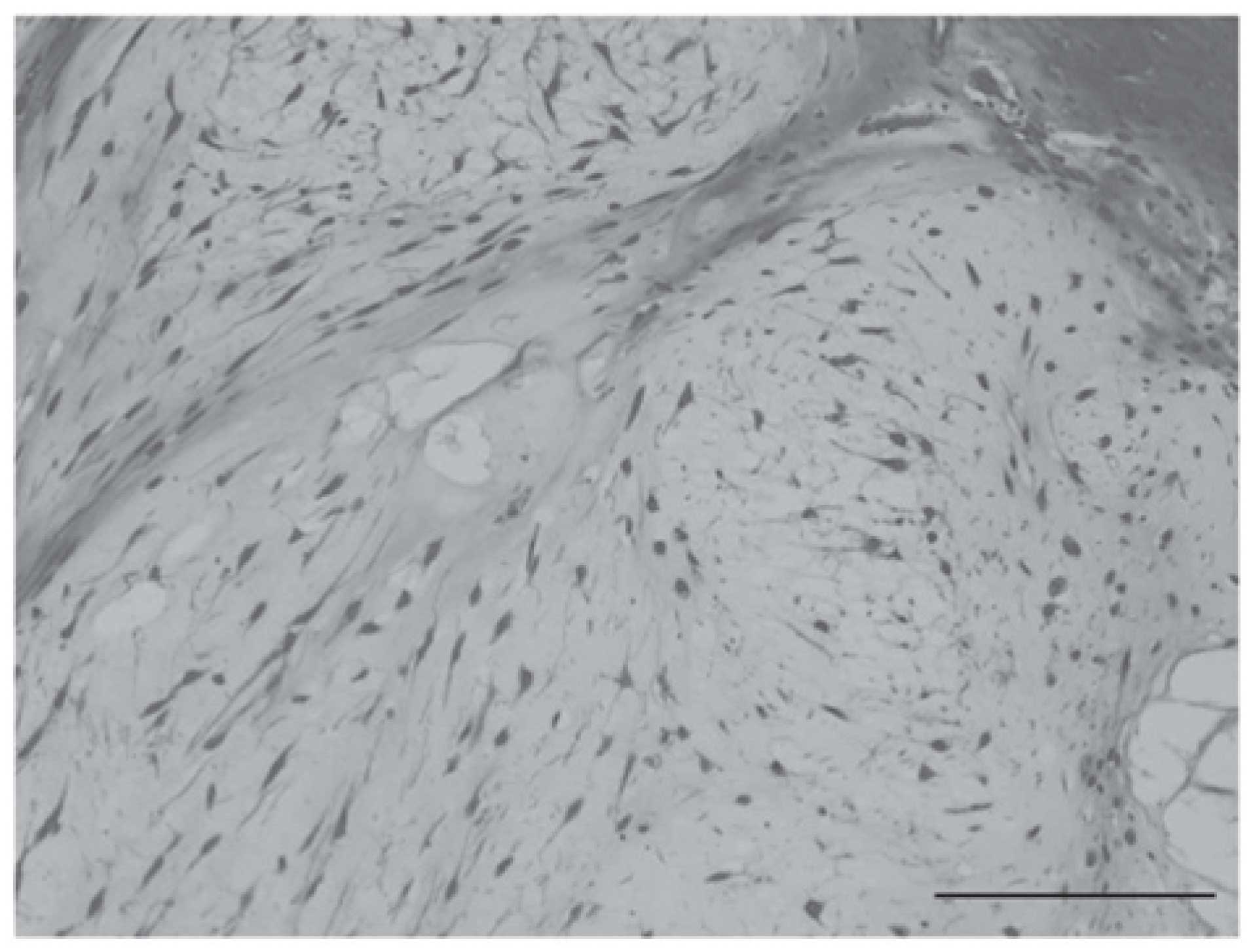
En bloc resection of the tumor was performed with a
wide margin. The histology of the resected sample demonstrated
variant forms of nuclei, the appearance of cells with two nuclei,
and cytostromatic changes such as myxoma. Periosteal chondrosarcoma
grade II was diagnosed (Fig.
5).
The patient started walking on the day following
surgery. Neither recurrence nor metastases have been identified in
the 3 years following surgery.
Discussion
Periosteal chondrosarcoma presents in the second to
fourth decade of life as a slowly growing painless mass. The most
common site of this tumor is the distal femur, followed by the
proximal humerus. The size is generally >5 cm (3). Radiographic features are cortical
saucerization, cortical thickening, cortical marginal buttressing
and a soft tissue mass that may contain matrix calcification
(10). Invasion of the medullary
cavity is infrequent, but has been previously described (5,11). In
the treatment of this condition, wide resection is essential since
the rates of recurrence and metastases are higher for patients
treated with intralesional or marginal excisions than for patients
treated with wide resection. Papagelopoulos et al (2) reported that the 5-year local
recurrence-free survival rate was lower in patients treated with
intralesional or marginal excisions (25%) than for patients treated
with wide resections (93%). In addition, the 5-year metastasis-free
survival rate was lower for patients who underwent intralesional or
marginal excisions (50%) than for patients who were treated by wide
resection (100%).
Periosteal chondroma is the benign counterpart of
periosteal chondrosarcoma. Periosteal chondroma is generally a
smaller painless mass <3 cm in size. Local excision is
sufficient treatment for chondromas (5). The preoperative differentiation of the
conditions is thus important, since the treatments differ.
