Introduction
The incidence of breast cancer is higher in elderly
patients (>65 years) when compared with younger patients (<65
years old), with the elderly being associated with an increased
mortality risk (1). For elderly
patients, age-related factors must be considered when prescribing
the cancer treatment and supportive care. These factors include
organ function, comorbidity, consumption of other medication and
cognitive function. In this type of patient, quality of life
remains a primary objective for the clinician. In the last decade,
a large quantity of research has provided support for the
importance and efficacy of chemotherapy for the treatment of
elderly patients with metastatic breast cancer (2).
However, previous data has implicated the role of
chemotherapy or radiotherapy in the development of second cancers
following adult or pediatric cancer (3). The delayed effects of treatment may be
modified by moderate or low-penetrance genetic traits or by
additional gene-environment and gene-gene interactions. As
variations in DNA repair genes appear to have a role in the
susceptibility to de novo cancer (4), it is likely that these variations
modify cancer risk following exposure to DNA-damaging agents,
including radio- and chemotherapeutic agents.
As yet, the identification of patient subgroups that
may possess a heightened susceptibility to developing cancer or
other adverse sequelae has not been systematically addressed.
However, an increase in cases of head and neck cancer (HNC) has
been observed in the elderly (5).
The development of squamous cell carcinoma of the
tongue may depend on various factors, which include the human
papilloma virus (HPV), alcohol consumption and smoking (6). In the present study we describe an
elderly patient who presented with advanced breast cancer that was
intensively treated, who subsequently developed a second cancer of
the tongue. Patient provided written informed consent.
Case report
In March 2005, an 81-year-old female smoker was
diagnosed at the Medical Oncology Unit of the San Giovanni di Dio
Hospital (Frattamaggiore, Italy) with advanced left breast cancer.
The tumor was characterized as estrogen and progesterone
receptor-positive, and human epidermal growth factor 2-positive.
The tumor was treated with numerous cycles of chemo- and hormonal
therapy and the cancer only progressed locally. The patient did not
show metastases to any sites during the follow-up period. The
patient received the following combination treatments:
Capecitabine, anastrozole, pegylated liposomal doxorubicin and
