Introduction
Breast cancer is one of the most common types of
malignant tumor worldwide and is the second leading cause of
cancer-related mortality among females (1). Genetic alterations, environmental
toxins, hormones, diet and stress are the predominant causes of
breast cancer. Although improved early detection and effective
treatment may help to prolong the survival times of breast cancer
patients, numerous patients succumb to the disease as a result of
invasion and metastasis (2).
Therefore, it is important to identify effective predictive
biomarkers to provide more accurate diagnoses and to develop novel
therapeutic strategies.
MicroRNAs (miRNAs) are a class of short (18–24
nucleotides), non-protein-coding RNAs that bind to the 3′
untranslated regions (3′ UTRs) of target mRNAs to regulate gene
expression by inhibiting the translation of target mRNAs or by
promoting transcript degradation (3–5). A
number of studies have found that miRNAs are important in a number
of biological processes, including cell differentiation,
proliferation, apoptosis and metabolism (6). miRNAs are also involved in the process
of cancer development, progression and metastasis, exhibiting
oncogenic or tumor suppressor functions (7). For example, miR-34a expression is
reduced in neuroblastoma and acts as a tumor suppressor (8); however, miR-155 is overexpressed in
chronic lymphocytic leukemia and acts as an oncogene (9).
Previous studies have revealed that miR-320a
exhibits abnormal expression levels in multiple malignancies and is
involved in the formation, progression and metastasis of cancer.
Sun et al (10) reported
that miR-320a suppressed human colon cancer cell proliferation by
directly targeting β-catenin. miR-320a also inhibits tumor invasion
by targeting neuropilin-1 and is associated with liver metastasis
in colorectal cancer (11).
However, Xu et al (12)
reported that miR-320a was upregulated two- to 14-fold in prostate
cancer cells, and may exhibit an oncogenic function in prostate
cancer. Recently, Xu et al (13) revealed that miR-320a was a
potentially valuable biomarker for diagnosing older females with
gastric cancer. However, few studies have investigated the
clinicopathological value and prognostic significance of miR-320a
expression in breast cancer.
In the present study, the miR-320a expression levels
in 15 in situ breast carcinoma and 130 invasive breast
cancer samples were examined using chromogenic in situ
hybridization. The results demonstrated that miR-320a was
downregulated in invasive breast cancer. Furthermore, low miR-320a
expression was found to be associated with invasive breast cancer
progression and predicts poor patient prognosis.
Materials and methods
Patients and tissue samples
Paraffin-embedded invasive breast cancer samples
from 130 patients (mean age, 55.7 years; range, 34–87 years) were
obtained between January 1999 and December 2002. A total of 15
paraffin-embedded in situ breast carcinoma tissues were
collected in 2011. All tissues were obtained from Huashan Hospital
of Fudan University (Shanghai, China). None of the 130 invasive
breast cancer patients received chemotherapy or radiation therapy
prior to surgery. The study was approved by the ethical committee
of Huashan Hospital, Fudan University (Shanghai, China), and all
patients provided written informed consent.
A total of 102 (78.5%) invasive ductal carcinomas,
15 (11.5%) lobular carcinomas, eight (6.2%) medullary carcinomas
and five (3.8%) mucinous adenocarcinomas were identified among the
130 invasive breast cancer samples. The clinical tumor lymph node
metastasis (TNM) stage of each cancer was based on the World Health
Organization guidelines (14), and
the histological grade was classified according to
Scarff-Bloom-Richardson grading (15). All 130 cases were followed-up after
surgery, and the final date of follow-up was December 31, 2008. The
mean duration of follow-up was 77.5 months. The overall survival
rates were calculated from the date of resection to the follow-up
deadline or date of mortality. The clinicopathological
characteristics of the patients and follow-up data are shown in
Table I.
 | Table IClinicopathological characteristics
and follow-up data of 130 invasive breast cancer patients. |
Table I
Clinicopathological characteristics
and follow-up data of 130 invasive breast cancer patients.
