Introduction
Previous cytogenetic studies have revealed that
complex genetic changes occur in leiomyosarcoma (LMS). Numerical
aberrations and structural rearrangements in all chromosomes have
been reported in LMS (1,2). No specific primary cytogenetic
abnormality characteristics of LMS have been identified, although,
consistent chromosomal profiles have been observed and an attempt
at a chromosomal classification has been made (1). Recent advances in mapping resolution
using array-based comparative genomic hybridization (array CGH)
have significantly improved the resolving power in comparison with
that of metaphase CGH (3,4). This has provided more information
regarding the complexity and exact locations of genomic
rearrangements, which result in DNA copy number alterations
(DCNAs). Using array CGH, it has previously been reported that an
increase in DCNAs is associated with tumor size in LMS (5).
As a morphological variant of LMS, pleomorphic LMS
(P-LMS) was initially described as an important differential
diagnosis of pleomorphic malignant fibrous histiocytoma by Fletcher
in 1992 (6). Subsequently, various
studies have examined a series of P-LMS using morphological,
immunohistochemical and electron microscopy methods, establishing
the occurrence of this variant (7–9).
However, cytogenetic and molecular genetic data for P-LMS have not
previously been described. Therefore, the current study reports the
DCNA observations for a primary tumor and metastatic lymph node in
a patient presenting with P-LMS.
Case report
A 31-year-old male presented with a mass in the left
axilla, which had rapidly enlarged over the previous two months
prior to admission to the University Hospital of Toyama (Toyoma,
Japan). The patient had an unremarkable clinical history. On
examination, a 10×9 cm elastic hard mass, presenting with
tenderness, was identified. Neurovascular examination results and
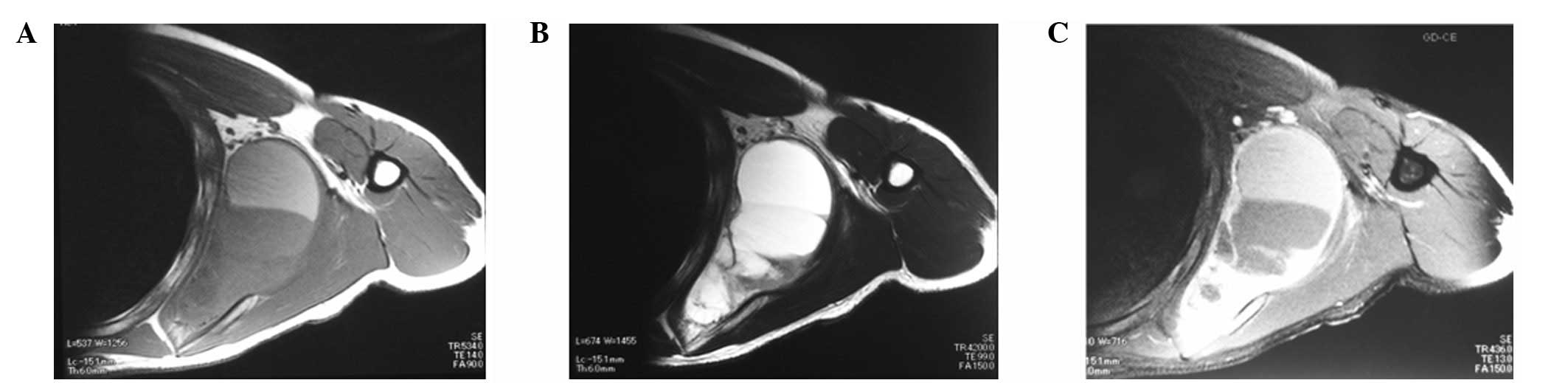
laboratory observations were relatively normal. T1- and T2-weighted
magnetic resonance imaging showed a large cystic tumor with
fluid-fluid levels, indicative of a soft tissue sarcoma (Fig. 1). Angiograms revealed that the tumor
was hypervascular.