vinorelbine; trastuzumab and fulvestrant; docetaxel, gemcitabine
and trastuzumab; and capecitabine and lapatinib. In August 2011,
the patient presented with a painful nodule on the tongue, which
had been gradually increasing in size. The patient’s clinical
analysis identified an elevated leukocyte count
(19.32×103/μl in September 2011, with the level of
neutrophils above the normal range). This tumor progressed to
involve the floor of the mouth and the left border of the tongue.
The histological analysis determined that is had not originated as
a result of metastasis from the breast lesion; it was diagnosed as
a moderately differentiated squamous cell carcinoma. The patient
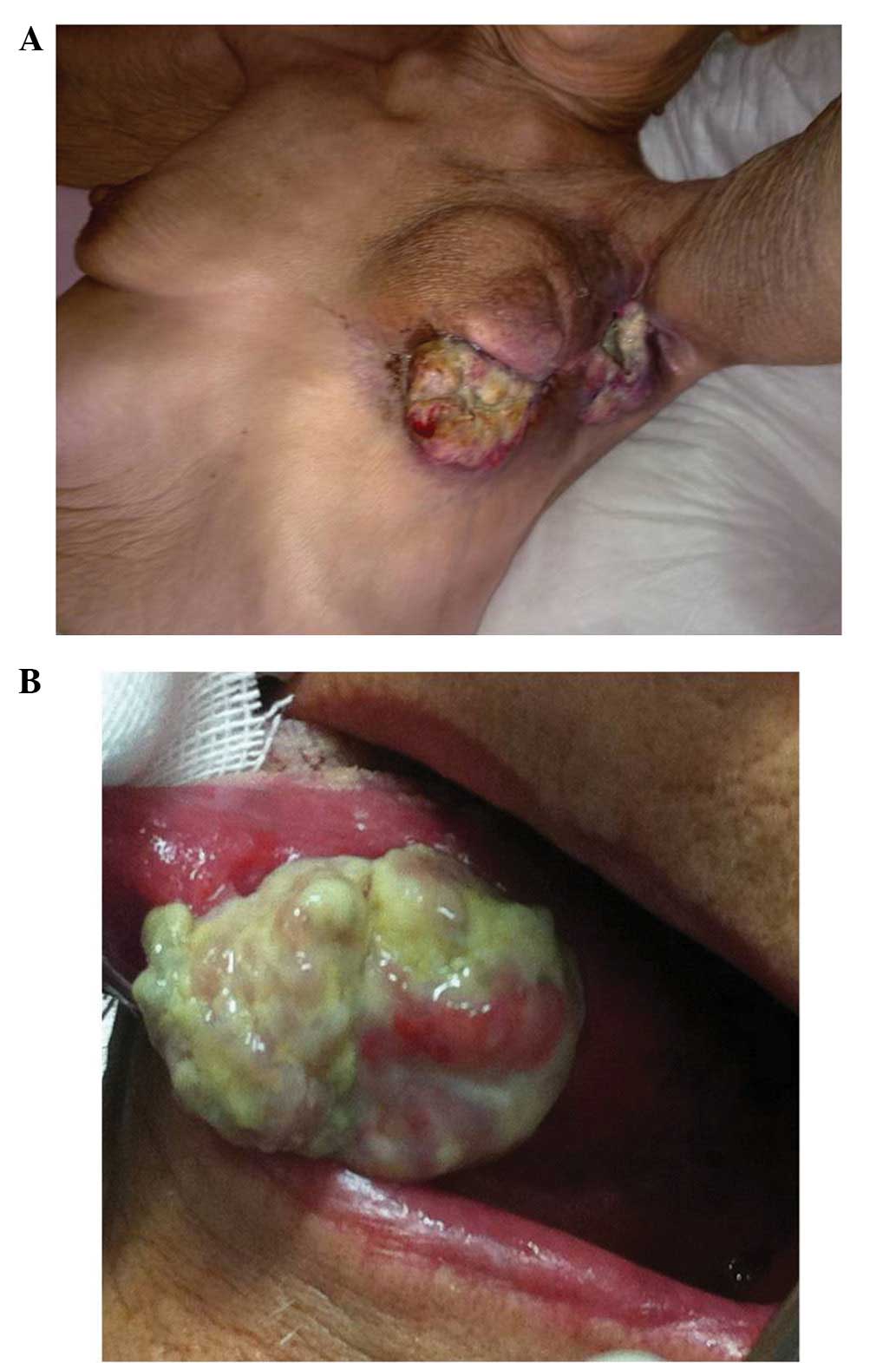
refused any local treatment and received only supportive care. The
involvement of the left breast and axilla by the breast cancer, and
the tongue cancer are demonstrated in Fig. 1A and B, respectively. The breast
cancer, despite its advanced status, was less complex to manage in
the elderly patient compared with the management of the tongue
tumor. The patient succumbed to the tongue cancer as a result of
bleeding, the associated anemia, and increasing problems with food
intake and cancer cachexia.
Discussion
Tobacco smoking and alcohol consumption are the
principal risk factors for developing tongue squamous cell
carcinoma (7). In addition, chewing
tobacco, radiation exposure, HPV, as well as immune deficiencies
have been implicated (8). The
prognosis for patients presenting with tongue cancer varies
depending on the stage and site.
The percentage of elderly people with HNC is rising
as a result of the increasing average lifespan; ~10% of HNC occur
in patients aged ≥80 years (5).
Management of this subpopulation has become a source of debate due
to the paucity of randomized data regarding the effect of age on
treatment response as well as morbidity associated with the
treatment of HNC. Furthermore, approximately two-thirds of HNC
patients present with locoregionally advanced stage (III and IV)
disease§. This requires multimodality therapy, including surgery,
radiation and/or chemotherapy. Elderly patients may not be suitable
for aggressive multimodality treatment due to their increased
comorbidity status, poor treatment tolerance and the toxicity of
treatments, such as radiotherapy and chemotherapy. The
Health-Related Quality of Life assessment is currently considered
to be one of the primary objectives of clinical research concerning
this subpopulation of patients (9).
