Introduction
Inflammatory myofibroblastic tumors (IMTs) are
uncommon, mesenchymal neoplasms that are composed of proliferative
myofibroblasts and infiltrating inflammatory cells, usually plasma
cells and lymphocytes (1). The
tumors have been documented to occur in various anatomical sites,
including the lungs, abdomen, retroperitoneum, pelvis, trunk,
peripheral nerves, soft tissue and breast (2,3). The
etiology of IMT remains uncertain and controversial. IMT is
generally accepted as a benign disease, however, in certain cases,
a malignant phenotype is observed. For example, Carillo et
al (4) reported a case of a
bilateral pulmonary IMT with left adrenal gland metastasis.
Complete surgical excision, when feasible, remains the primary
treatment of choice for IMT (5).
For inoperable cases, however, a treatment regimen with
chemotherapy or radiotherapy is adopted (6). The current study presents an unusual
case of IMT of the breast, with malignant transformation to a
metaplastic carcinoma following surgical resection. Consent was
obtained from the patient’s relatives.
Case report
A 56-year-old female was admitted to a local
hospital for the treatment of a rapidly growing mass in the right
breast. The patient claimed that the mass had been present for
>20 years, but had profoundly increased in size during the two
months prior to admission. A computed tomography (CT) scan
confirmed a solitary mass, ~9×6 cm in size, with a clear margin.
Subsequently, the patient underwent lumpectomy of the mass. Based
on the post-operative histopathological examination, the mass was
diagnosed as IMT, with positive staining for smooth muscle actin
(SMA) and Ki-67 (intense nuclear staining in 30% of the cells), and
negative staining for S-100, cluster of differentiation (CD)34, p63
and cytokeratin.
The patient suffered a relapse two months after the
lumpectomy and was transferred to the Department of Breast Surgery,
the First Affiliated Hospital of China Medical University
(Shenyang, Liaoning, China). Enhanced CT and ultrasonography
examinations revealed no abnormalities in the lungs, liver,
gallbladder or spleen. However, the patient exhibited a low serum
hemoglobin level of 57 g/l (normal range, 110–150 g/l). The
recurrent tumor mass was growing progressively and ulceration was
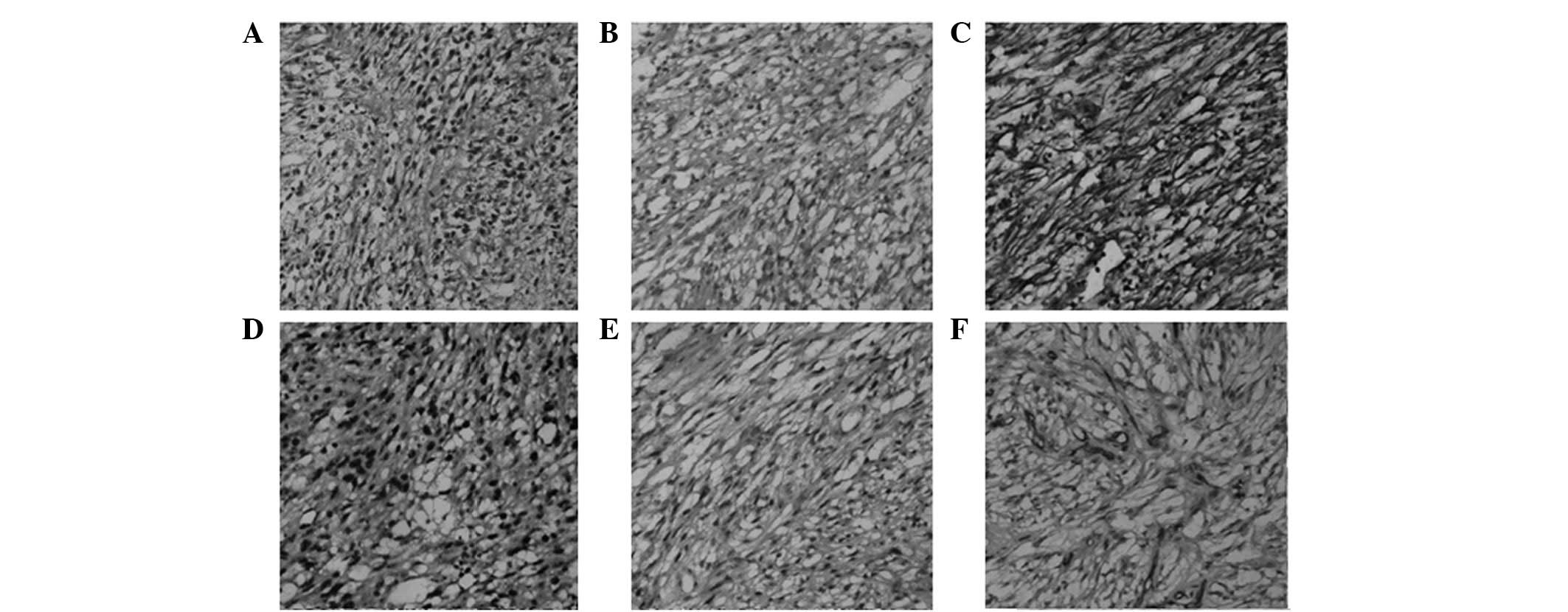
evident on the surface. Histologically, the tumor was predominantly
composed of a conspicuous proliferation of spindle cells arranged
in a loose fashion and surrounded by infiltrating inflammatory
cells. In addition, partial necrosis was noted (<10%).