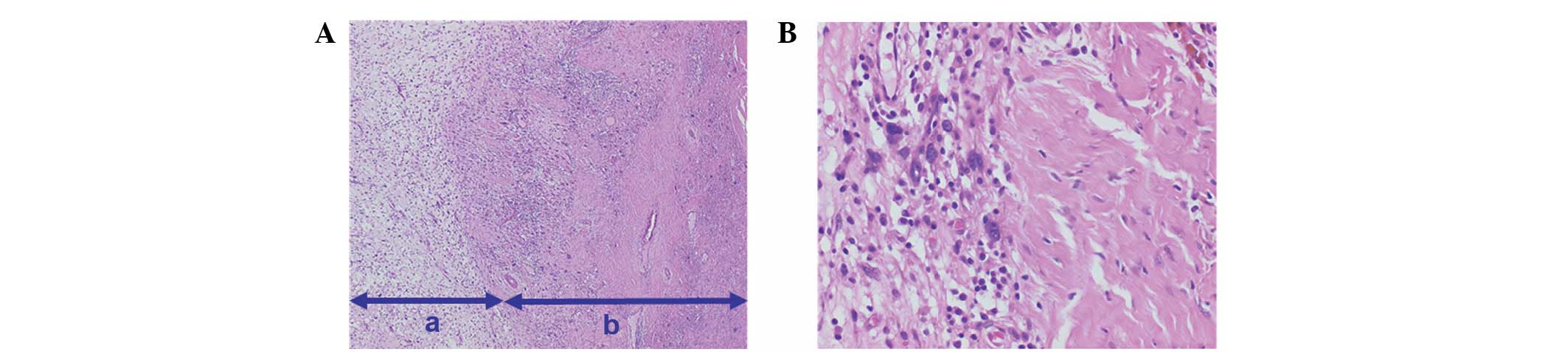
An open tumor biopsy was performed and the pathology
was determined as a P-LMS (Fig. 2).
Following preoperative chemotherapy for two days with doxorubicin
(40 mg/day) and ifosfamide (4 g/day), the tumor was surgically
resected. Gross examination of the resected specimen showed an
elastic firm and tan-to-yellow mass; its largest diameter was 14
cm. The tumor had a large cyst that contained a brown serous fluid.
An enlarged regional lymph node (metastasis) was also resected.
Microscopically, the tumor consisted of myxomatous
and pleomorphic areas with proliferating ovoid or short-spindle
atypical cells and a number of mitotic figures were observed
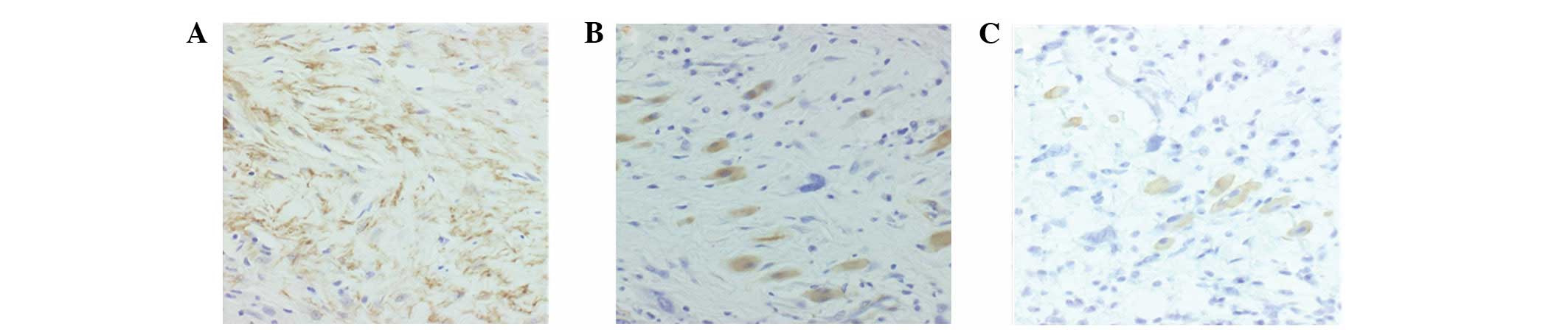
(Fig. 2). Immunohistochemistry
revealed that the tumor cells were positive for vimentin,
h-caldesmon and muscle actin (HHF-35; Fig. 3), with slight positivity for smooth
muscle actin (SMA). However, these cells were negative for desmin,
S-100, cluster of differentiation (CD)31, CD34, CD56, CD99,
cytokeratin, c-kit, calretinin and p53 (DakoCytomation, Copenhagen,
Denmark).
