Introduction
Cancer is a global disease with a high incidence of
mortality, having caused 7.6 million mortalites in 2008 alone. Over
the past 10 years, there has been a decreasing trend in mortality
due to cancer, allowing for the prevention of ~1.18 million
cancer-related mortalities (1,2).
Lung, colorectal and gastric cancer are the leading
cancer types in terms of occurrence and severity: lung cancer is
the most common cancer worldwide and the first leading cause of
cancer mortality, colorectal cancer is the third most common cancer
worldwide and the fourth leading cause of cancer-related mortality,
while gastric cancer is the fourth most common cancer worldwide and
the third leading cause of cancer-related mortality (1). The incidence of cancer has seen a
steady decline in males while it has remained stable in females,
resulting in a gradual decrease in the overall mortality rate with
regard to cancer (2). Thus NCCN
guidelines suggest that the K-ras mutation be detected prior
to applying medication such as cetuximab.
Materials and methods
Patients
Clinical samples were obtained from 100 hospitals in
China, including 131 tissue samples, 51 plasma samples, and 5
pleural and ascites samples for lung cancer; 445 tissue and 60
plasma samples for colorectal cancer; and 126 tissue and 9 plasma
samples for gastric cancer. Approval for this study was obtained
from the Shanghai Clinical Research Center Ethics Committee. All
patients participating in this study provided written informed
consent.
Tissue samples were stored and transported under
controlled temperatures, while plasma, and pleural and ascites
samples were transported on ice packs. The following materials were
purchased: Taq DNA polymerase (Takara Biotechnology Co., Ltd.,
Dalian, China), dNTP (Shi Ze Biotechnology Co., Ltd., Shanghai,
China), the DNA extraction kit (DN10, Aidlab Biotechnologies Co.,
Ltd., Beijing, China), PCR instrument (EDC-810, Eastwin
Biotechnology Co., Ltd., Beijing, China), BioSafe Centrifuge
Systems (L420, Xiangyi LXJ Centrifuge Instruments Co., Ltd.).
Methods
Nested and COLD-PCR were used to detect the
K-ras mutations. Regular PCR was used to amplify the 465-bp
outer product. The primers used were: forward, 5′-GTCGATGGAGG
AGTTTGTAAATGAAGT-3′ and reverse
5′-TTCAGATAACTTAACTTTCAGCATAATTATCTTG-3′. This was followed by 10
μl PCR reaction mixture including 0.25 mM dNTP, 0.5 μM primers, 0.5
units Taq DNA polymerase and 10 ng DNA template. The PCR program
was conducted under the following conditions: 3 min at 95°C for 1
cycle, 32 amplification cycles for 30 sec at 94°C, 30 sec in 57°C,
and 30 sec at 72°C, and maintained for 5 min at 72°C. COLD-PCR was
used to amplify the 155-bp inner product. The primers used were:
forward, 5′-GTCACATTTT CATTATTTTTATTATAAGG-3′ and reverse
5′-TTTACCTCTATTGTTGGATCATATTC-3′. This was followed by 50 μl PCR
reaction mixture including 0.25 mM dNTP, 0.5 μM primers, 0.5 units
Taq DNA polymerase and 1 μl outer PCR product. The PCR program was
conducted under the following conditions: 3 min at 95°C for 1
cycle, 40 amplification cycles for 30 sec at 80°C, 30 sec in 58°C,
30 sec at 72°C, followed by 15 cycles for 30 sec at 94°C, 30 sec at
58°C, and 30 sec at 72°C, maintained for 5 min at 72°C.
The Chi-squared test was used for statistical
analysis. P<0.05 was considered statistically significant.
