Introduction
Angioleiomyoma, also termed vascular or dermal
angiomyoma, is an uncommon benign soft tissue tumor (1–3),
comprising approximately two-thirds of oral leiomyomas reported in
previous studies (4,5). The rarity of the tumor is likely due
to the paucity of smooth muscle in the oral cavity, the primary
source of smooth muscle being the tunica media of blood vessels
(6). The tumor normally manifests
as a painful solid mass on the extremities (in 89.0% of cases),
particularly below the knee; only 8.5% arise in the head and neck
(7,8). At present, <200 head and neck
angioleiomyomas have been previously reported, and they have tended
to present as painless masses of the venous or cavernous type
(1,7). Angioleiomyoma is difficult to diagnose
correctly from clinical manifestations and imaging alone, and a
biopsy is generally required (1,9).
Angioleiomyomas comprise vascular endothelial and
smooth muscle cells (2,10). Morimoto classified the tumors as
follows (7): i) Solid, the tumor
comprises closely compacted smooth muscle and abundant blood
vessels, which are small and slit-like. The smooth muscle bundles
surround the vessels and interdigitate with them; ii) venous, the
tumor lacks compacted smooth muscle bundles and the blood vessels
have thick muscular walls of varying size; iii) cavernous, the
tumor consists of numerous dilated vascular channels and smaller
quantities of smooth muscle bundles, which are difficult to
distinguish from the muscular walls of the vessel channels.
The present study retrospectively examined the
clinical features, characteristics and management of all head and
neck angioleiomyomas that were treated between 1978 and 2012 at the
West China Hospital of Stomatology, Sichuan University (Chengdu,
Sichuan, China). Where possible, archived tissue was subjected to
modern immunohistochemical diagnostic techniques.
Patients and methods
Patient records and analysis. In total, 21 patients
have been diagnosed with angioleiomyoma at the West China Hospital
of Stomatology over the past 34 years. The records of these
patients were examined and recorded, including data on age, gender,
presenting symptoms and their duration, clinical features,
investigations and method of diagnosis, tumor location and size,
original diagnosis and Morimoto’s pathological classification, and
subsequent management and surveillance (7). Archived paraffin blocks were cut and
stained with hematoxylin and eosin, Masson’s trichrome stain, Van
Gieson stain and immunohistochemical stain (avidin-biotin complex
method) to re-evaluate and confirm the diagnosis. For the
immunohistochemical analysis, anti-vimentin goat polyclonal
(sc-7557; Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA),
anti-CD34 mouse monoclonal (sc-7324, Santa Cruz, Biotechnology,
Inc.), anti-S-100 rabbit polyclonal (ab868; Abcam, Cambridge, UK),
anti-desmin rabbit polyclonal (ab32362; Abcam) and anti-α-actin
smooth muscle rabbit polyclonal (ab5694; Abcam) antibodies were
used. The present study followed the Declaration of Helsinki for
the medical protocol and was approved by the regional Ethical
Review Board of the West China Hospital of Stomatology.
Results
Distribution
The patients diagnosed with angioleiomyomas
accounted for 0.18% (21 out of 11,916) of all benign head and neck
tumors, 0.17% (four out of 2,413) of all benign salivary gland
tumors and 91.3% (21 out of 23) of all leiomyomas during the
34-year study period.
Clinical features
The clinical characteristics of the present cohort
and details of the disease are shown in Table I. Those diagnosed with
angioleiomyoma were predominantly male (male:female ratio,
1.625:1), with a mean age of 42.5 years. Approximately half (52.4%)
of cases were diagnosed in the fourth to sixth decades. Six tumors
were detected in the deep tissues, including four in the parotid
gland, one in the mandible and one in the neck. The remaining
tumors were located in the submucosal layer (12 cases) or the
dermis/subcutaneous layer of the skin (three cases). Tumors tended
to be solitary, mobile, firm, ovoid and well circumscribed, with a
smooth surface; only two were soft. Macroscopically, certain tumors
were brown with hemorrhagic areas on the surface. Others were light
red, similar to muscle. One patient had a painless ulcer on the
tumor surface (0.3 cm diameter). The majority of patients reported
no pain, with the exception of three patients who exhibited
spontaneous pain and three with tenderness; one reported pain and
tenderness (Table II). Two of the
patients who reported pain were also found to have nerve tissue
within the tumor (cases 8 and 20).
 | Table ICharacteristics of the 21-patient
cohort. |
Table I
Characteristics of the 21-patient
cohort.
| Characteristic | Value (%) |
|---|
| Gender |
| Male | 13 (61.9) |
| Female | 8 (38.1) |
| M/F ratio | 1.625:1 |
| Age, years |
| Range | 10–65 |
| Mean | 42.5 |
| Males | 42.4 |
| Females | 42.6 |
| Site |
| Buccal mucosa | 6 (28.5) |
| Parotid gland | 4 (19.0) |
| Palate | 4 (19.0) |
| Nasolabial
groove | 2 (9.5) |
| Lip | 1 (4.8) |
| Tongue | 1 (4.8) |
| Gingiva | 1 (4.8) |
| Mandible | 1 (4.8) |
| Neck | 1 (4.8) |
| Diameter, cm |
| ≤2 | 8 (38.1) |
| >2 | 13 (61.9) |
| Symptoms |
| Painless | 16 (76.2) |
| Tender | 2 (9.5) |
| Spontaneously
painfula | 3 (14.3) |
| Duration |
| Longest, years | 30+ |
| Shortest,
months | 1+ |
| Table IISummary of clinical information of the
patient cohort. |
Table II
Summary of clinical information of the
patient cohort.