| Characteristics | Number of
patients/total number (%) |
|---|
| Age (years)a | 55.7 (34–87) |
| Histological
type |
| Invasive ductal | 102/130 (78.5) |
| Lobular | 15/130 (11.5) |
| Medullary | 8/130 (6.2) |
| Mucinous | 5/130 (3.8) |
| Histological
grade |
| Low (I) | 14/130 (10.8) |
| Intermediate
(II) | 93/130 (71.5) |
| High (III) | 23/130 (17.7) |
| Tumor size (cm) |
| ≤3.5 | 79/130 (60.8) |
| >3.5 | 51/130 (39.2) |
| Lymph node
metastasis |
| 0 | 71/130 (54.6) |
| 1–2 | 32/130 (24.6) |
| >2 | 27/130 (20.8) |
| Distant
metastasis |
| Yes | 12/130 (9.2) |
| No | 118/130 (90.8) |
| Clinical TNM
stage |
| I | 44/130 (33.8) |
| II | 54/130 (41.6) |
| III–IV | 32/130 (24.6) |
| Estrogen
receptor |
| − | 61/130 (46.9) |
| + | 69/130 (53.1) |
| Progesterone
receptor |
| − | 75/130 (57.7) |
| + | 55/130 (42.3) |
| C-erbB-2
expression |
| − | 50/130 (38.5) |
| + | 80/130 (61.5) |
| Menopause |
| No | 50/130 (38.5) |
| Yes | 80/130 (61.5) |
| Alive with
cancer | 103/130 (79.2) |
| Succumbed to
cancer | 27/130 (20.8) |
Chromogenic in situ hybridization
(CISH)
Chromogenic in situ hybridization (CISH) was
used to detect miR-320a expression levels in 15 paraffin-embedded
in situ breast carcinoma and 130 invasive breast cancer
samples. Briefly, following dewaxing in xylene and rehydrating in
graded alcohol, the slides were digested with pepsin. The slides
were then prehybridized in a prehybridization solution at 54°C for
2 h. Following prehybridization, 5′digoxin-conjugated locked
nucleic acid probes for miR-320a, U6 (positive control) and
scrambled RNA (negative control) (all Exiqon, Copenhagen, Denmark)
were used for hybridization at 54°C for 16–20 h. Following washing
with Tris-buffered saline, the slides were incubated with a sheep
polyclonal anti-digoxin antibody (Roche Diagnostics GmbH, Mannheim,
Germany). Next, the slides were stained with nitro blue
tetrazolium/5-bromo-4-chloro-3-indolyl-phosphate. Methyl green was
used to counterstain the nuclei. Positive results appeared blue in
the cytoplasm and nuclei.
The slides were scored independently by two
pathologists, and positive nuclear and cytoplasmic miR-320a
expression was detected. The proportion of positively stained tumor
cells and the staining intensity were evaluated over 10 visual
fields (magnification, ×40; BX-51, Olympus America Inc., Melville,
NY, USA). For statistical analysis, with reference to Tang et
al (16), total staining of
miR-320a was analyzed based on the proportion of positively stained
tumor cells identified, and the following four scores were used: 0,
no positive tumor cells; 1, <10% positive tumor cells; 2, 10–50%
positive tumor cells; and 3, >50% positive tumor cells. The
staining intensity was also analyzed according to four scores: 0,
no staining; 1, light blue/weak staining; 2, blue/moderate
staining; and 3, dark blue/strong staining. The staining index (SI)
was calculated using the following formula: SI = staining intensity
× proportion of positively stained tumor cells. Using the
aforementioned method, the expression of miR-320a was scored as 0,
1, 2, 3, 4, 6 or 9. An SI score of 4 was selected as a cut-off
value based on a measurement of heterogeneity with the log-rank
test statistic with respect to overall survival (16,17),
and the expression levels of miR-320a were defined as high (SI≥4)
or low (SI<4).
Statistical analysis
Statistical analyses were performed using SPSS,
version 19.0 (SPSS, Inc., Chicago, IL, USA). The χ2 test
and Fisher’s exact test were used to analyze the association
between miR-320a expression and clinicopathological features.
Survival curves were generated using the Kaplan-Meier method and
compared using the log-rank test. Variables with P<0.05 in the
univariate analysis were entered into the Cox regression analysis,
and the multivariate analysis used the Cox proportional-hazards
model. Receiver operating characteristic (ROC) curves were
generated using MedCalc, version 10.4.7.0 (MedCalc, Mariakerke,
Belgium). P<0.05 was considered to indicate a statistically
significant difference.
