Introduction
Carcinosarcoma is a rare neoplasm that shows an
admixture of epithelial and mesenchymal components (1,2). The
carcinomatous component of carcinosarcoma may be represented by
varying forms, including transitional cell carcinoma,
adenocarcinoma or squamous cell carcinoma (SCC). The sarcomatous
portion shows specific features of mesenchymal differentiation,
with elements that include chondrosarcoma, osteosarcoma,
rhabdomyosarcoma, liposarcoma and fibrosarcoma (3–6).
Carcinosarcoma is often localized in a wide variety of organs,
including the uterus, breast, esophagus, larynx, lungs, urinary
bladder, prostate and oviducts, with a variable frequency; however,
localization in the renal pelvis is rare (7). The present study reports a case of
carcinosarcoma of the renal pelvis in a 73-year-old female, which
consisted of SCC and fibrosarcoma components, and discusses the
diagnosis and treatment of such tumors. Patient provided written
informed consent.
Case report
Patient presentation
A 73-year-old female was admitted to the Department
of Urology, First Hospital of Jilin University (Jilin, China)
presenting with intermittent hematuria and right-flank pain for one
month. The patient had a history of hysterectomy for uterine
fibroids 10 years previously. The patient had no other voiding
complaints or any significant urological history. The patient also
denied past tobacco use or analgesic abuse, and the results of the
physical examination were normal, except for mild percussion pain