| Case | Age, years | Gender | Tumor location | Size, cm | Duration | Symptoms | Examination | Imaging | Pre-operative
diagnosis | Treatment | Recurrence |
|---|
| 1 | 62 | F | Buccal mucosa | 1.5 | 15 years | Painless | None | CDU | Hemangioma | Excision | NR |
| 2 | 46 | M | Parotid gland | 3.2 | 1 year | Painless | None | ECT/CDU | Pleomorphic
adenoma | LSD | NR |
| 3 | 38 | F | Parotid gland | 2.5 | 8 months | Painless | None | ECT | Pleomorphic
adenoma | LAD | NR |
| 4 | 49 | M | Buccal mucosa | 2.0 | 1 year | Painless | None | CDU | Unknown mass | Excision | NR |
| 5 | 36 | F | Buccal mucosa | 2.0 | 1 year | Painless | None | ECT | Unknown mass | Excision | NR |
| 6 | 65 | F | Nasolabial
groove | 2.5 | 30 years | Painless | FNA-blood | CDU | Schwannoma | Excision | NR |
| 7 | 51 | M | Parotid gland | 3.5 | 3 months | Painless | None | ECT/CDU | Pleomorphic
adenoma | LAD | NR |
| 8 | 51 | F | Buccal mucosa | 1.0 | 6 years | Pain | None | None | Unknown mass | Excision | NR |
| 9 | 50 | M | Nasolabial
groove | 3.0 | 18 years | Painless | FNA-blood | ECT | Hemangioma | Excision | NR |
| 10 | 49 | F | Palate | 1.0 | 3 months | Painless | FNA-blood, cast-off
cells | None | Hemangioma | Excision | NR |
| 11 | 42 | M | Parotid gland | 2.4 | 1 year | Painless | None | CDU | Pleomorphic
adenoma | Excision | NR |
| 12 | 10 | F | Mandible | 3.5 | 1 month | Painless | Biopsy | DR | Unknown cyst | Excision | NR |
| 13 | 30 | F | Buccal mucosa | 3.0 | 1 month | Painless | FNA-blood | CDU | Unknown mass | Excision | NR |
| 14 | 20 | M | Gingiva | 2.5 | 1 month | Tenderness | Biopsy | None | Mass | Excision | NR |
| 15 | 60 | M | Palate | 1.5 | 1 year | Painless | None | None | Pleomorphic
adenoma | Excision | NR |
| 16 | 34 | M | palate | 1.0 | 5 years | Painless | None | None | Unknown mass | Excision | NR |
| 17 | 58 | M | Lip | 6.0 | 15 years | Pain | None | None | Neurofibroma | Excision | NK |
| 18 | 18 | M | Palate | 3.5 | 2 month | Painless | FNA-blood | None | Pleomorphic
adenoma | Excision | NR |
| 19 | 19 | M | Tongue | 3.5 | 2 years | Tenderness | None | None | Unknown mass | Excision | NR |
| 20 | 47 | M | Buccal mucosa | 2.0 | 2 month | Pain
Tenderness | Biopsy | None | Mass | Excision | NK |
| 21 | 57 | M | Neck | 4.0 | 4 years | Painless | FNA-blood | None | Schwannoma | Excision | NR |
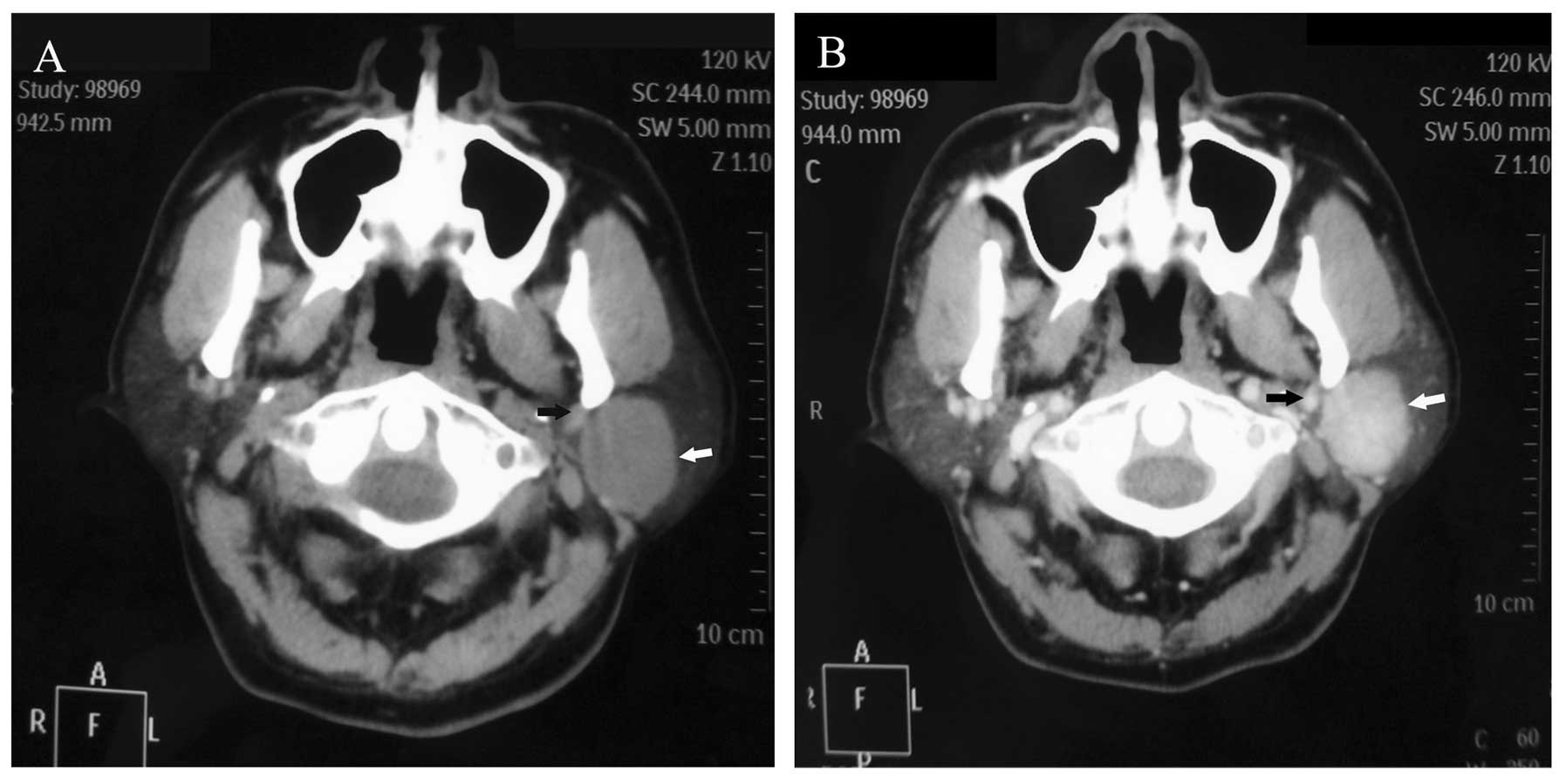
Investigations
Fine-needle aspiration (FNA) was undertaken in five
patients, and revealed blood and cast-off cells, indicating the
presence of hemangiomas. Enhanced computed tomography (ECT) of the
head and neck was performed in three cases and Doppler
ultrasonography in seven. An example of an ECT image is shown in
Fig. 1, showing an ovoid,