Immunohistological studies revealed that the tumor yielded positive
staining for p63, vimentin, CD34 and CD68, but was negative for
SMA, CD38 and cytokeratin (Fig. 1).
Positive Ki-67 staining was observed in >40% of the cells
(Fig. 1), and five satellite
lesions were identified, with a mean diameter ranging between 1 and
2 cm. These clinical and pathological findings confirmed the
diagnosis of IMT with malignant transformation.
With regard to treating the symptomatic anemia, 10
units of leukocyte-filtered red blood cells were administered prior
to surgery. The patient then underwent a total mastectomy of the
right breast. During the surgery, the tumor (16×15×15 cm in size)
was found to intrude into the junctions of the ribs (third and
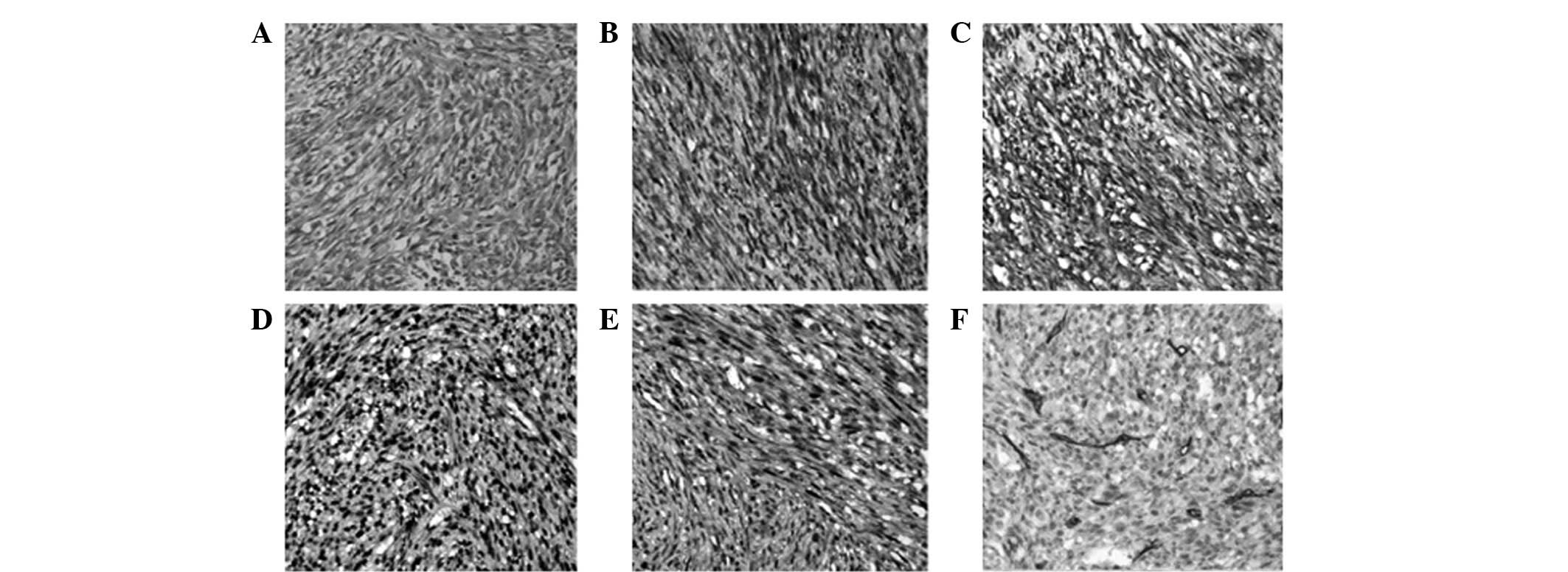
fourth) and into the sternum. The final pathology revealed
metaplastic carcinoma of the breast, predominantly composed of
scattered spindle cells with atypical mitotic features. The
immunoreactivity for the carcinoma was positive for cytokeratin,
vimentin, CD34, p63 and Ki-67 (>30%), and negative for
cytokeratin 7, SMA, desmin and S-100 (Fig. 2). Pathological examination indicated
the presence of invading cancer cells in all three resected
axillary lymph nodes. At 16 days post-surgery, local recurrence was
observed in the right chest wall, coupled with the emergence of
three satellite lesions (~1 cm in diameter). Due to the inoperable
nature of the disease, the patient was referred to the Department
of Oncology for palliative chemotherapy with capecitabine (2.5
g/m2 twice daily for 30 days) but succumbed to the
disease after 12 weeks.