in the right kidney area. Urinalysis revealed increased numbers of
red blood cells, leukocytes and suspicious malignant cells.
Furthermore, protein was found to be excreted in the urine (score,
1+) and the analysis of the blood biochemistry revealed an elevated
erythrocyte sedimentation rate (90 ml/h).
Tumor imaging and resection
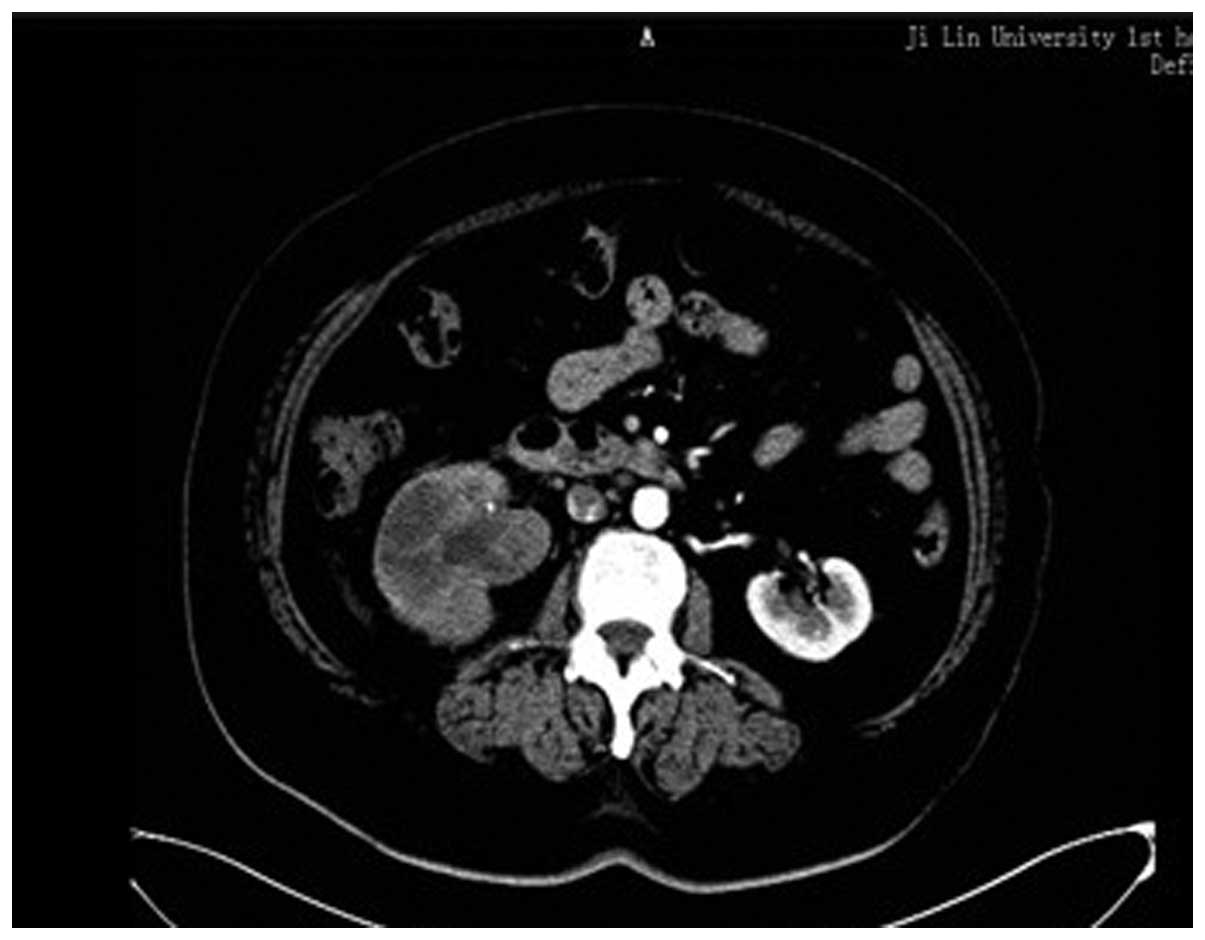
Abdominal ultrasonography showed a solid, relatively
well-demarcated tumor, 3.0×3.1 cm, occupying the right renal
pelvis. Computed tomography (CT) showed a 2.4×2.5-cm heterogeneous
and poorly-enhanced mass in the right renal pelvis (Fig. 1). The CT findings also revealed a
thickened ureter wall, with irregular contrast enhancement.
Cystoscopy showed no abnormalities in the urinary bladder.
Retrograde pyelography could not be performed due to ureteral
catheter obstruction. Further clinical analyses revealed no
metastasis to other organs. Based on the clinical and radiological
findings, a laparoscopic radical resection of the right kidney and
an open ureterectomy were performed to remove the tumors.
Macroscopic and histological tumor
analysis
Macroscopic examination of the 13×8×6-cm nephrectomy
specimen revealed a 8×5×4-cm tumoral mass in the renal pelvis. The
cut section of the mass was gray-white in color, with a hard
consistency. Areas of extensive necrosis were also present. The
tumor had invaded the full-thickness of the renal pelvic wall and
peripelvic adipose tissue. Furthermore, invasion into the renal
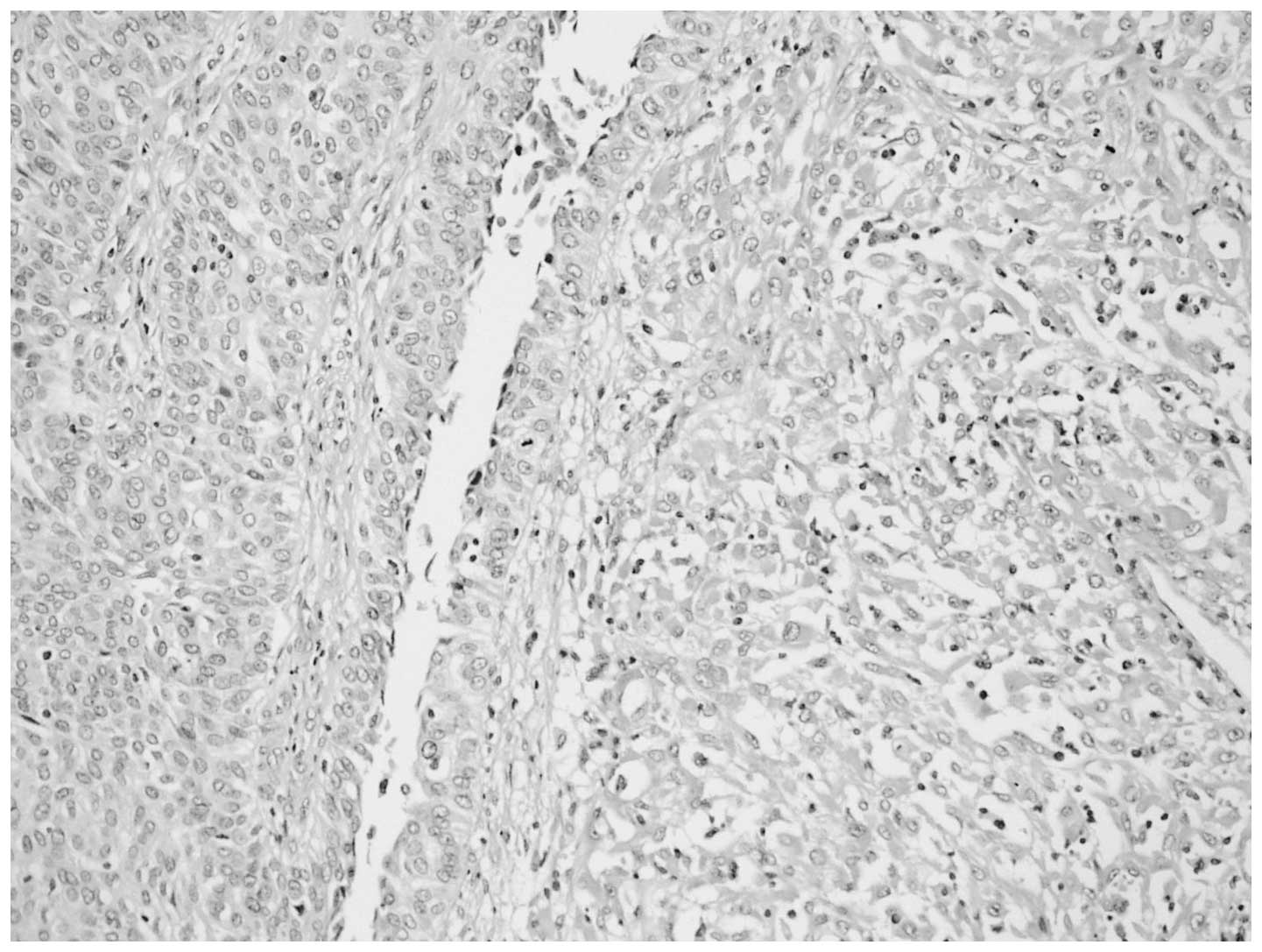