high-density area with a regular margin, but heterogeneous
enhancement displacing the left posterior facial vein in the
parotid gland. In this case, color Doppler examination also
revealed high resistance to blood flow in the intratumoral
arteries, indicating that the tumor was benign. In one case,
Doppler ultrasonography detected a feeding artery supplying an
angioleiomyoma in the parotid gland from the superficial temporal
artery. In four cases, color Doppler flow imaging did not detect
continuous or intermittent blood flow. Digital radiography of a
tumor in the mandible revealed a cystic lesion with clearly defined
borders in the left angle extending from the distal root of D6 to
the middle of the mandibular ramus, subsequently leading to tooth
mobility of D7 and D8. None of the cases were diagnosed correctly
by FNA or imaging studies.
Treatment and follow-up
All patients underwent excision of the tumor. Those
with tumors in the parotid gland also underwent parotidectomy.
Intraoperatively, the tumors were found to be well circumscribed.
One tumor had a partial capsule, however, the remainder had
complete capsules. Their cut surfaces were gray-white, brown or
dark red. The follow-up duration was 6–81 months, during which, no
local recurrences were observed (although two patients were lost to
follow up).
Pathological findings
Microscopically, the lesions consisted of a
proliferation of smooth muscle cells and numerous blood vessels of
varying size that were surrounded by smooth muscle bundles. The
spindle-shaped cells were characterized by elongated, cigar-like
nuclei and an eosinophilic cytoplasm. Smooth muscle bundles with
collagen fibers exhibited an interlacing and swirling arrangement.
The abundant blood vessels, with thin or thick walls and circular,
slit-like or stellate lumens, were of varying size between tumors
and in different areas of the same tumor. In certain cases,
neoplastic cells were arranged around vessels that were lined with
endothelial cells containing basophilic nuclei. Out of the 21
tumors, five were solid, six venous, nine cavernous and one
venous-cavernous (Table III). It
was noteworthy that six of the tumors (four solid and one each of
the venous and cavernous types) contained focal areas with hyaline
change. In eight tumors, including venous and cavernous lesions,
focal myxoid change was present. Areas containing small groups of
mature fat cells were observed in three tumors, one each of the
venous, cavernous and venous-cavernous types (Fig. 2). Two solid tumors demonstrated
calcified foci. Focal lymphocytic infiltration was identified in 11
tumors. Neither thrombi nor hemosiderin deposits were observed in
any of the tumors.