Discussion
IMT has been detected in multiple locations,
including the lungs, abdomen, pelvis, trunk, peripheral nerves and
soft tissue (2,3). IMT of the breast, however, is an
extremely rare entity and only a few cases have been reported in
the English language literature (7,8). No
specific signs or symptoms have been associated with IMT, and the
exact diagnosis is usually based on pathological and
immunohistochemical findings following resection of the tumor. The
neoplastic nature of IMT (benign or malignant) remains a subject of
debate. Idrees et al (9)
reported two cases of benign laryngeal IMTs that appeared
clinically as large infiltrating masses. Similarly, Ezzine-Baccari
et al (10) described a
benign pulmonary IMT with locally aggressive behavior. However,
local recurrence and distant metastases are also encountered in
certain cases of IMT (4). Due to
the tendency towards local recurrence and the small risk of distant
metastasis, IMT is classified as a tumor of intermediate biological
potential by the World Health Organization (11). Rapid tumor growth and a high Ki-67
labeling index are associated with the aggressive behavior. The
small tumor size (<3 cm) is regarded as a favorable prognostic
factor for overall survival in patients with pulmonary IMT
(12). In the present case, the
tumor mass rapidly enlarged in size and a high Ki-67 labeling index
was observed (30–40%). The tumor was positive for CD68, a
macrophage-specific marker, indicating a pronounced infiltration of
macrophages; accumulating evidence has linked tumor-associated
macrophages and tumor progression (13). These findings indicate an aggressive
potential of the IMT.
Although relatively rare, several cases of IMT with
malignant progression have been reported. For example, Carillo
et al (4) described a case
of IMT of the bladder with rapid malignant progression, where
multiple lymph node, bone and soft tissue metastases were observed
on positron emission tomography. Malignant transformation of the
IMT was also observed. Local recurrence with axillary lymph node
metastases occurred even after total mastectomy. Histologically,
the recurrent tumor mass was consistent with a metaplastic
carcinoma, which was predominantly composed of spindle cells with
atypical mitotic features. Furthermore, the immunostaining findings
demonstrated that such malignant transformation was accompanied by
high immunoreactivity for CD34 and p63. CD34 is a sensitive marker
of the vascular endothelium and strong CD34 staining is usually
associated with tumor relapse or metastasis (14). p63 is a p53 homolog that is
expressed in a variety of normal epithelial tissues and epithelial
malignancies. It has been documented that p63 serves as a sensitive
and specific myoepithelial marker in benign and malignant breast
lesions (15). Taken together,
these pathological results confirm a malignant nature of a
recurrent tumor.
Cytokeratin is a surface marker expressed on
epithelial cells, while vimentin is a member of the intermediate
filament family and is expressed in mesenchymal cells. In the
present case, the recurrent tumors prior to and following total
mastectomy consistently demonstrated strong immunostaining for
vimentin. By contrast, cytokeratin immunoreactivity was only
observed in the recurrent tumor following surgery. The concurrent
positive immunostaining for cytokeratin and vimentin indicated
mixed epithelial- and mesenchymal-type tumor cells in the malignant
neoplasm following surgery. The acquired expression of cytokeratin
may indicate its critical role in the malignant transformation of
IMT of the breast. Cytokeratin expression has also been found to be
associated with aggressive potential and a poor prognosis in
numerous malignancies, including breast (16) and laryngeal cancer (17), which further validates this
hypothesis.
Surgery remains the first-line treatment option for
IMT. A pre-operative evaluation, aiming to differentiate between
benign and malignant lesions, is critical for selecting a surgical
modality. There is currently no reliable biomarker for predicting
the nature of IMT. However, the results of the present case
indicated that rapid tumor development and a high Ki-67 labeling
index may be indicators for extended radical mastectomy. Complete
surgical excision is critical for achieving a good prognosis in
patients with IMT. Additionally, long-term follow-up is mandatory,
as certain cases may have the potential for malignant
transformation.