Results
The K-ras mutation frequency was detected in
lung cancer (Table I), colorectal
cancer (Table II) and gastric
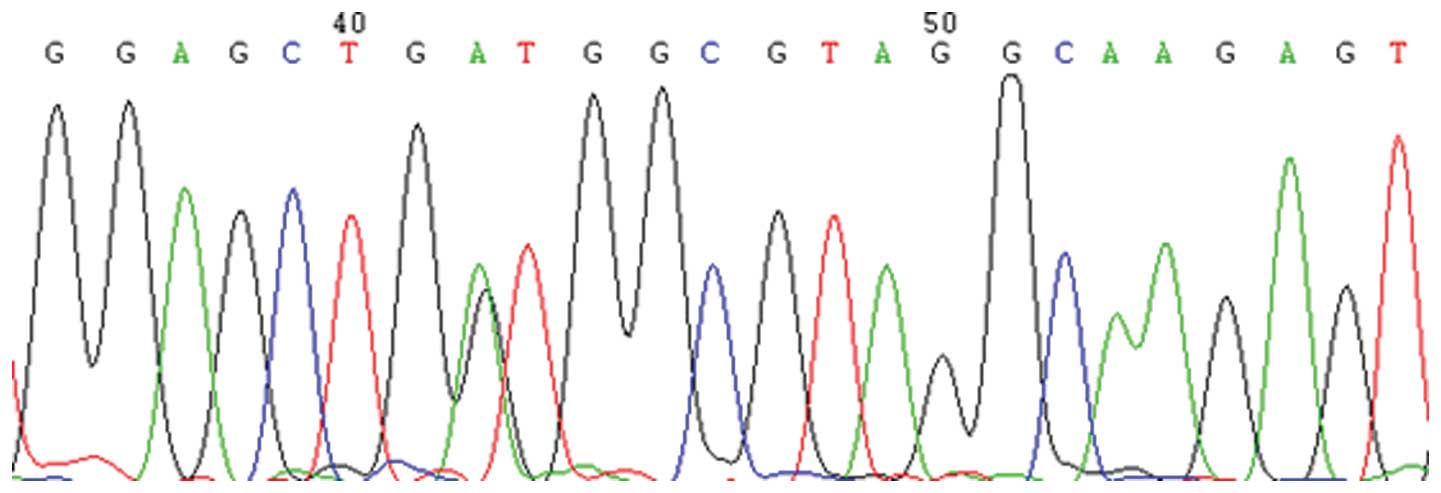
cancer (Table III). COLD-PCR was
used to detect the K-ras mutations. Fig. 1 shows the representative results,
which showed the G12D (GGT>GAT) mutation.
 | Table IThe mutation frequencies of
K-ras gene in different sample types, genders and age groups
of lung cancer patients detected with COLD-PCR and sequencing. |
Table I
The mutation frequencies of
K-ras gene in different sample types, genders and age groups
of lung cancer patients detected with COLD-PCR and sequencing.
| | Mutation frequency
(%) |
|---|
| |
|
|---|
| | Type of samples | Gender | Age (years) |
|---|
| |
|
|
|
|---|
| Amino acid
change | K-ras
mutation | Plasma
N=51 | Tumor
tissue
N=131 | Pleural and
ascites
N=5 | Male
N=123 | Female
N=64 | Youth
(25–44)
N=9 | Middle age
(45–59)
N=72 | Elderly
(60–90)
N=106 |
|---|
| G12S | GGT>AGT | | | | | | | | |
| G12R | GGT>CGT | | | | | | | | |
| G12C | GGT>TGT | | 2 (1.53) | | 2 (1.63) | | | 1 (1.39) | 1 (0.94) |
| G12D | GGT>GAT | | 5 (3.82) | 1 (20) | 4 (3.25) | 2 (3.13) | | 1 (1.39) | 5 (4.72) |
| G12A | GGT>GCT | | | | | | | | |
| G12V | GGT>GTT | | 4 (3.05) | | 2 (1.63) | 2 (3.13) | | 1 (1.39) | 3 (2.83) |
| G13S | GGC>AGC | | | | | | | | |
| G13R | GGC>CGC | | | | | | | | |
| G13C | GGC>TGC | | | | | | | | |
| G13D | GGC>GAC | 1 (1.96) | 4 (3.05) | | 3 (2.44) | 2 (3.13) | 1 (11.11) | 2 (2.78) | 2 (1.89) |
| G13A | GGC>GCC | | | | | | | | |
| G13V | GGC>GTC | | | | | | | | |
| Q61K | CAA>AAA | | | | | | | | |
| Q61L | CAA>CTA | | | | | | | | |
| Q61H | CAA>CAT | | | | | | | | |
| Total (%) | | 1.96 | 11.45 | 20 | 8.94 | 9.38 | 11.11 | 6.94 | 10.38 |
| Table IIThe mutation frequencies of
K-ras gene in different sample types, genders, and age
groups of colorectal cancer patients detected with COLD-PCR and
sequencing. |
Table II
The mutation frequencies of
K-ras gene in different sample types, genders, and age
groups of colorectal cancer patients detected with COLD-PCR and
sequencing.