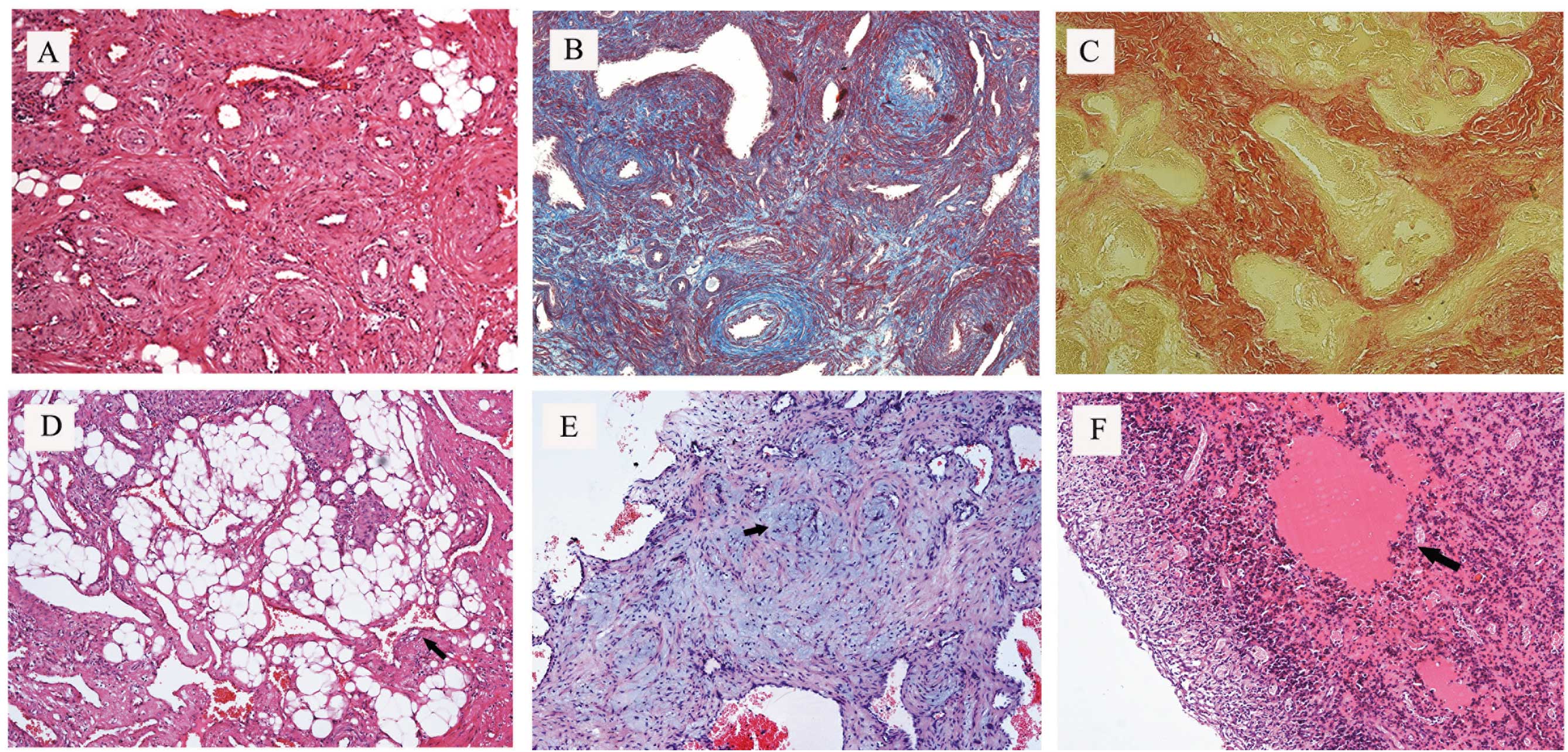 | Figure 2Angioleiomyoma tissue stained with
H&E, Masson’s trichrome and Van Gieson stains. (A) The
angioleiomyoma comprised of rich vascular channels with thick
vessel walls and smooth muscle bundles with elongated nuclei
(magnification, ×100). (B) Masson’s stain showing smooth muscle
fibers in red, erythrocytes in blue, collagen fibers in black and
nuclei in black-blue (magnification, ×100). (C) Van Gieson stain
showing smooth muscle fibers in red and collagen fibers in yellow
(magnification, ×100). (D) Groups of mature fat cells observed by
H&E staining (magnification, ×100). (E) Focal myxoid change
(black arrow) in the lesion, stained blue with H&E staining
(magnification, ×100). (F) Hyaline change (black arrow) observed by
H&E staining (magnification, ×100). H&E, hematoxylin and
eosin. |
| Table IIISummary of pathological
characteristics of the 21 tumors. |
Table III
Summary of pathological
characteristics of the 21 tumors.