Radiographically, periosteal chondrosarcoma and
periosteal chondroma appear as a saucer-shaped defect with
thickening and sclerosis of the underlying cortex. Periosteal
chondrosarcoma may invade the underlying cortex and medullary
cavity, while medullary invasion is not observed with periosteal
chondromas (12–14). Robinson et al (5) reported that size is the most reliable
indicator for distinguishing the two conditions. Periosteal
chondromas are typically small (1–6.5 cm; median, 2.5 cm), whereas
periosteal chondrosarcomas tend to be larger (3–14 cm; median, 4
cm). In the present case, the lesion measured ~3 cm in size with no
invasion into the underlying cortex and medullary cavity. It was
challenging to differentiate periosteal chondrosarcoma from
periosteal chondroma on the basis of size and the radiological and
MRI findings alone.
Previous studies have reported that PET is a useful
imaging method for differentiating between benign and malignant
cartilaginous tumors (7–9). An SUVmax cut-off of 2.0 can
be used to distinguish benign from malignant cartilaginous tumors
with 90.9% overall sensitivity, 100% specificity and 96.6% accuracy
(7). Lee et al (9) reported that grade I chondrosarcoma is
difficult to differentiate from chondroma. However, an
SUVmax cut-off of 2.3 was useful in differentiating
grade II or III chondrosarcomas from chondroma and grade I
chondrosarcomas. The positive predictive value was 0.82 (95%
confidence interval, 0.48–0.97), and the negative predictive value
was 0.96 (95% confidence interval, 0.77–1.00).
In the present case, the typical findings of
periosteal chondrogenic tumor were identified by radiography, CT
and MRI. However, none of these findings could clearly
differentiate periosteal chondrosarcoma from periosteal chondroma.
However, given the SUVmax of 2.7, PET/CT was able to
indicate malignancy. Consequently, a periosteal chondrosarcoma of
grade II or III was diagnosed and wide resection was therefore
carried out. In conclusion, PET/CT can distinguish periosteal
chondrosarcoma from periosteal chondroma, even where
differentiation of the conditions is challenging on the basis of
size and radiographical findings.
Acknowledgements
In support of preparation of this manuscript, one of
the authors (HF) received a grant from the Fund of the Ministry of
Education, Culture, Sports, Science and Technology, Japan.
References
|
1
|
Schajowicz F: Juxtacortical
chondrosarcoma. J Bone Joint Surg Br. 59-B:473–480. 1977.PubMed/NCBI
|
|
2
|
Papagelopoulos PJ, Galanis EC, Mavrogenis
AF, et al: Survivorship analysis in patients with periosteal
chondrosarcoma. Clin Orthop Relat Res. 448:199–207. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kenan S, Abdelwahab IF, Klein MJ, Hermann
G and Lewis MM: Lesions of juxtacortical origin (surface lesions of
bone). Skeletal Radiol. 22:337–357. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Papagelopoulos PJ, Galanis EC, Boscainos
PJ, Bond JR, Unni KK and Sim FH: Periosteal chondrosarcoma.
Orthopedics. 25:839–842. 2002.PubMed/NCBI
|
|
5
|
Robinson P, White LM, Sundaram M, et al:
Periosteal chondroid tumors: radiologic evaluation with pathologic
correlation. AJR Am J Roentgenol. 177:1183–1188. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nojima T, Unni KK, McLeod RA and Pritchard
DJ: Periosteal chondroma and periosteal chondrosarcoma. Am J Surg
Pathol. 9:666–677. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Feldman F, Van Heertum R, Saxena C and
Parisien M: 18FDG-PET applications for cartilage
neoplasms. Skeletal Radiol. 34:367–374. 2005. View Article : Google Scholar
|
|
8
|
Aoki J, Watanabe H, Shinozaki T, Tokunaga
M, Inoue T and Endo K: FDG-PET in differential diagnosis and
grading of chondrosarcomas. J Comput Assist Tomogr. 23:603–608.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lee FY, Yu J, Chang SS, Fawwaz R and
Parisien MV: Diagnostic value and limitations of fluorine-18
fluorodeoxyglucose positron emission tomography for cartilaginous
tumors of bone. J Bone Joint Surg Am. 86-A:2677–2685. 2004.
|
|
10
|
Kumta SM, Griffith JF, Chow LT and Leung
PC: Primary juxtacortical chondrosarcoma dedifferentiating after 20
years. Skeletal Radiol. 27:569–573. 1998.PubMed/NCBI
|
|
11
|
Hatano H, Ogose A, Hotta T, Otsuka H and
Takahashi HE: Periosteal chondrosarcoma invading the medullary
cavity. Skeletal Radiol. 26:375–378. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Brien EW, Mirra JM and Luck JV Jr: Benign
and malignant cartilage tumors of bone and joint: their anatomic
and theoretical basis with an emphasis on radiology, pathology and
clinical biology. II Juxtacortical cartilage tumors. Skeletal
Radiol. 28:1–20. 1999. View Article : Google Scholar
|
|
13
|
Robbin MR and Murphey MD: Benign chondroid
neoplasms of bone. Semin Musculoskelet Radiol. 4:45–58. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sinha S, Singhania GK and Campbell AC:
Periosteal chondroma of the distal radius. J Hand Surg Br.
24:747–749. 1999. View Article : Google Scholar : PubMed/NCBI
|