Decision-making in the present case was based on the
patient’s characteristics and age, however, was also based on a
performance status evaluation, comorbidity and a patient-reported
outcomes assessment. This mode of conduct is similar to that which
was proposed in a recent study regarding geriatric patients with
HNC (10).
An additional case of a young female who presented
with tongue cancer that later developed into breast cancer was
identified in the literature (11).
In addition, the quantity of patients presenting with two types of
cancer, with oral cancer as the primary malignancy, is reportedly
on the rise (12).
In conclusion, in the present case, the origin of
the second cancer was unknown, however, the patient was an elderly
female who smoked, which may have been a possible cause of the
tongue tumor. Furthermore, previous chemotherapeutic treatment may
have been involved in predisposing the patient to develop the
second neoplasm. A possible mechanism is chemotherapy-induced
immunosuppression, which is a well-recognized cause of skin tumors,
specifically squamous cell carcinomas (13). The present case highlights the
influence of individual risk factors and chemotherapy-induced
immunosuppression in the selection of treatment for elderly cancer
patients to prevent the occurrence of a second cancer.
References
|
1
|
Yancik R, Wesley MN, Ries LA, Havlik RJ,
Edwards BK and Yates JW: Effect of age and comorbidity in
postmenopausal breast cancer patients aged 55 years and older.
JAMA. 285:885–892. 2001.
|
|
2
|
Spazzapan S, Crivellari D, Bedard P,
Lombardi D, Miolo G, Scalone S and Veronesi A: Therapeutic
management of breast cancer in the elderly. Expert Opin
Pharmacother. 12:945–960. 2011.
|
|
3
|
Oeffinger KC, Baxi SS, Novetsky Friedman D
and Moskowitz CS: Solid tumor second primary neoplasms: who is at
risk, what can we do? Semin Oncol. 40:676–689. 2013.
|
|
4
|
Berwick M and Vineis P: Markers of DNA
repair and susceptibility to cancer in humans: an epidemiologic
review. J Natl Cancer Inst. 92:874–897. 2000.
|
|
5
|
Siddiqui F and Gwede CK: Head and neck
cancer in the elderly population. Semin Radiat Oncol. 22:321–333.
2012.
|
|
6
|
Bello IO, Soini Y and Salo T: Prognostic
evaluation of oral tongue cancer: means, markers and perspectives
(I). Oral Oncol. 46:630–635. 2010.
|
|
7
|
Corcoran TP and Whiston DA: Oral cancer in
young adults. J Am Dent Assoc. 131:7262000.
|
|
8
|
Warnakulasuriya S: Global epidemiology of
oral and oropharyngeal cancer. Oral Oncol. 45:309–316. 2009.
|
|
9
|
Balducci L, Colloca G, Cesari M and
Gambassi G: Assessment and treatment of elderly patients with
cancer. Surg Oncol. 19:117–123. 2010.
|
|
10
|
Silveira AP, Gonçalves J, Sequeira T,
Ribeiro C, Lopes C, Monteiro E and Pimentel FL: Geriatric oncology:
comparing health related quality of life in head and neck cancer
patients. Head Neck Oncol. 3:32011.
|
|
11
|
Kousaka J, Fujii K, Yorozuya K, Mouri Y,
Yoshida M, Nakano S, Fukutomi T, Takahashi E and Yokoi T: A case of
quadruple primary malignancies including breast, tongue, and
thyroid cancers and osteosarcoma in a young female without
karyotype abnormality. Breast Cancer. May 12–2011.(Epub ahead of
print).
|
|
12
|
Ikawa H, Tonogi M, Yamane GY, Yamauchi T,
Tanaka Y, Sato M, Matsui J, Ando N and Katakura A: Upper
gastrointestinal tract cancers as double-cancers in elderly
patients with oral squamous cell carcinoma. Bull Tokyo Dent Coll.
53:9–16. 2012.
|
|
13
|
Rangwala S and Tsai KY: Roles of the
immune system in skin cancer. Br J Dermatol. 165:953–965. 2011.
|