| Microscopic |
|---|
|
|
|---|
| Histological
type | Hyaline change | Myxoid change | Mature fat
cell | Foci of
calcification | Focal lymphocytic
infiltration | Nerves |
|---|
| Solid, n | 4 | 0 | 0 | 2 | 4 | 1 |
| Venous, n | 1 | 2 | 1 | 0 | 6 | 1 |
| Cavernous, n | 1 | 5 | 1 | 0 | 1 | 1 |
| Venous-cavernous,
n | 0 | 0 | 1 | 0 | 0 | 0 |
| Total, n (%) | 6 (28.6) | 7 (38.1) | 3 (14.3) | 2 (9.5) | 11 (52.4) | 3 (14.3) |
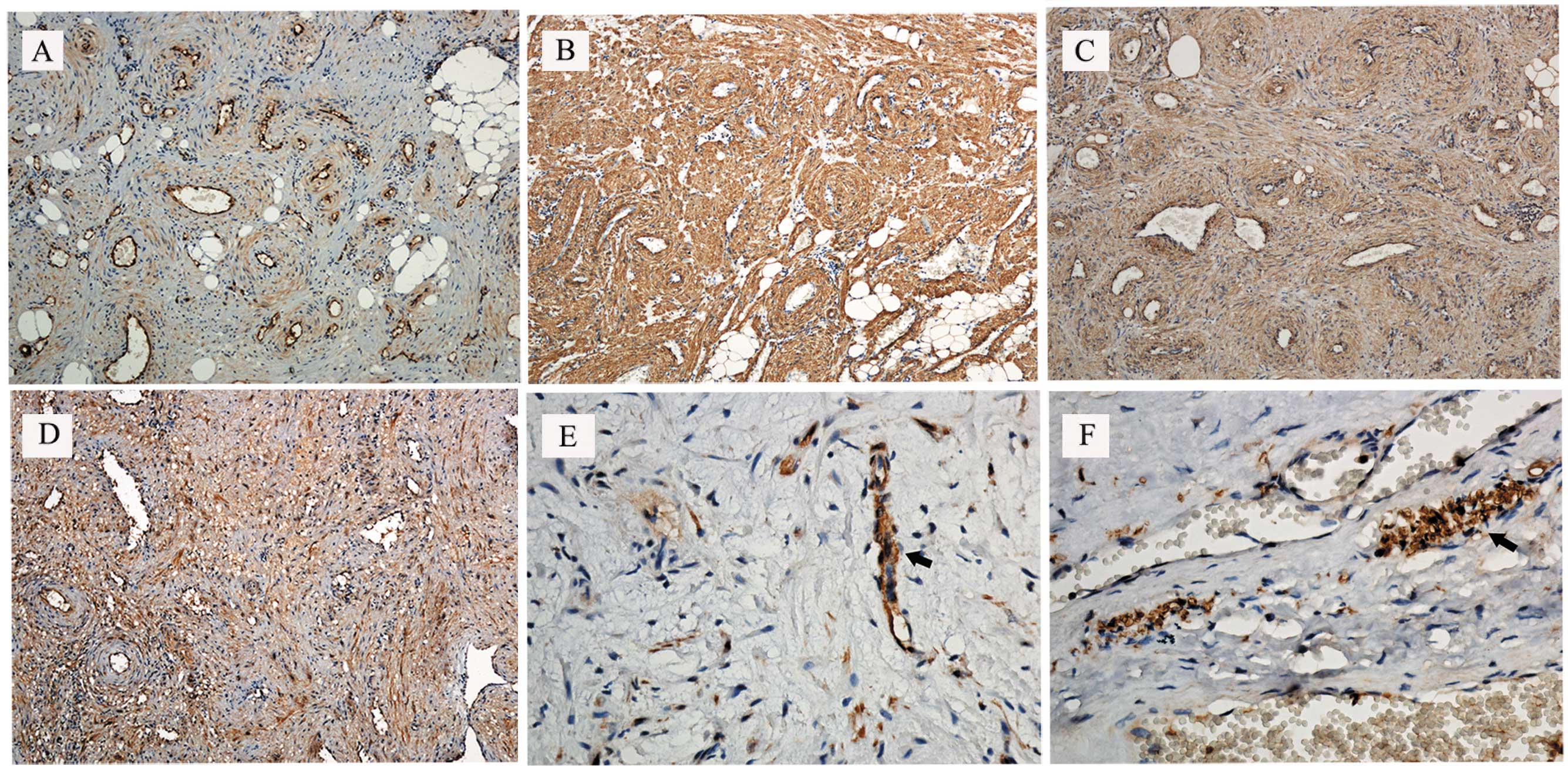
Immunohistochemical analysis revealed that the
spindle-shaped tumor cells were diffusely reactive to α-actin
smooth muscle and vimentin, and focally reactive to desmin.
Endothelial cells in tumor vessels stained positively for CD34. In
three cases, a few small neurons that stained positively for S-100
were evident close to the capsule (two cases) or interstitium (one
case; Fig. 3). The diagnosis of
angioleiomyoma was confirmed on the basis of these findings.