parenchyma was observed. Histological examination of the tumor
showed a malignant neoplasm comprising of epithelial and
mesenchymal components, which were largely separated from each
other (Fig. 2). However, in certain
areas, the epithelial component blended into the sarcomatous
component, generating a histological transition between the two.
The sarcomatous areas primarily consisted of spindle cells, which
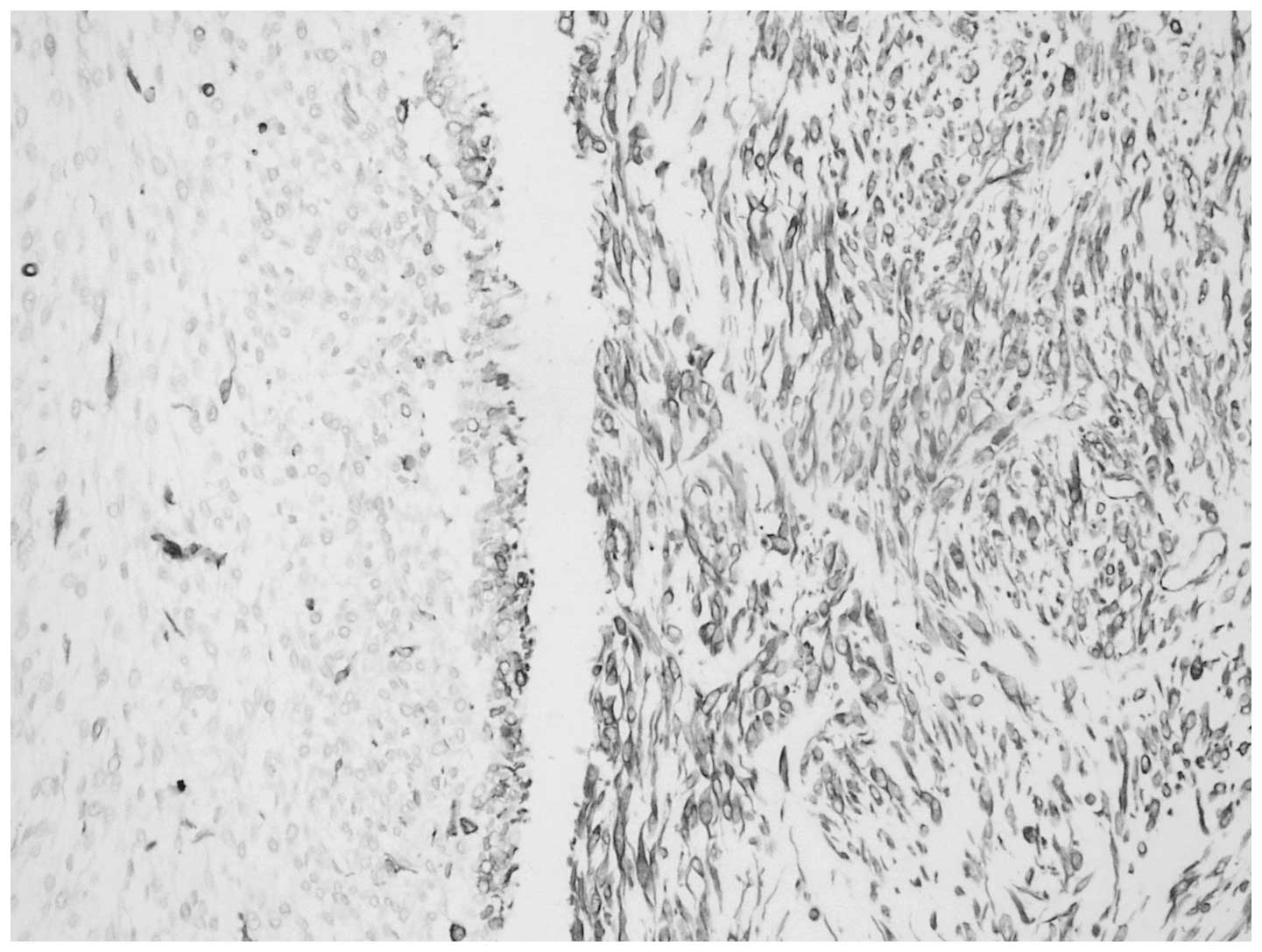
were full of eosinophilic cytoplasm. Immunohistochemical staining
was performed using a panel of markers, including cytokeratin,
vimentin, Ki-67 antigen and p53. The epithelial portion of the
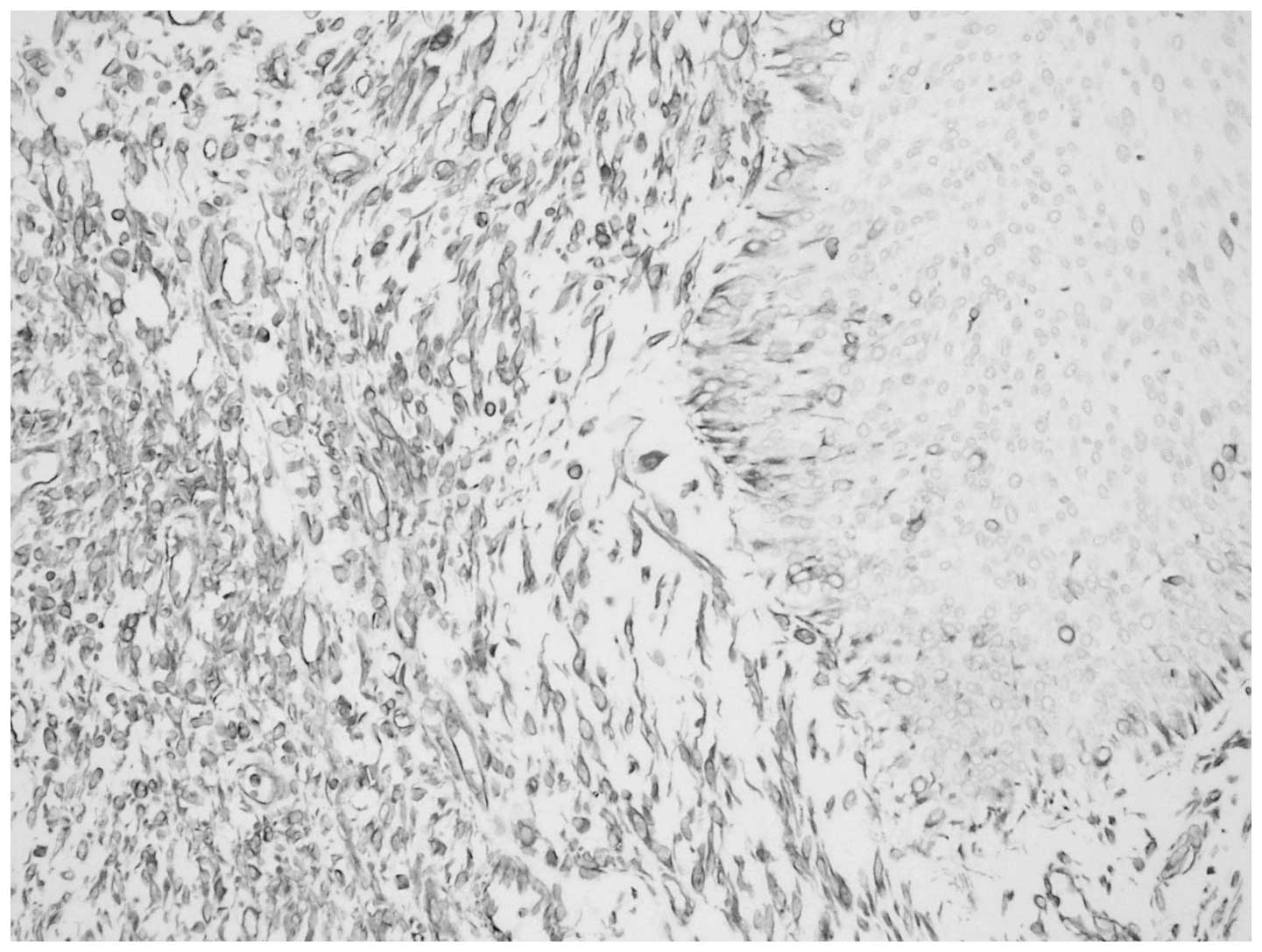
tumor was found to stain positively for cytokeratin (Fig. 3) and the sarcomatoid spindle cells
were observed to stain positively for vimentin, but negatively for
cytokeratin (Fig. 4). The tumor
cells in the epithelial and sarcomatous components were also found
to express p53 protein in the nuclei. The expression level of p53
was >10%. Furthermore, the Ki-67 labeling indices were >20%
in all of the tumor cells. Due to the advanced age of the patient,
chemotherapy and radiotherapy were not administered. The patient
was discharged six days after surgery and no recurrence was
observed after eight months.
Discussion
Carcinosarcoma is a rare, malignant neoplasm that
shows histological evidence of intimately mixed epithelial and
mesenchymal elements (3). The
histogenesis of carcinosarcomas remains controversial and there are
two predominant theories. Völker et al (8) proposed that carcinosarcomas may