Results
miR-320a expression in invasive breast
cancer and in situ breast carcinoma
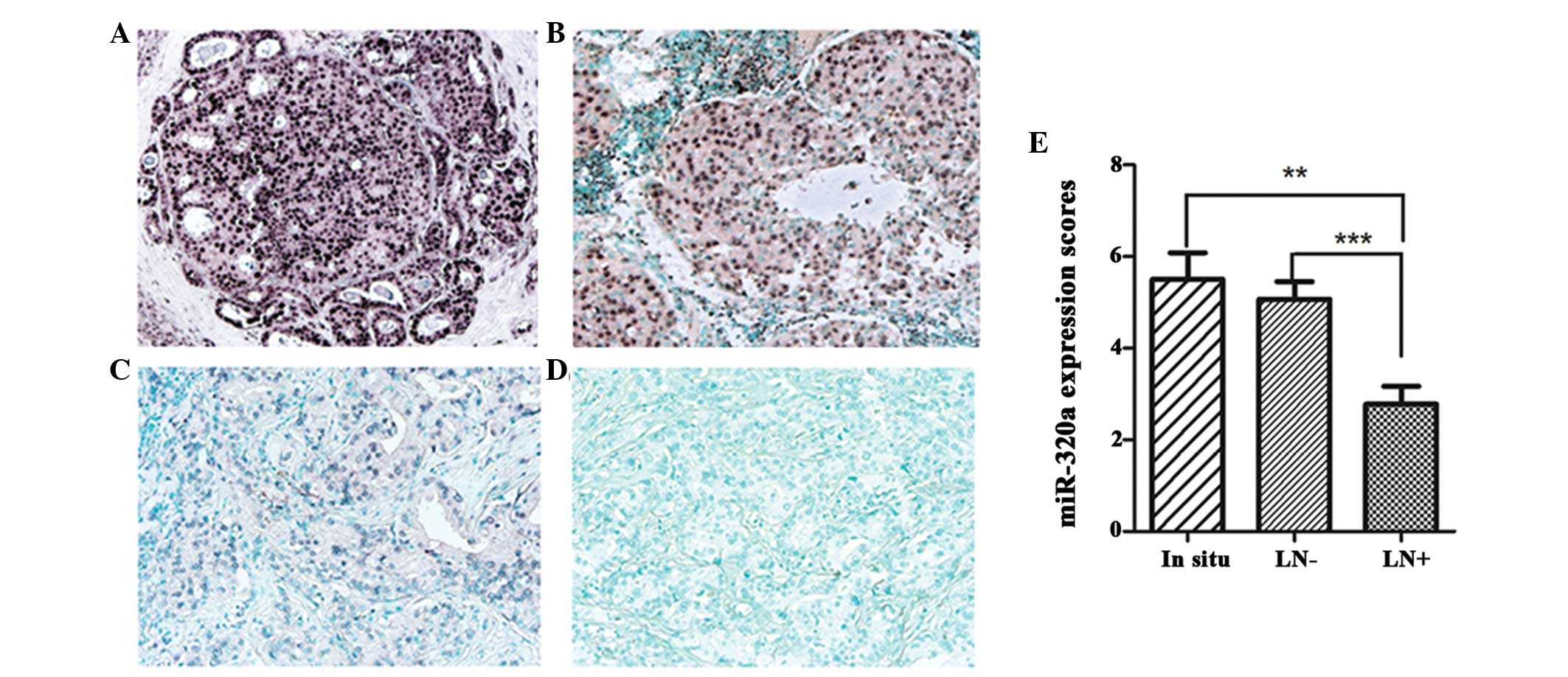
CISH was used to detect miR-320a expression in 15
in situ breast carcinoma and 13 invasive breast cancer
tissues. miR-320a expression was observed in the nuclei and
cytoplasm, predominately in luminal epithelial cells (Fig. 1). High miR-320a expression (SI≥4)
was detected in 12/15 (80%) in situ breast carcinoma and
60/130 (46%) invasive breast cancer samples. In addition, levels of
miR-320a expression in invasive breast cancer with lymph node
metastasis were found to be significantly lower than levels for
breast cancer without lymph node metastasis and in situ
breast carcinoma (P<0.01; Fig.
1E). However, no significant differences were identified
between in situ breast carcinoma and invasive breast cancer
without lymph node metastasis. These results suggest that
downregulated miR-320a expression may be involved in cancer
progression.
Correlation between miR-320a expression
and clinicopathological characteristics in invasive breast
cancer
To further evaluate whether low miR-320a expression
was associated with the progression of breast cancer, we analyzed
the correlation between miR-320a expression levels and the
clinicopathological characteristics of 130 invasive breast cancer
patients (Table II). It was found
that miR-320a was downregulated in patients with a larger tumor
size (P=0.046), more advanced clinical staging (P<0.001) and
increased lymph node metastases (P<0.001), as well as the
presence of distant metastasis (P=0.006). However, no significant
differences were identified between the expression levels of
miR-320a and age (P=0.164), histological grade (P=0.745), menopause
(P=0.697), human epidermal growth factor-2 (HER-2) expression
(P=0.290), estrogen receptor (ER) status (P=0.684) or progesterone
receptor (PR) status (P=0.352).
| Table IICorrelation between miR-320a
expression and clinicopathological characteristics in invasive
breast cancer (n=130). |
Table II
Correlation between miR-320a
expression and clinicopathological characteristics in invasive
breast cancer (n=130).