| | Mutation
frequency |
|---|
| |
|
|---|
| | Type of samples | Gender | Age (years) |
|---|
| |
|
|
|
|---|
| Amino acid
change | K-ras
mutation | Plasma
N=60 | Tumor
tissue
N=445 | Pleural and
ascites
N=0 | Male
N=294 | Female
N=211 | Youth
(25–44)
N=60 | Middle age
(45–59)
N=195 | Elderly
(60–90)
N=250 |
|---|
| G12S | GGT>AGT | | 2 (0.45) | | | 2 (0.95) | | 1 (0.51) | 1 (0.4) |
| G12R | GGT>CGT | | 1 (0.22) | | 1 (0.34) | | | | 1 (0.4) |
| G12C | GGT>TGT | | 5 (1.12) | | 3 (1.02) | 2 (0.95) | | 1 (0.51) | 4 (1.6) |
| G12D | GGT>GAT | 1 (1.67) | 35 (7.87) | | 14 (4.76) | 22 (10.43) | 3 (5) | 12 (6.15) | 21 (8.4) |
| G12A | GGT>GCT | | 4 (0.90) | | 3 (1.02) | 1 (0.47) | | 2 (1.03) | 2 (0.8) |
| G12V | GGT>GTT | 1 (1.67) | 14 (3.15) | | 9 (3.06) | 6 (2.84) | | 8 (4.10) | 7 (2.8) |
| G13S | GGC>AGC | 2 (0.45) | | | | 2 (0.95) | | | 2 (0.8) |
| G13R | GGC>CGC | | 1 (0.22) | | 1 (0.34) | | | 1 (0.51) | |
| G13C | GGC>TGC | | 1 (0.22) | | 1 (0.34) | | | | 1 (0.4) |
| G13D | GGC>GAC | 1 (1.67) | 24 (5.39) | | 11 (3.74) | 14 (6.64) | 2 (3.33) | 15 (7.69) | 8 (3.2) |
| G13A | GGC>GCC | | | | | | | | |
| G13V | GGC>GTC | | | | | | | | |
| Q61K | CAA>AAA | | | | | | | | |
| Q61L | CAA>CTA | | 2 (0.45) | | 1 (0.34) | 1 (0.47) | | 1 (0.51) | 1 (0.4) |
| Q61H | CAA>CAT | | | | | | | | |
| Total (%) | | 5 | 20.45 | | 14.97 | 23.70 | 8.33 | 21.03 | 19.2 |
| Table IIIThe mutation frequencies of
K-ras gene in different sample types, genders, and age
groups of gastric cancer patients detected with COLD-PCR and
sequencing. |
Table III
The mutation frequencies of
K-ras gene in different sample types, genders, and age
groups of gastric cancer patients detected with COLD-PCR and
sequencing.