The tumor specimens were frozen and stored at −80°C
until the CGH analysis was conducted. Genomic DNA was isolated from
a tumor sample by standard procedures using proteinase K digestion
and phenol-chloroform extraction (10,11).
Hybridization and analysis by array CGH were performed according to
the manufacturer’s instructions (Vysis-Abbott Japan, Inc., Tokyo,
Japan). The array CGH comprised of 287 clones that included
important tumor suppressors and oncogene loci. Tumor DNA (n=100)
was labeled by random priming with fluorescent-labeled cy3-dUTP
(Perkin-Elmer, Waltham, MA, USA) and normal reference DNA (n=100)
was labeled with cy5-dUTP. The tumor and control DNAs were mixed
with Cot-1 DNA (Vysis-Abbott Japan, Inc.), precipitated and
resuspended in a microarray hybridization buffer, which contained
50% formamide. The hybridization solution was heated to 80°C for 10
min to denature the DNA and subsequently incubated for 1 h at 37°C.
Hybridization was performed for 72 h in a moist chamber, followed
by post-hybridization washing in a 50% formamide/2× saline sodium
citrate buffer at 45°C. Slides were mounted in phosphate-buffered
saline containing 4′,6-diamidino-2-phenylindole (array DAPI
solution). Fluorescence intensity images were captured from the
hybridized microarray slides using a GenoSensor Reader System