originate from a common pluripotent progenitor cell that is capable
of undergoing epithelial and mesenchymal differentiation. Perret
et al (9) proposed that
certain carcinosarcomas should be regarded as a variant of
sarcomatoid carcinoma (metaplastic carcinoma) that shows prominent
heterologous differentiation.
Carcinosarcoma has been described in various organs,
including the uterus, breast, stomach, lung, salivary glands,
thyroid gland and gallbladder. However, carcinosarcoma of the
urogenital organs has rarely been reported (1–4,6,10–15).
Carcinosarcoma of the renal pelvis has been shown to
be aggressive and often has a poor prognosis (16–18),
thus it is important to detect and diagnose this disease early.
Microscopically, the carcinomatous component is primarily composed
of transitional cell carcinoma and the sarcomatous component is
predominantly composed of spindle and/or pleomorphic tumor giant
cells (11). In the present case,
light microscopy revealed epithelial and sarcomatous components,
which were largely separated from each other. However, in certain
areas, the epithelial component blended into the sarcomatous
component, generating a histological transition between the
two.
Due to the similar microscopic appearance of
carcinosarcomas and sarcomatoid carcinomas, immunohistochemistry
may be a useful diagnostic adjunct for differentiating between
these tumors. In the present case, antigenic determinants that were
specific for epithelial cells, such as cytokeratin, were
identified. Furthermore, the sarcomatous component was
characterized by strong staining for vimentin. In addition, the
lack of expression of keratin markers in the mesenchymal component
further confirmed the diagnosis of carcinosarcoma.
No clinical trials have been specifically designed
for carcinosarcoma, thus an optimal treatment strategy has yet to
be established. At present, radical resection is the only curative
treatment. Nephrectomy, radiation therapy and chemotherapy have
been used alone or in combination (1,19). In
the present case, due to the age of the patient and the history of
previous pelvic surgery, a laparoscopic radical resection of the
right kidney and ureter was performed. Previous studies have
reported very poor prognoses for carcinosarcoma, with a median
cancer-specific survival time of approximately one year (6,9,20). One
half of patients are reported to succumb within approximately one
year of diagnosis. Chen et al (12) reported the longest survival period
of two years. Cancer-specific survival times have been found to be
significantly improved for patients who undergo radical resection
rather than chemotherapy or radiation therapy.
In conclusion, carcinosarcoma of the renal pelvis is
a rare, aggressive tumor, with a low survival rate. Although rare,
carcinosarcoma should be included in the differential diagnosis.
Further investigations into the natural history and prognostic
factors of this disease and specific guidelines regarding
therapeutic approaches for this tumor are urgently required.