| | Mutation
frequency |
|---|
| |
|
|---|
| | Type of
samples | Gender | Age (years) |
|---|
| |
|
|
|
|---|
| Amino acid
change | K-ras
mutation | Plasma
N=9 | Tumor
tissue
N=126 | Pleural and
ascites
N=0 | Male
N=92 | Female
N=43 | Youth
(25–44)
N=22 | Middle age
(45–59)
N=61 | Elderly
(60–90)
N=52 |
|---|
| G12S | GGT>AGT | | | | | | | | |
| G12R | GGT>CGT | | | | | | | | |
| G12C | GGT>TGT | | | | | | | | |
| G12D | GGT>GAT | | 3 (2.38) | | 3 (3.26) | | 1 (4.55) | 1 (1.64) | 1 (1.92) |
| G12A | GGT>GCT | | | | | | | | |
| G12V | GGT>GTT | | | | | | | | |
| G13S | GGC>AGC | | | | | | | | |
| G13R | GGC>CGC | | | | | | | | |
| G13C | GGC>TGC | | | | | | | | |
| G13D | GGC>GAC | | 6 (4.76) | | 4 (4.35) | 2(4.65) | 1 (4.55) | 2 (3.28) | 3 (5.77) |
| G13A | GGC>GCC | | | | | | | | |
| G13V | GGC>GTC | | | | | | | | |
| Q61K | CAA>AAA | | | | | | | | |
| Q61L | CAA>CTA | | | | | | | | |
| Q61H | CAA>CAT | | | | | | | | |
| Total (%) | | 0 | 7.14 | | 7.61 | 4.65 | 9.09 | 4.92 | 7.69 |
The total K-ras mutation frequency was 9.09,
18.61 and 6.67% in lung, colorectal and gastric cancer,
respectively, as detected in all types of samples which suggested
that the K-ras mutations occurred more frequently in
colorectal cancer than in the other two types of cancer
investigated.
Of 187 lung cancer patients investigated, four
mutation types were detected, including G12C (GGT>TGT), G12D
(GGT>GAT), G12V (GGT>GTT) and G13D (GGC>GAC). The mutation
frequency was 1.96, 11.45 and 20% in plasma, tumor tissue, and
pleural and ascites samples, respectively, with no statistical
significance being identified (P=0.0935). The ratio of male to
female patients was 8.94 and 9.38%, respectively, which did not
indicate statistical significance (P=0.9223). Similarly, the ratio
for youth, middle age, and elderly patients was 11.11, 6.94 and
10.38%, respectively, which did not indicate statistical
significance (P=0.7196).
Of 505 colorectal cancer patients investigated, 11
mutation types were detected, including G12S (GGT>AGT), G12R
(GGT>CGT), G12C (GGT>TGT), G12D (GGT>GAT), G12A
(GGT>GCT), G12V (GGT>GTT), G13S (GGC>AGC), G13R
(GGC>CGC), G13C (GGC>TGC), G13D (GGC>GAC) and Q61L
(CAA>CTA). The mutation frequency for plasma, and tumor tissue
samples was 5 and 20.45%, respectively, indicating statistical
significance (P=0.0039). The ratio for male to female patients was
14.97 and 23.70%, respectively, indicating statistical significance
(P=0.0129). Similarly, the ratio for youth, middle age, and elderly
patients was 8.33, 21.03 and 19.2%, respectively, which did not
indicate statistical significance (P=0.0824).
Of 135 gastric cancer patients investigated, the
mutation types G12D (GGT>GAT), and G13D (GGC>GAC) were
detected. The mutation frequency for plasma, and tumor tissue
samples was 0 and 7.14%, respectively, which did not indicate
statistical significance (P=1.0000). The ratio for male to female
patients was 7.61 and 4.65%, respectively, which indicated no
statistical significance (P=0.7860). Similarly, the ratio for
youth, middle age, to elderly patients was 9.09, 4.92 and 7.69%,
respectively, which indicated no statistical significance
(P=0.7425).