Discussion
Angioleiomyomas are extremely rare tumors,
particularly in the head and neck. The 21 patients included in the
present study who were treated over a period of 34 years account
for 10% of the cases in the published literature. The present
cohort was significantly younger than those investigated in other
studies, with a mean age of 42.5 years at diagnosis and a peak in
presentation in the fourth to sixth decades. Angioleiomyomas are
particularly rare in children (1,3,11–14)
and there is only one study of a congenital tumor (15). In the present study, the youngest
patient was 10 years old, with an angioleiomyoma located in the
mandible. Previous studies have reported that the lip, palate and
tongue are the most common sites for angioleiomyomas in the oral
cavity (3,14,16),
however, the present study identified a preponderance of tumors in
the buccal mucosa, followed by the parotid gland and palate. The
majority of angioleiomyomas are <2 cm in diameter on
presentation and rarely exceed 4–5 cm (1,3,8,13),
however, more than half the tumors in the present cohort measured
>2 cm in diameter at diagnosis. These differences may be
explained by referral patterns to the specialist West China
Hospital of Stomatology and the population it serves. In addition,
the four parotid angioleiomyomas are noteworthy, as these tumors
are particularly unusual in the major salivary glands. Currently,
<15 cases (including the four in the present study) have been
previously reported (5,13,17–21).
In addition to the three classical pathological
types, Morimoto further classified angioleiomyomas into two groups:
i) A larger group of extremity tumors that are frequently painful
and predominantly of the solid type; and ii) a smaller group of
painless tumors on the head that are predominantly (75%) of the
venous type (7). If pain is
provoked by angioleiomyomas, it is occasionally described as
paroxysmal, stinging or radiating, which are essentially the
symptoms of neuropathic pain (7,22,23).
One previous study indicated that only a small proportion (7.8%) of
oral angioleiomyomas are painful (22). In the present study, three patients
had radiating or stinging pain reminiscent of neuropathic pain,
three reported tenderness and one reported pain provoked by
exposure to the cold. Other studies have described pain that can be
provoked by cold and wind, pressure, pregnancy and menstruation,
however, it can also be spontaneous (1,3,9,24).
There are three possible theories explaining the cause of the pain:
i) The contraction of smooth muscle vessels, particularly those in
solid-type lesions, may cause local ischemia (7); ii) the compression of nerves
accompanying the blood vessels in the tumor (24), which relies on the existence of
neurofibrils within the tumor capsule (1,12,14,25,26);
and iii) secondary inflammation of the mass, with a mild to
moderate infiltration of inflammatory cells (22). At present, the first two theories
are considered to be the most plausible. Fox et al found
small neurofibrils, some closely associated with vessels, between
the smooth muscle bundles within the body of the tumor, but argued
that the capsular neurofibrils were more likely to be pain
generators than the small number of interstitial neurofibrils
(27). The present study revealed
positive immunoexpression of S-100 antigen by neurofibrils in three
tumors (of venous and cavernous type), indicating that the presence
of small interstitial neurofibrils and capsular nerves may explain
the occurrence and nature of the pain in certain patients (3). In the present study, extensive focal
lymphocytic infiltrations were also found in two tumors, although
in one of these cases the patient did not report pain. It was
hypothesized that compression of the nerves accompanying numerous
blood vessels in the tumor causes the pain, particularly in
venous-type and cavernous-type angioleiomyomas. In other words, the
pain may be closely associated with nerve and pathological type.
Although it was hypothesized that the presence of neural tissue in
an angioleiomyoma may be responsible for the symptoms of
neuropathic pain, the sample size used in the present study is too
small to draw any firm conclusions. Further studies are required,
although accumulating a sufficiently large cohort on which to
perform meaningful statistical analysis is a challenge in such a
rare tumor.
The pre-operative diagnosis of head and neck
angioleiomyomas is challenging (1).
FNA and cytology were not beneficial in the present study, indeed
it provided a misdiagnosis of hemangioma or schwannoma on several
occasions. Although imaging was also unhelpful in this regard, it
at least yielded information that guided the surgery, particularly
in those patients who also required parotidectomy. Magnetic
resonance imaging (MRI) can distinguish fibrous nodules (low signal
intensity on T1-and T2-weighted images) and lipomas (high signal
intensity on T1-weighted images) from angioleiomyomas (28), which show a uniform signal pattern,
with T1 signal intensity partially greater than the surrounding
soft tissue, but with marked hyperintensity on T2-weighted
sequences (29). Nevertheless, none
of the patients in the present study underwent MRI.
The differential diagnosis of angioleiomyoma
includes vascular tumors (such as hemangiomas and lymphangiomas),
certain benign mesenchymal tumors (including lipomas, schwannomas
and neurofibromas), pleomorphic adenomas and cysts (1,3,9).