| miR-320a
expression | |
|---|
|
| |
|---|
| Characteristics | High expression, n
(%) | Low expression, n
(%) | P-value |
|---|
| Age (years) | | | 0.164 |
| <45 | 9 (60) | 6 (40) | |
| 45–55 | 23 (38) | 38 (62) | |
| >55 | 28 (52) | 26 (48) | |
| Tumor size (cm) | | | 0.046 |
| ≤2.5 | 42 (53) | 37 (47) | |
| >2.5 | 18 (35) | 33 (65) | |
| Lymph node
metastasis | | | <0.001 |
| 0 | 46 (65) | 25 (35) | |
| 1–2 | 10 (31) | 22 (69) | |
| >2 | 4 (15) | 23 (85) | |
| Distant
metastasis | | | 0.006 |
| No | 59 (50) | 59 (50) | |
| Yes | 1 (8.3) | 11 (91.7) | |
| Histological
grade | | | 0.745 |
| Low (I) | 7 (50) | 7 (50) | |
| Intermediate
(II) | 44 (47) | 49 (53) | |
| High (III) | 9 (39) | 14 (61) | |
| Clinical TNM
stage | | | <0.001 |
| I | 28 (64) | 16 (36) | |
| II | 27 (50) | 27 (50) | |
| III–IV | 5 (16) | 27 (84) | |
| Estrogen
receptor | | | 0.684 |
| − | 27 (44) | 34 (56) | |
| + | 33 (48) | 36 (52) | |
| Progesterone
receptor | | | 0.352 |
| − | 32 (43) | 43 (57) | |
| + | 28 (51) | 27 (49) | |
| HER-2
expression | | | 0.290 |
| − | 26 (52) | 24 (48) | |
| + | 34 (42.5) | 46 (57.5) | |
| Menopause | | | 0.697 |
| No | 22 (44) | 28 (56) | |
| Yes | 38 (47.5) | 42 (52.5) | |
Low expression levels of miR-320a
correlate with poor prognosis in 130 invasive breast cancer
patients
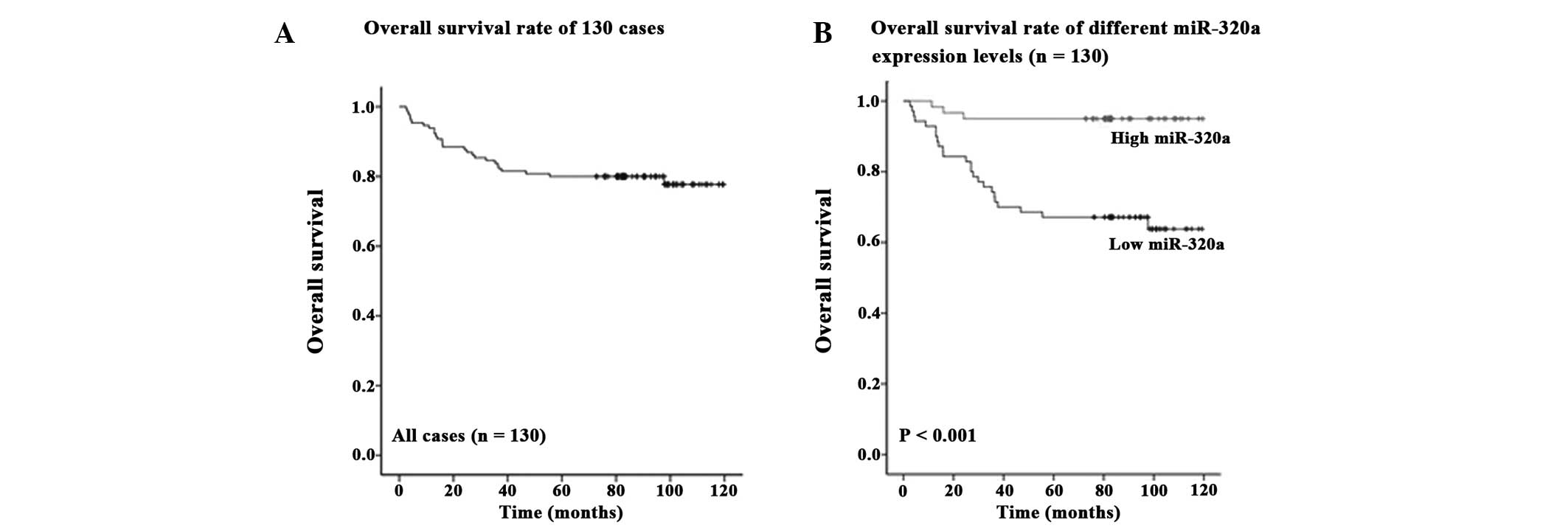
The prognostic value of miR-320a expression levels
was evaluated in 130 invasive breast cancer patients using
Kaplan-Meier analysis and the log-rank test. Among the 130 invasive
breast cancers patients, 57/60 (95%) patients with high miR-320a
expression survived, whereas 46/70 (66%) patients with low miR-320a
expression survived. The overall survival rate of the 130 invasive
breast cancer patients was 79% (Fig.
2A), and the overall survival rate of invasive breast cancer
patients with low miR-320a expression levels was significantly
shorter than that in patients with high miR-320a expression
(P<0.001; Fig. 2B).