In conclusion, in the present case of IMT of the
breast, malignant transformation to a metaplastic carcinoma of the
spindle-cell type was observed following surgical intervention.
Such malignant progression may be ascribed to incomplete initial
surgical resection due to misdiagnosis as a benign lesion.
Therefore, differentiation between aggressive and non-aggressive
forms of IMT is critical in the choice of surgical approaches.
Rapid tumor growth and a high Ki-67 labeling index may indicate a
high risk of recurrence.
References
|
1
|
Saab ST, Hornick JL, Fletcher CD, Olson SJ
and Coffin CM: IgG4 plasma cells in inflammatory myofibroblastic
tumor: inflammatory marker or pathogenic link? Mod Pathol.
24:606–612. 2011.
|
|
2
|
Jain A, Kasana S, Ramrakhiani D and Sharma
M: Inflammatory myofibroblastic tumor of the stomach in an adult
female - report of a rare case and review of the literature. Turk J
Gastroenterol. 23:399–405. 2012.
|
|
3
|
Gleason BC and Hornick JL: Inflammatory
myofibroblastic tumours: where are we now? J Clin Pathol.
61:428–437. 2008.
|
|
4
|
Carillo C, Anile M, De Giacomo T and
Venuta F: Bilateral simultaneous inflammatory myofibroblastic tumor
of the lung with distant metastatic spread. Interact Cardiovasc
Thorac Surg. 13:246–247. 2011.
|
|
5
|
Kovach SJ, Fischer AC, Katzman PJ, Salloum
RM, Ettinghausen SE, Madeb R and Koniaris LG: Inflammatory
myofibroblastic tumors. J Surg Oncol. 94:385–391. 2006.
|
|
6
|
Chavez C and Hoffman MA: Complete
remission of ALK-negative plasma cell granuloma (inflammatory
myofibroblastic tumor) of the lung induced by celecoxib: A case
report and review of the literature. Oncol Lett. 5:1672–1676.
2013.
|
|
7
|
Zhao HD, Wu T, Wang JQ, et al: Primary
inflammatory myofibroblastic tumor of the breast with rapid
recurrence and metastasis: A case report. Oncol Lett. 5:97–100.
2013.
|
|
8
|
Khanafshar E, Phillipson J, Schammel DP,
Minobe L, Cymerman J and Weidner N: Inflammatory myofibroblastic
tumor of the breast. Ann Diagn Pathol. 9:123–129. 2005.
|
|
9
|
Idrees MT, Huan Y, Woo P and Wang BY:
Inflammatory myofibroblastic tumor of larynx: a benign lesion with
variable morphological spectrum. Ann Diagn Pathol. 11:433–439.
2007.
|
|
10
|
Ezzine-Baccari S, Bacha D and Sassi S,
Abouda M, Ghrairi H, Touinsi H and Sassi S: Inflammatory
myofibroblastic tumor of the lung: a benign lesion with aggressive
behavior. Gen Thorac Cardiovasc Surg. 60:531–533. 2012.
|
|
11
|
Fletcher CD, Unni KK and Mertens F: World
Health Organization Classification of Tumors. Pathology and
Genetics of Soft Tissue and Bone. IARC Press; Lyon: pp. 91–93.
2002
|
|
12
|
Melloni G, Carretta A, Ciriaco P, et al:
Inflammatory pseudotumor of the lung in adults. Ann Thorac Surg.
79:426–432. 2005.
|
|
13
|
Obeid E, Nanda R, Fu YX and Olopade OI:
The role of tumor-associated macrophages in breast cancer
progression (Review). Int J Oncol. 43:5–12. 2013.
|
|
14
|
Nielsen JS and McNagny KM: Novel functions
of the CD34 family. J Cell Sci. 121:3683–3692. 2008.
|
|
15
|
Stefanou D, Batistatou A, Nonni A,
Arkoumani E and Agnantis NJ: p63 expression in benign and malignant
breast lesions. Histol Histopathol. 19:465–471. 2004.
|
|
16
|
Brotherick I, Robson CN, Browell DA, et
al: Cytokeratin expression in breast cancer: phenotypic changes
associated with disease progression. Cytometry. 32:301–308.
1998.
|
|
17
|
Negm H, Mosleh M, Fathy H, Hareedy A and
Elbattawy A: Cytokeratin immunohistochemically detected nodal
micrometastases in N0 laryngeal cancer: impact on the overall
occult metastases. Eur Arch Otorhinolaryngol. 270:1085–1092.
2013.
|