equipped with Array 300 Software (Vysis-Abbott Japan, Inc.). The
total intensity and intensity ratio of the two dyes for each spot
were automatically calculated. The diagnostic cut-off levels
representing the gains and losses of the DCNAs were set to an upper
threshold of 1.25 and a lower threshold of 0.75.
The current study was approved by the Institutional
Review Board for Human Use of the University Hospital of Toyama.
Written informed consent for the publication of the patient’s data
was obtained from the patient.
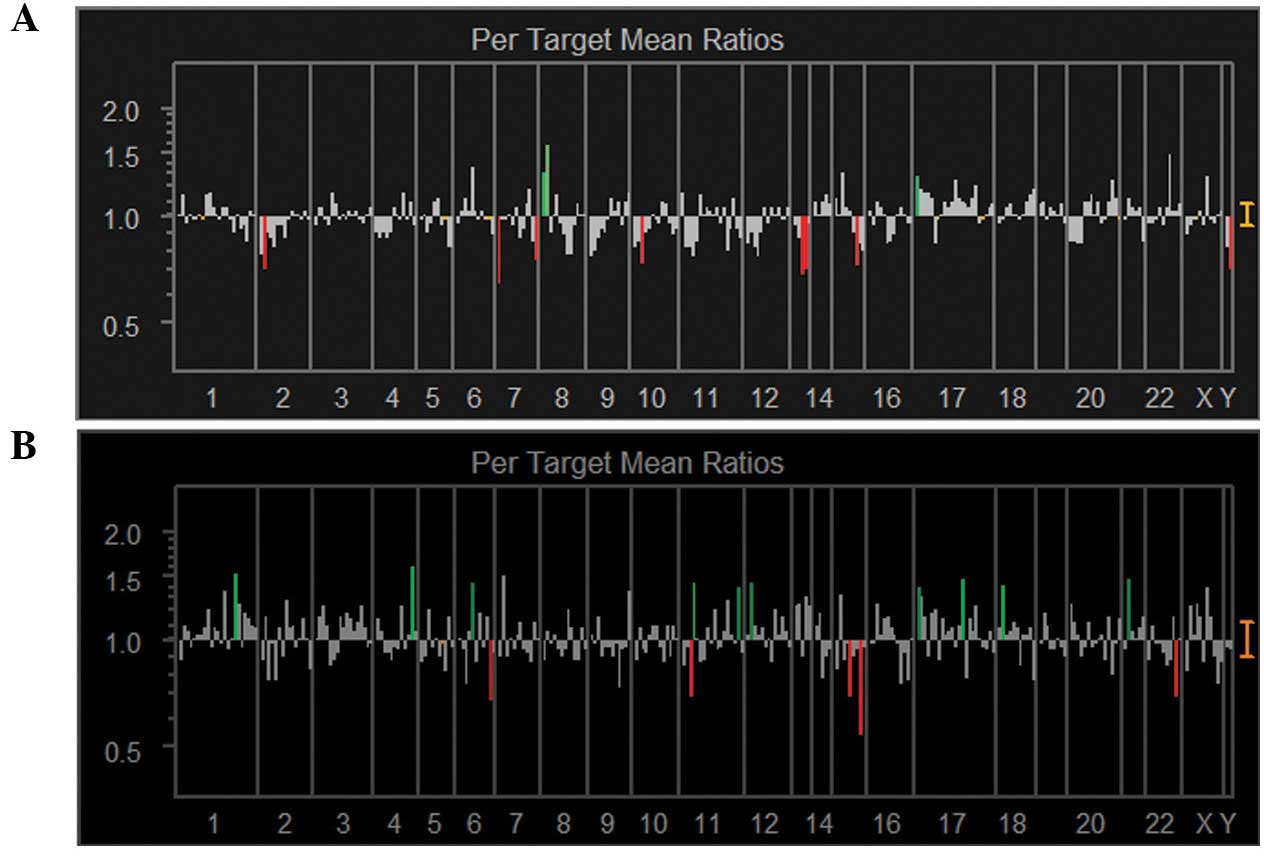
The genetic instabilities of the primary tumor and
metastatic lymph node were analyzed and compared in the present
study. The DCNAs of all chromosomes were determined (Fig. 4). DCNAs that exhibited marked gains
(1.25) or losses (0.75) were selected and are listed in Table I. Of the 287 clones represented on
array CGH, the primary tumor showed four DCNAs (1.4%) with gains
and nine DCNAs (3.1%) with losses. In comparison, the metastatic
lymph node showed 11 DCNAs (3.8%) with gains and six DCNAs (2.1%)
with losses. Genetic aberrations in the metastatic lesion were
increased compared with the primary lesion. Only one DCNA, 17ptel
(282M15/SP6), was increased in the two samples.
 | Table ISummary of DCNA data in the current
case of pleomorphic LMS. |
Table I
Summary of DCNA data in the current
case of pleomorphic LMS.