Of all the K-ras mutation types in lung
cancer, G12C accounted for 1.07%, G12D for 3.21%, G12V for 2.14%,
G13D for 2.67% of the total mutation frequency. Analysis of
colorectal cancer mutations showed that, G12D accounted for 7.13%,
G12V for 2.97%, G13D for 4.95%, while the remaining mutation types
collectively accounted for 3.56% of the total mutation frequency
(Table II). In gastric cancer
patients, only two K-ras mutation types were identified,
with G12D accounting for 2.22%, whereas G13D accounted for 4.44% of
the total mutation frequency. Thus, G12D and G13D are the two most
frequently occurring mutation types in the three types of cancer
investigated.
Discussion
The mammalian ras gene family comprises
H-ras, K-ras, N-ras, encoding H-ras, K-ras,
N-ras proteins, respectively, with a similar structure and
function. The Ras protein is located in the inner region of the
cell membrane, tranforms signals from EGFR to mitogen-activated
protein kinases (MAPKs), to control cell growth, proliferation, and
motility, as well as metastasis and angiogenesis (3). The K-ras gene usually contains
point mutations at codons 12, 13 and 61 (Tables I–III), and these mutations often activate
the K-ras oncogene (4,5). The
K-ras mutation status is associated with the therapeutic
efficacy of EGFR-targeting monoclonal antibodies, rendering
patients with K-ras mutation as not suitable for Erbitux
treatment (6).
Various methods have been developed to improve
detection sensitivity, such as denaturing high-performance liquid
chromatography (DHPLC) (7), nested
Allele-Specific Blocker (ASB-)PCR (8), PCR single-strand conformation
polymorphism (SSCP) (9),
restriction fragment length polymorphism (RFLP) (10), and the amplification refractory
mutation system (ARMS) (11). Due
to the need for simple equipment, high sensitivity, COLD-PCR
(co-amplification at lower denaturation temperature-PCR) (12–15)
has been widely used, it can enrich variant DNA sequences and
improve detection sensitivity.
In the present study, the results showed that the
mutation frequency of K-ras was different in the three types
of cancer, indicating statistical significance (P=0.0001). The
ratio for the variables compared was highest in colorectal cancer.
Thus, detection of K-ras mutation status is more important
for colorectal cancer patients when personalized medicine is
involved.
The mutation frequency was not statistically
significant for the different sample types for lung and gastric
cancer. Therefore, plasma samples may be substituted by tissue
samples when the latter are not readily available, particularly for
lung cancer patients, from whom pleural and ascites samples are
also feasible. However, other types of samples cannot be
substituted for colorectal cancer tissues for K-ras mutation
detection, considering that the detection frequency of K-ras
mutations in tumor tissues is 4-fold that of plasma samples, with
the difference between sample types being statistically significant
for colorectal cancer patients.
For lung cancer and gastric cancer patients, the
mutation frequency indicated no statistical significance for
gender, although a difference was identified for colorectal cancer.
The frequency for male to female was 14.97 and 23.70% (P=0.0129),
respectively, suggesting the likelihood of mutation in female
colorectal cancer patients as compared with their male
counterparts.
Age did not affect the mutation frequency in the
three types of cancer investigated, suggesting that K-ras
mutation does not play a role in patient age Previously, an
anticorrelation pattern of K-ras mutation status with the
therapeutic effect, progression-free survival and overall survival
following patient treatment with Erbitux was demonstrated (4,6). By
contrast, results of other studies have shown that many patients
cannot improve efficacy end-points after receiving Erbitux
(16,17) without K-ras mutation
detection. That finidng suggests that other key signal transduction
molecules also play an important role in the downstream of Erbitux
against EGFR, for example, B-raf, PIK3CA (17). Therefore, the mutation status of
genes such as B-raf, and PIK3CA should be detected at
the same time as the K-ras mutation status.
Acknowledgements
This study was supported by Science and Technology
Development Foundation in Baoshan District, Shanghai, China
(11-B-9), and Development Center Foundation for Medical Science and
Technology, Ministry of Health, China (W2012FZ139).