Using univariate survival analysis, the clinical TNM
stage (P=0.010), menopause (P=0.020), miR-320a expression level
(P=0.015) and distant metastasis (P=0.001) were found to be
significantly associated with prognosis, however, no significant
differences were identified between prognosis and age (P=0.587),
lymph node metastasis (P=0.076), chemotherapy (P=0.900), tumor size
(P=0.230), histological grade (P=0.977), ER expression (P=0.802),
PR expression (P=0.445) or HER-2 expression (P=0.650) (Table III). Multivariate analyses were
then used to determine whether miR-320a expression levels were an
independent prognostic predictor of clinical outcomes. The results
revealed that a decrease in miR-320a expression [hazard ratio
(HR)=0.221; 95% confidence interval (CI), 0.050–0.979; P=0.047] and
clinical TNM stage (HR, 4.434; 95% CI, 2.308–8.522; P<0.001)
(Table III) showed significant
prognostic effects on overall survival. Thus, these results
indicated that miR-320a expression levels were significantly
associated with invasive breast cancer patient prognosis.
| Table IIIUnivariate and multivariate analysis
for overall survival in invasive breast cancer patients
(n=130). |
Table III
Univariate and multivariate analysis
for overall survival in invasive breast cancer patients
(n=130).
| | Univariate
analysis | Multivariate
analysis |
|---|
| |
|
|
|---|
| Features | Subset | P-value | HR | 95% CI | P-value |
|---|
| Age | | 0.587 | | | |
| Menopause | Yes/No | 0.020 | 0.660 | 0.261–1.672 | 0.381 |
| Chemotherapy | | 0.900 | | | |
| Tumor size | ≤2.5/>2.5 | 0.230 | | | |
| Lymph node
metastasis | N0/N1–2,
>N2 | 0.076 | | | |
| Clinical TNM
stage | I/II, III, IV | 0.010 | 4.434 | 2.308–8.522 | <0.001 |
| Histological
grade | I/II, III | 0.977 | | | |
| Estrogen
receptor | −/+ | 0.802 | | | |
| Progesterone
receptor | −/+ | 0.445 | | | |
| HER-2
expression | −/+ | 0.650 | | | |
| Distant
metastasis | Yes/No | 0.001 | 0.381 | 0.130–1.119 | 0.079 |
| miR-320a | High/Low | 0.015 | 0.221 | 0.050–0.979 | 0.047 |
miR-320a is an indicator for predicting
the prognosis of advanced-stage invasive breast cancer
patients
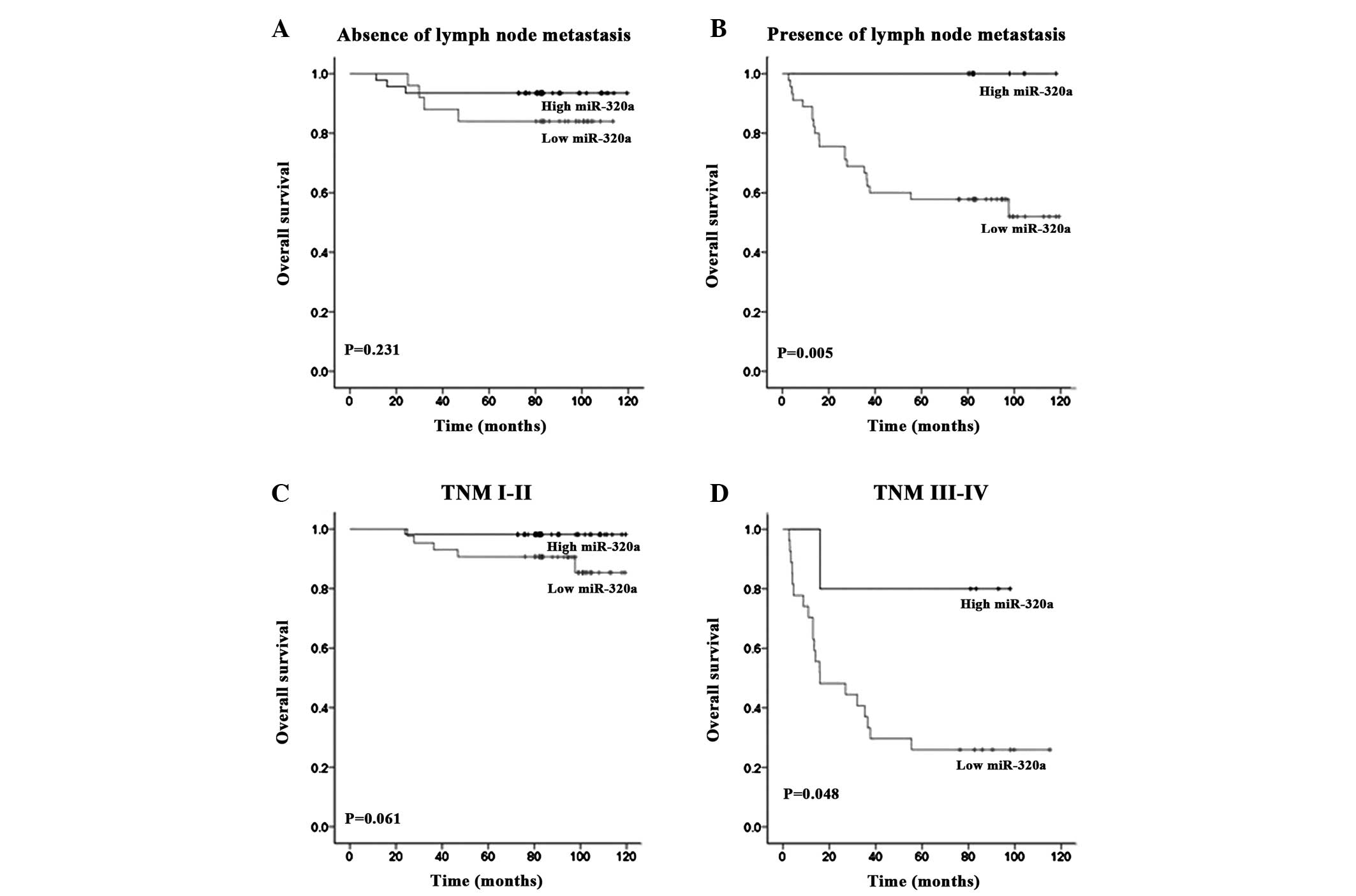
The prognostic value of miR-320a expression in
selective patient subgroups classified by clinical TNM stage and
lymph node status was evaluated. Low miR-320a expression was found
to significantly correlate with poor survival in patients with
clinical stage III–IV (P=0.048; Fig.
3D) and lymph node metastasis (P=0.005; Fig. 3B). However, no significant