| A, Gain |
|---|
|
|---|
| Primary tumor | Lymph node
metastasis |
|---|
|
|
|---|
| Gene name | Locus | DCNAs | Gene name | Locus | DCNAs |
|---|
| D8S504 | 8p tel | 1.31 | WI-5663,
WI-13414 | 1q21 | 1.54 |
| D8S596 | 8p tel | 1.56 | 4QTEL11 | 4q tel | 1.59 |
|
282M15/SP6 | 17p tel | 1.29 | HTR1B | 6q13 | 1.44 |
| NF1 3′ | 17q11.2 | 1.26 |
CDKN1C(p57) | 11p15.5 | 1.45 |
| | | WI-6509 | 11q tel | 1.39 |
| | | SHGC-5557 | 12p tel | 1.44 |
| | | SNRPN | 15q12 | 1.34 |
| | |
282M15/SP6 | 17p tel | 1.39 |
| | |
PPARBP(PBP) | 17q12 | 1.48 |
| | | SHGC17327 | 18p tel | 1.42 |
| | |
RUNX1(AML1) | 21q22.3 | 1.49 |
|
| B, Loss |
|
| Primary tumor | Lymph node
metastasis |
|
|
| Gene name | Locus | DCNAs | Gene name | Locus | DCNAs |
|
| 2PTEL27 | 2p tel | 0.72 | ESR1 | 6q25.1 | 0.69 |
| G31341 | 7p tel | 0.65 | HRAS | 11p15.5 | 0.71 |
| 7QTEL20 | 7q tel | 0.76 | MAP2K5 | 15q23 | 0.70 |
|
D10S249,D10S533 | 10p15 | 0.75 | PACE4C | 15q tel | 0.55 |
|
CDKN1B(p27) | 12p13.1-p12 | 0.78 | stSG30213 | 16q tel | 0.78 |
| D13S319 | 13q14.2 | 0.69 | ARSA | 22q tel | 0.71 |
| D13S25 | 13q14.3 | 0.72 | | | |
| IGF1R | 15q25–q26 | 0.74 | | | |
| AZFa
region | Yq11 | 0.72 | | | |
The current study focused on the gain of 8ptel
(D8S504 and D8S596) and the loss of 13q14.2-14.3
(D13S319 and D13S25) in the primary tumor, since
these loci showed marked changes on the two different arrays for
the same locus. These DCNAs may provide various starting points for
identifying candidate genes that are associated with oncogenesis.
However, these genetic changes were not observed in the metastatic
lymph node (Table I).
Discussion
Analysis of DCNAs to identify the molecular events
in soft tissue sarcomas is important. Array CGH technology
(3,4) enables the detection of specific genes
with DCNAs and may be used to screen for genomic imbalances in
human solid cancers. The key biological value of high-resolution
array CGH is its ability to detect small amplicons and deletions
that potentially harbor specific oncogenes or suppressor genes.
P-LMS is usually defined by an association between
areas of undifferentiated pleomorphic sarcoma and areas showing
morphological, immunohistochemical or ultrastructural evidence of
smooth muscle differentiation. SMA, desmin and HHF-35 are specific
to smooth muscle. The novel marker, h-caldesmon, is highly specific
for smooth muscle differentiation, however, is expressed in only
40% of cases (9). To date, CGH
analysis has not been performed to differentiate LMS subtypes.
Therefore, we were unable discuss P-LMS DCNAs from previous
reports.
Riva et al (12) previously identified a 19p deletion
in a single case of recurring LMS. In addition, a previous CGH
analysis of 28 cases of LMS (13)
reported that a 13q14–q21 loss and 5p14-pter gain at diagnosis may
be used to identify patients with LMS who are likely to have
reduced survival times. The most frequent losses detected were 10q
(20 cases; 69%) and 13q (17 cases; 59%), the most frequent gain
that was detected was 17p (16 cases; 55%), and the high-level
amplifications that were detected were 17p (seven cases; 24%) and
8q (six cases; 21%). These observations may indicate early changes
during LMS tumorigenesis.
The array CGH analysis results of the current study
for a primary tumor indicated that the 8ptel (D8S504 and
D8S596) gain and 13q14.2-3 (D13S319 and
D13S25) loss were target genes. The loss of 13q14.2-3 has
been reported previously (13). The
most marked changes (1.25 or 0.75) in the metastatic tumor occurred
in 17 DCNAs. Among these loci, WI-5663 (1q21),
SHGC-5557 (12ptel), 282M15/SP6 (17ptel) and
RUNX1 (21q22.3) were observed in our previously reported
case of metastatic osteosarcoma (10).