References
|
1
|
Chiu KC, Lin MC, Liang YC and Chen CY:
Renal carcinosarcoma: case report and review of literature. Ren
Fail. 30:1034–1039. 2008.
|
|
2
|
Fauci PA Jr, Therhag HG and Davis JE:
Carcinosarcoma of the renal pelvis. J Urol. 85:897–902. 1961.
|
|
3
|
Dimitriou RJ, Gattuso P and Coogan CL:
Carcinosarcoma of the renal pelvis. Urology. 56:5082000.
|
|
4
|
Yilmaz E, Birlik B, Arican Z, et al:
Carcinosarcoma of the renal pelvis and urinary bladder: a case
report. Korean J Radiol. 4:255–259. 2003.
|
|
5
|
Lema Grille J, Blanco Parra M, Suárez
Peñaranda JM and Durana Tonder C: Carcinosarcoma of the renal
pelvis: report of a case and review of the literature. Actas Urol
Esp. 26:509–512. 2002.(In Spanish).
|
|
6
|
Vermeulen P, Hoekx L, Colpaert C, et al:
Biphasic sarcomatoid carcinoma (carcinosarcoma) of the renal pelvis
with heterologous chondrogenic differentiation. Virchows Arch.
437:194–197. 2000.
|
|
7
|
Reuter VE: Sarcomatoid lesions of the
urogenital tract. Semin Diagn Pathol. 10:188–201. 1993.
|
|
8
|
Völker HU, Zettl A, Schön G, et al:
Molecular genetic findings in two cases of sarcomatoid carcinoma of
the ureter: evidence for evolution from a common pluripotent
progenitor cell? Virchows Arch. 452:457–463. 2008.
|
|
9
|
Perret L, Chaubert P, Hessler D and
Guillou L: Primary heterologous carcinosarcoma (metaplastic
carcinoma) of the urinary bladder: a clinicopathologic,
immunohistochemical, and ultrastructural analysis of eight cases
and a review of the literature. Cancer. 82:1535–1549. 1998.
|
|
10
|
Baschinsky DY, Chen JH, Vadmal MS, et al:
Carcinosarcoma of the urinary bladder - an aggressive tumor with
diverse histogenesis. A clinicopathologic study of 4 cases and
review of the literature. Arch Pathol Lab Med. 124:1172–1178.
2000.
|
|
11
|
Rao MS, Lotuaco LG and McGregor DH:
Carcinosarcoma of the adult kidney. Postgrad Med J. 53:408–411.
1977.
|
|
12
|
Chen KT, Workman RD, Flam MS and DeKlotz
RJ: Carcinosarcoma of renal pelvis. Urology. 22:429–431. 1983.
|
|
13
|
Ridolfi RL and Eggleston JC:
Carcinosarcoma of the renal pelvis. J Urol. 119:569–572. 1978.
|
|
14
|
Pusiol T, Morichetti D, Zorzi MG and
Piscioli F: Carcinosarcoma of the renal pelvis: inaccurate
documentation of origin and incomplete review of the literature.
Ren Fail. 33:844–845. 2011.
|
|
15
|
Wang J, Wang FW and Kessinger A: The
natural history and outcomes of the patients with carcinosarcoma
involving kidney and renal pelvis. Adv Urol. 2011:6939642011.
|
|
16
|
Tarry WF, Morabito RA and Belis JA:
Carcinosarcoma of the renal pelvis with extension into the renal
vein and inferior vena cava. J Urol. 128:582–585. 1982.
|
|
17
|
Tajima Y and Aizawa M: Unusual renal
pelvic tumor containing transitional cell carcinoma, adenocarcinoma
and sarcomatoid elements (so-called sarcomatoid carcinoma of the
renal pelvis). A case report and review of the literature. Acta
Pathol Jpn. 38:805–814. 1988.
|
|
18
|
Lopez-Beltran A, Escudero AL, Cavazzana
AO, et al: Sarcomatoid transitional cell carcinoma of the renal
pelvis. A report of five cases with clinical, pathological,
immunohistochemical and DNA ploidy analysis. Pathol Res Pract.
192:1218–1224. 1996.
|
|
19
|
Orsatti G, Corgan FJ and Goldberg SA:
Carcinosarcoma of urothelial organs: sequential involvement of
urinary bladder, ureter, and renal pelvis. Urology. 41:289–291.
1993.
|
|
20
|
Johnin K, Kadowaki T, Kushima M, et al:
Primary heterologous carcinosarcoma of the ureter with necrotic
malignant polyps. Report of a case and review of the literature.
Urol Int. 70:232–235. 2003.
|