differences between high and low miR-320a expression groups were
identified between invasive breast cancer patients with clinical
stage I–II (P=0.061; Fig. 3C) and
those without lymph node metastasis (P=0.231; Fig. 3A). These results indicate that
miR-320a may present an improved prognostic biomarker for
advanced-stage invasive breast cancer patients.
miR-320a more effectively predicts
invasive breast cancer prognosis when compared with commonly used
clinicopathological prognostic biomarkers
ROC curves were used to compare the sensitivity and
specificity of miR-320a expression with commonly used
clinicopathological prognostic biomarkers (ER, PR and HER-2). The
survival state of patients was used as the classification variable,
whereas ER, PR, HER-2 (negative/positive) and the expression scores
of miR-320a were used as the test variables. An area under the ROC
curve of 0.7–0.9% was considered to present improved
discrimination, whereas an ROC value of 0.5% indicated no
discrimination (18). The ROC areas
for miR-320a, ER, PR, and HER-2 were 0.710, 0.517, 0.549, and
0.574%, respectively. This result revealed that compared with
routinely applied clinical prognostic biomarkers, miR-320a alone is
a more reliable predictor for invasive breast cancer prognosis
(Fig. 4).
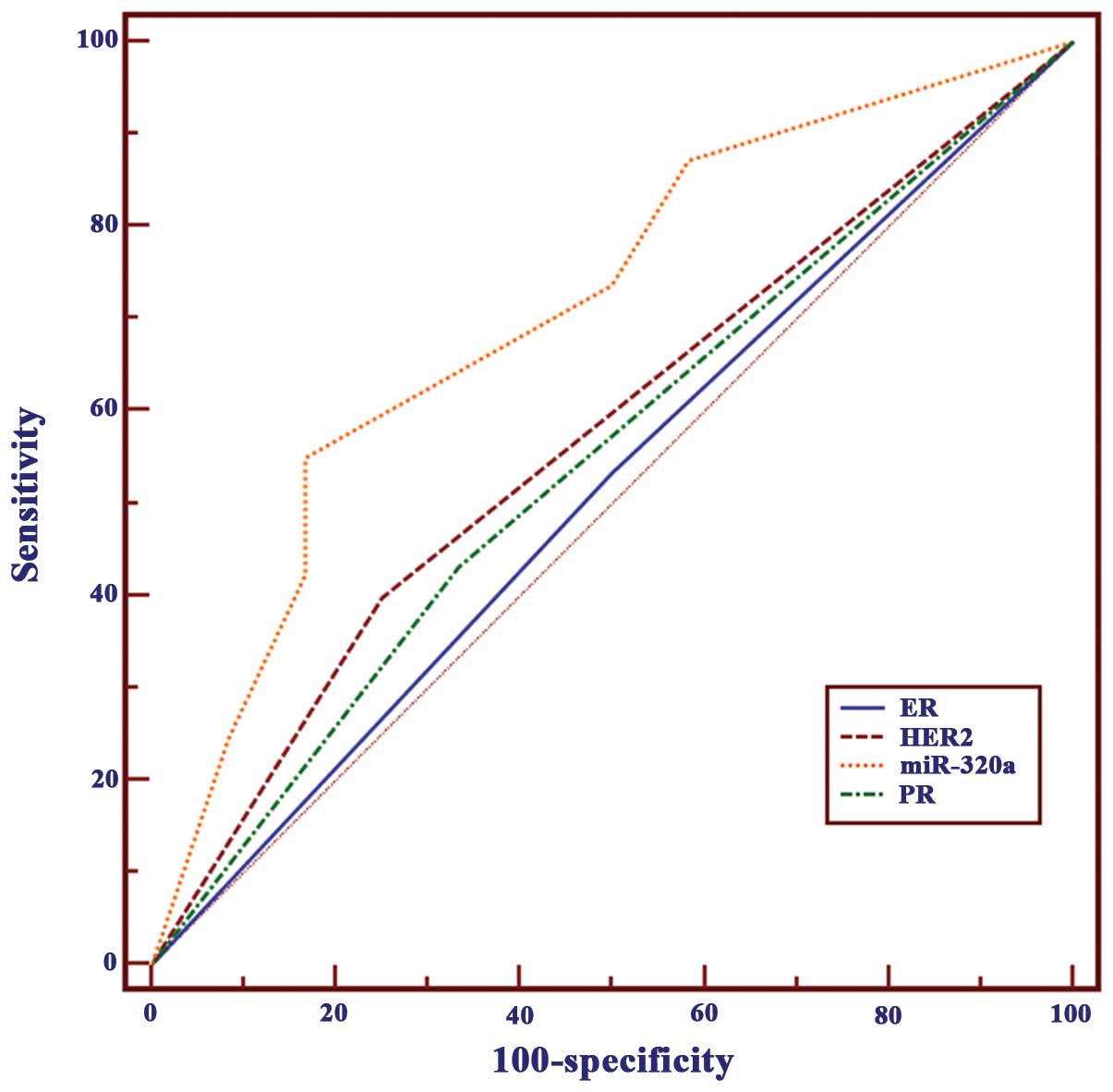 | Figure 4Comparison of miR-320a with commonly
used prognostic parameters using ROC curves. The ROC areas under
the curve for miR-320a, ER, PR and HER-2 were 0.710, 0.517, 0.549
and 0.574, respectively. miR-320a, microRNA-320a; ROC, receiver
operating characteristic; ER, estrogen receptor; PR, progesterone
receptor; HER-2, human epidermal growth factor. |
Discussion
miRNA profiles have been established for numerous
solid and hematologic malignancies (19). In particular, miR-320a has been
reported to be important in a number of cancer types (20–22);
however, the association between clinicopathological
characteristics and survival in breast cancer remains unclear. In
the present study, miR-320a expression in 15 paraffin-embedded
in situ breast carcinoma and 130 invasive breast cancer
tissues was evaluated using CISH. miR-320a expression levels were
found to be lower in invasive breast cancer when compared with
in situ breast carcinoma, which suggested that miR-320a may
be associated with the progression of breast cancer. However, no
significant association was identified between in situ
breast carcinoma and invasive breast cancer without lymph node