Histological examination following resection remains the most
reliable method for diagnosis. In the present study, Masson’s
trichrome stain, Van Gieson stain and the positive expression of
desmin and α-actin smooth muscle antibodies demonstrated the
presence of smooth muscle cells, and the positive expression of
CD34 demonstrated the presence of vascular endothelium. It is
important to differentiate angioleiomyoma from other types of
spindle cell tumor, including leiomyoma (CD34− and
S-100−), myofibroma (desmin−,
CD34− and S-100−/+) and myopericytoma
(desmin−, CD34− and S100−)
(11). It is particularly important
to distinguish angioleiomyomas from malignant mesenchymal tumors,
including leiomyosarcoma (30).
Angioleiomyomas are predominantly composed of mature smooth muscle
cells, while leiomyosarcomas consist mainly of undifferentiated
mesenchymal cells or fibroblast-like cells and myofibroblast-like
cells (31). Immunohistochemical
and molecular markers, for example, proliferating cell nuclear
antigen, B-cell lymphoma 2, cyclin-dependent kinase 4, p53 and
mouse double minute 2 homolog also allow accurate discrimination
between benign and malignant smooth muscle tumors (32). A strength of the present study was
the access to archived tissue, which allowed tissue collected up to
34 years ago to be subjected to modern immunohistochemical
analysis, thus adding substantially to the body of literature on
these rare tumors.
In the present study, one patient had undergone
laser therapy at a local hospital prior to referral, however, the
tumor recurred one year later. In accordance with the literature,
the present study concluded that surgical resection along the tumor
capsule is the most effective treatment for all head and neck
angioleiomyomas (1,9,13), as
recurrence is rare following resection (13,33).
To the best of our knowledge, there have been no recurrences among
the patients enrolled in the present study, although two were lost
to follow-up. Other studies have reported four head and neck
angioleiomyomas that have recurred following resection: One in the
external skin of the nose at eight years; one in the larynx at an
unspecified time; and two recurring one and seven years after
resection, although the location was not reported (13,34,35).
In conclusion, it is extremely rare for an
angioleiomyoma to present in the head or neck; such cases comprised
only 0.18% of the cases at the West China Hospital of Stomatology,
a specialist institution, over 34 years. The diagnosis could only
be made pre-operatively if a biopsy was undertaken; pre-operative
cytological and imaging investigations were not fruitful in any of
the cases. At present, surgical excision is the only effective
treatment and recurrence is rare. In the present study, three
tumors that contained neurofibrils were identified. Angioleiomyoma
is a benign tumor and surgery is almost always curative, and
although it is rare in the head and neck, it is important to
recognize that it can only be reliably diagnosed prior to surgery
by biopsy.
Acknowledgements
This study was supported by the Science Foundation
for the Youth Scholars of Central South University (grant no.
120925) and the National Natural Science Foundation of China (grant
no. 81302621).
References
|
1
|
Hachisuga T, Hashimoto H and Enjoji M:
Angioleiomyoma. A clinicopathologic reappraisal of 562 cases.
Cancer. 54:126–130. 1984.
|
|
2
|
Enzinger FM and Weiss SW: Angioleiomyoma
(vascular leiomyoma). Soft Tissue Tumors. 3rd edition. Mosby; St.
Louis, MO: pp. 467–470. 1995
|
|
3
|
Brooks JK, Nikitakis NG, Goodman NJ and
Levy BA: Clinicopathologic characterization of oral
angioleiomyomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
94:221–227. 2002.
|
|
4
|
Wertheimer-Hatch L, Hatch GF 3rd, Hatch
BSK, et al: Tumors of the oral cavity and pharynx. World J Surg.
24:395–400. 2000.
|
|
5
|
Baden E, Doyle JL and Lederman DA:
Leiomyoma of the oral cavity: a light microscopic and
immunohistochemical study with review of the literature from 1884
to 1992. Eur J Cancer B Oral Oncol. 30B:1–7. 1994.
|
|
6
|
Cherrick HM, Dunlap CL and King OH Jr:
Leiomyomas of the oral cavity. Review of the literature and
clinicopathologic study of seven new cases. Oral Surg Oral Med Oral
Pathol. 35:54–66. 1973.
|
|
7
|
Morimoto N: Angiomyoma (vascular
leiomyoma): a clinicopathologic study. Med J Kagoshima Univ.
24:663–683. 1973.
|
|
8
|
MacDonald DM and Sanderson KV:
Angioleiomyoma of the skin. Br J Dermatol. 91:161–168. 1974.
|
|
9
|
Ramesh P, Annapureddy SR, Khan F and
Sutaria PD: Angioleiomyoma: a clinical, pathological and
radiological review. Int J Clin Pract. 58:587–591. 2004.
|
|
10
|
McGuff HS, Jones AC and Ellis E 3rd: Oral
and maxillofacial pathology case of the month. Angiomyoma (vascular
leiomyoma). Tex Dent J. 129:454–455. 2012.
|
|
11
|
Gaitan Cepeda LA, Quezada Rivera D,
Tenorio Rocha F, Leyva Huerta ER and Mendez Sánchez ER: Vascular
leiomyoma of the oral cavity. Clinical, histopathological and
immunohistochemical characteristics Presentation of five cases and
review of the literature. Med Oral Pathol Oral Cir Bucal.
13:E483–E488. 2008.
|
|
12
|
Duhig JT and Ayer JP: Vascular leiomyoma.