The current study reports the DCNA observations for
a primary tumor and metastatic lymph node in a patient with P-LMS.
The gain of 8ptel (D13S319) and the loss of 13q14.2-14.3
(D13S25) may be involved in tumor progression and
metastasis. However, further cytogenetic study is required to
elucidate the DCNAs in P-LMS.
Acknowledgements
The authors would like to thank Akimi Sano from the
Department of Orthopaedics (University of Toyama, Toyoma, Japan)
who provided technical advice. The current study was partly
supported by a Grant-in-Aid for Scientific Research from the Japan
Society for the Promotion of Science (grant no. 22501043).
References
|
1
|
Sandberg AA and Bridge JA:
Leiomyosarcomas. The Cytogenetics of Bone and Soft Tissue Tumors.
RG Landes Company; Austin, TX: pp. 104–124. 1994
|
|
2
|
Sreekantaiah C, Davis JR and Sandberg AA:
Chromosomal abnormalities in leiomyosarcomas. Am J Pathol.
142:293–305. 1993.PubMed/NCBI
|
|
3
|
Pinkel D, Segraves R, Sudar D, et al: High
resolution analysis of DNA copy number variation using comparative
genomic hybridization to microarrays. Nat Genet. 20:207–211. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pollack JR, Perou CM, Alizadeh AA, et al:
Genome-wide analysis of DNA copy-number changes using cDNA
microarrays. Nat Genet. 23:41–46. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
El-Rifai W, Sarlomo-Rikala M, Knuutila S
and Miettinen M: DNA copy number changes in development and
progression in leiomyosarcomas of soft tissues. Am J Pathol.
153:985–990. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fletcher CD: Pleomorphic malignant fibrous
histiocytoma: fact or fiction? A critical reappraisal based on 159
tumors diagnosed as pleomorphic sarcoma. Am J Surg Pathol.
16:213–228. 1992. View Article : Google Scholar
|
|
7
|
Schürch W, Bégin LR, Seemayer TA, et al:
Pleomorphic soft tissue myogenic sarcomas of adulthood: A
reappraisal in the mid-1990s. Am J Surg Pathol. 20:131–147.
1996.PubMed/NCBI
|
|
8
|
Yamamoto I, Oshiro Y, Fukuda T and
Tsuneyoshi M: Pleomorphic leiomyosarcoma of the soft parts: a
reassessment by histology and immunohistochemistry of pleomorphic
soft tissue sarcomas. Oncol Rep. 6:533–537. 1999.
|
|
9
|
Oda Y, Miyajima K, Kawaguchi K, et al:
Pleomorphic leiomyosarcoma: clinicopathologic and
immunohistochemical study with special emphasis on its distinction
from ordinary leiomyosarcoma and malignant fibrous histiocytoma. Am
J Surg Pathol. 25:1030–1038. 2001. View Article : Google Scholar
|
|
10
|
Yasuda T, Kanamori M, Nogami S, et al:
Establishment of a new human osteosarcoma cell line, UTOS-1:
cytogenetic characterization by array comparative genomic
hybridization. J Exp Clin Cancer Res. 28:262009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kanamori M, San A, Yasuda T, Hori T and
Suzuki K: Array-based comparative genomic hybridization for
genomic-wide screening of DNA copy number alterations in aggressive
bone tumors. J Exp Clin Cancer Res. 31:1002012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Riva P, Dalprá L, Gualandri V, et al: 19p
deletion in recurring leiomyosarcoma lesions from the same patient.
Cancer Genet Cytogenet. 119:102–108. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang R, Titley JC, Lu YJ, Summersgill BM,
Bridge JA, Fisher C and Shipley J: Loss of 13q14-q21 and gain of
5p14-pter in the progression of leiomyosarcoma. Mod Pathol.
16:778–785. 2003. View Article : Google Scholar : PubMed/NCBI
|