metastasis. These observations indicated that miR-320a may be
involved in the later stages of cancer progression rather than
primary tumor formation.
Breast cancer is a complex, heterogeneous disease
and, thus, an urgent requirement remains to identify more effective
biomarkers to predict patient prognosis. Over the past decade, an
increasing number of biological parameters have been identified as
being involved in the prognosis of breast cancer (23). ER is important in the carcinogenic
process, and acts as a powerful prognostic factor for breast cancer
patients (24). PR, an
estrogen-regulated gene, exhibits a function in the ER pathway
(18), and the presence of PR is
associated with a lower frequency of metastasis. HER-2 is a member
of the epidermal growth factor receptor (EGFR) family (25), which has also been used to predict
the prognosis of breast cancer (26,27).
However, according to the results of the current study, ER, PR and
HER-2 exhibited no prognostic value for breast cancer patients,
which was consistent with the results of previous studies (18,28,29).
These observations, however, appeared to be inconsistent with those
that suggest ER, PR and HER-2 may predict clinical outcome for
breast cancer patients. The reason for this discrepancy is unclear
and may be due to sample size and regional differences.
Furthermore, this inconsistency demonstrates the complexity and
heterogeneity of breast cancer. There is an urgent requirement for
the identification of more effective biomarkers to predict patient
prognosis.
Considering that miRNAs are only 18–24 nucleotides
in length, they are robustly stable in formalin-fixed
parraffin-embedded tissues. Previous studies have suggested that
introducing miRNAs as biomarkers into clinical practice is
beneficial, as miRNA data provides more reliable results than mRNA
profiles (30,31). miR-150 may be considered as a
potential prognosis biomarker in colorectal cancer therapy outcome
(32). The overexpression of miR-21
predicts limited survival in patients with node-negative disease
(19). In the present study,
following the analysis of miR-320a expression in 130 invasive
breast cancers, the correlation between miR-320a and patient
prognosis was determined. The results showed that miR-320a had a
potential function in predicting poor outcomes for invasive breast
cancer patients. This result was confirmed using univariate and
multivariate survival analyses, whereby low miR-320a expression was
found to be an independent prognostic predictor of poor survival.