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011.
|
|
2
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013.
|
|
3
|
Kiaris H and Spandidos DA: Mutations of
ras genes in human tumours. International Journal of Oncology.
7:413–429. 1995.
|
|
4
|
Schubbert S, Shannon K and Bollag G:
Hyperactive Ras in developmental disorders and cancer. Nat Rev
Cancer. 7:295–308. 2007.
|
|
5
|
Bos JL, Fearon ER, Hamilton SR, et al:
Prevalence of ras gene mutations in human colorectal cancers.
Nature. 327:293–297. 1987.
|
|
6
|
Benvenuti S, Sartore-Bianchi A, Di
Nicolantonio F, et al: Oncogenic activation of the RAS/RAF
signaling pathway impairs the response of metastatic colorectal
cancers to anti-epidermal growth factor receptor antibody
therapies. Cancer Res. 67:2643–2648. 2007.
|
|
7
|
Lilleberg SL, Durocher J, Sanders C,
Walters K and Culver K: High sensitivity scanning of colorectal
tumors and matched plasma DNA for mutations in APC, TP53, K-RAS,
and BRAF genes with a novel DHPLC fluorescence detection platform.
Ann NY Acad Sci. 1022:250–256. 2004.
|
|
8
|
Mostert B, Jiang Y, Sieuwerts AM, et al:
KRAS and BRAF mutation status in circulating colorectal tumor cells
and their correlation with primary and metastatic tumor tissue. Int
J Cancer. 133:130–141. 2013.
|
|
9
|
Abdul Murad NA, Othman Z, Khalid M, et al:
Missense mutations in MLH1, MSH2, KRAS, and APC genes in colorectal
cancer patients in Malaysia. Dig Dis Sci. 57:2863–2872. 2012.
|
|
10
|
Sinha R, Hussain S, Mehrotra R, et al:
Kras gene mutation and RASSF1A, FHIT and MGMT gene promoter
hypermethylation: indicators of tumor staging and metastasis in
adenocarcinomatous sporadic colorectal cancer in Indian population.
PLoS One. 8:e601422013.
|
|
11
|
Bando H, Yoshino T, Tsuchihara K, et al:
KRAS mutations detected by the amplification refractory mutation
system-Scorpion assays strongly correlate with therapeutic effect
of cetuximab. Br J Cancer. 105:403–406. 2011.
|
|
12
|
Li J and Makrigiorgos GM: COLD-PCR: a new
platform for highly improved mutation detection in cancer and
genetic testing. Biochem Soc Trans. 37:427–432. 2009.
|
|
13
|
Zuo Z, Chen SS, Chandra PK, et al:
Application of COLD-PCR for improved detection of KRAS mutations in
clinical samples. Mod Pathol. 22:1023–1031. 2009.
|
|
14
|
Carotenuto P, Roma C, Cozzolino S, et al:
Detection of KRAS mutations in colorectal cancer with Fast
COLD-PCR. Int J Oncol. 40:378–384. 2012.
|
|
15
|
Pennycuick A, Simpson T, Crawley D, et al:
Routine EGFR and KRAS mutation analysis using COLD-PCR in non-small
cell lung cancer. Int J Clin Pract. 66:748–752. 2012.
|
|
16
|
Allegra CJ, Jessup JM, Somerfield MR, et
al: American Society of Clinical Oncology provisional clinical
opinion: testing for KRAS gene mutations in patients with
metastatic colorectal carcinoma to predict response to
anti-epidermal growth factor receptor monoclonal antibody therapy.
J Clin Oncol. 27:2091–2096. 2009.
|
|
17
|
De Roock W, Claes B, Bernasconi D, et al:
Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy
of cetuximab plus chemotherapy in chemotherapy-refractory
metastatic colorectal cancer: a retrospective consortium analysis.
Lancet Oncol. 11:753–762. 2010.
|