A study of sixty one cases. Arch Pathol. 68:424–430. 1959.
|
|
13
|
Wang CP, Chang YL and Sheen TS: Vascular
leiomyoma of the head and neck. Laryngoscope. 114:661–665.
2004.
|
|
14
|
Esguep A and Solar M: Oral vascular
leiomyoma - report of 5 cases and review of the literature. J Oral
Med. 41:126–129. 1986.
|
|
15
|
Kim YH, Jang YW, Pai H and Kim SG:
Congenital angiomyoma of the tongue: case report. Dentomaxillofac
Radiol. 39:446–448. 2010.
|
|
16
|
Epivatianos A, Trigonidis G and
Papanayotou P: Vascular leiomyoma of the oral cavity. J Oral
Maxillofac Surg. 43:377–382. 1985.
|
|
17
|
Wong SK, Ahuja A, Chow J and King WW:
Angioleiomyoma in the submandibular region: an unusual tumor in an
unusual site. Otolaryngol Head Neck Surg. 122:144–145. 2000.
|
|
18
|
Natiella JR, Neiders ME and Greene GW:
Oral leiomyoma. Report of six cases and a review of the literature.
J Oral Pathol. 11:353–365. 1982.
|
|
19
|
Kido T and Sekitani T: Vascular leiomyoma
of the parotid gland. ORL J Otorhinolaryngol Relat Spec.
51:187–191. 1989.
|
|
20
|
Ide F, Mishima K and Saito I: Angiomyoma
in the submandibular gland: a rare location for a ubiquitous
tumour. J Laryngol Otol. 117:1001–1002. 2003.
|
|
21
|
McDaniel RK: Benign mesenchymal neoplasms.
Surgical Pathology of the Salivary Glands. Ellis GL, Auclair P and
Gnepp DR: 2nd edition. WB Saunders; Philadelphia: pp. 489–513.
1991
|
|
22
|
Toida M, Koizumi H and Shimokawa K:
Painful angiomyoma of the oral cavity: report of a case and review
of the literature. J Oral Maxillofac Surg. 58:450–453. 2000.
|
|
23
|
Akizawa S: Angiomyoma: an analysis of 124
cases. Jikeikai Med J. 27:71–82. 1980.
|
|
24
|
Montgomery H and Winkelmann RK:
Smooth-muscle tumours of the skin. AMA Arch Derm. 79:32–40.
1959.
|
|
25
|
Stout AP: Solitary cutaneous and
subcutaneous leiomyoma. Am J Cancer. 29:435–469. 1937.
|
|
26
|
Magner D and Hill DP: Encapsulated
angiomyoma of the skin and subcutaneous tissues. Am J Clin Pathol.
35:137–141. 1961.
|
|
27
|
Fox SB, Heryet A and Khong TY:
Angioleiomyomas: an immunohistological study. Histopathology.
16:495–496. 1990.
|
|
28
|
Stoller DW, Steinkirchner TM and Porter
BA: Bone and soft tissue tumors. Magnetic Resonance Imaging in
Orthopaedics and Sports Medicine. Stoller DW: 2nd edition. JB
Lippincott; Philadelphia: pp. 1092–1093. 1993
|
|
29
|
Eley KA, Alroyayamina S, Golding SJ, Tiam
RN and Watt-Smith SR: Angioleiomyoma of the hard palate: report of
a case and review of the literature and magnetic resonance imaging
findings of this rare entity. Oral Surg Oral Med Oral Pathol Oral
Radiol. 114:e45–e49. 2012.
|
|
30
|
Bouquot JE and Nikai H: Lesions of the
oral cavity. Diagnostic Surgical Pathology of the Head and Neck.
Gnepp DR: 1st edition. WB Saunders; Philadelphia: pp. 141–233.
2001
|
|
31
|
Kawakami T, Hasegawa H and Chino T: A
transmission electron microscopic study of two cases of oral smooth
muscle neoplasm. J Oral Maxillofac Surg. 45:551–555. 1987.
|
|
32
|
Nikitakis NG, Lopes MA, Bailey JS,
Blanchaert RH Jr, Ord RA and Sauk JJ: Oral leiomyosarcoma: review
of the literature and report of two cases with assessment of the
prognostic and diagnostic significance of immunohistochemical and
molecular markers. Oral Oncol. 38:201–208. 2002.
|
|
33
|
Keerthi R, Nanjappa M, Deora SS and
Kumaraswamy SV: Angioleiomyoma of cheek: report of two cases. J
Maxillofac Oral Surg. 8:298–300. 2009.
|
|
34
|
Svane TJ, Smith BR, Cosentino BJ, Cundiff
EJ and Ceravolo JJ Jr: Oral leiomyomas. Review of the literature
and report of a case of palatal angioleiomyoma. J Periodontol.
57:433–435. 1986.
|
|
35
|
Hirshoren N, Weinberger JM, Neuman T, Ilan
O and Ben-Yaakov A: Recurrent vascular leiomyoma of the larynx:
clinical and histopathologic characteristics and treatment. Ear
Nose Throat J. 89:382–386. 2010.
|