In addition, miR-320a showed improved discrimination when compared
with ER, PR and HER-2, by using an ROC curve (the ROC areas under
the curve for miR-320a, ER, PR and HER-2 were 0.710, 0.517, 0.549
and 0.574, respectively). This result clearly suggests that
miR-320a is a more reliable predictor for invasive breast cancer
prognosis than commonly used biomarkers.
In addition to these results, the prognostic value
of miR-320a expression in invasive breast cancer subgroups
classified by lymph node metastasis status and clinical TNM stage
were also analyzed. The results revealed that low miR-320a
expression was associated with a poor prognosis in patients with
clinical TNM stage III–IV and lymph node metastasis. Thus, it may
be hypothesized that miR-320a may have increased prognostic value
for advanced-stage invasive breast cancer. However, the subgroups
of patients in this study were small and, therefore, a large study
to confirm these data is necessary.
In conclusion, the results of this study indicated
that miR-320a expression is significantly associated with the
progression and prognosis of invasive breast cancer. Notably,
miR-320a appears to be a better prognostic biomarker for invasive
breast cancer than commonly used prognostic parameters. Further
studies are required to investigate the function and the detailed
mechanism of miR-320a in breast cancer.
Acknowledgements
This study was supported by grants from the National
Nature Science Foundation of China (grant nos. 81272387 and
81071813). The authors would like to thank the members of the
laboratory for helpful discussions.
References
|
1
|
Yu G, Liu G, Dong J and Jin Y: Clinical
implications of CIP2A protein expression in breast cancer. Med
Oncol. 30:5242013.
|
|
2
|
Wu ZS, Wu Q, Wang CQ, et al: MiR-339-5p
inhibits breast cancer cell migration and invasion in vitro and may
be a potential biomarker for breast cancer prognosis. BMC Cancer.
10:5422010.
|
|
3
|
Hanna JA, Hahn L, Agarwal S and Rimm DL:
In situ measurement of miR-205 in malignant melanoma tissue
supports its role as a tumor suppressor microRNA. Lab Invest.
92:1390–1397. 2012.
|
|
4
|
Shenouda SK and Alahari SK: MicroRNA
function in cancer: oncogene or a tumor suppressor? Cancer Metast
Rev. 28:369–378. 2009.
|
|
5
|
Wu W, Takanashi M, Borjigin N, et al:
MicroRNA-18a modulates STAT3 activity through negative regulation
of PIAS3 during gastric adenocarcinogenesis. Br J Cancer.
108:653–661. 2013.
|
|
6
|
Wu ZS, Wu Q, Wang CQ, et al: miR-340
inhibition of breast cancer cell migration and invasion through
targeting of oncoprotein c-Met. Cancer. 117:2842–2852. 2011.
|
|
7
|
Zhang B, Pan X, Cobb GP and Anderson TA:
microRNAs as oncogenes and tumor suppressors. Dev Biol. 302:1–12.
2007.
|
|
8
|
Welch C, Chen Y and Stallings RL:
MicroRNA-34a functions as a potential tumor suppressor by inducing
apoptosis in neuroblastoma cells. Oncogene. 26:5017–5022. 2007.
|
|
9
|
Gartel AL and Kandel ES: miRNAs: Little
known mediators of oncogenesis. Semin Cancer Biol. 18:103–110.
2008.
|
|
10
|
Sun JY, Huang Y, Li JP, et al:
MicroRNA-320a suppresses human colon cancer cell proliferation by
directly targeting β-catenin. Biochem Biophys Res Commun.
420:787–792. 2012.
|
|
11
|
Zhang Y, He X, Liu Y, et al: microRNA-320a
inhibits tumor invasion by targeting neuropilin 1 and is associated
with liver metastasis in colorectal cancer. Oncol Rep. 27:685–694.
2012.
|
|
12
|
Xu G, Wu J, Zhou L, et al:
Characterization of the small RNA transcriptomes of androgen
dependent and independent prostate cancer cell line by deep
sequencing. PLoS One. 5:e155192010.
|
|
13
|
Xu Q, Dong QG, Sun LP, et al: Expression
of serum miR-20a-5p, let-7a, and miR-320a and their correlations
with pepsinogen in atrophic gastritis and gastric cancer: a
case-control study. BMC Clin Pathol. 13:112013.
|
|
14
|
Tavassoli FA and Devilee P: World Heatlh
Organization Classification of Tumours. Pathology and Genetics,
Tumors of the Breast and Female Genital Organs. IARC Press; Lyon:
pp. 102003
|
|
15
|
Allred DC, Wu Y, Mao S, et al: Ductal
carcinoma in situ and the emergence of diversity during breast
cancer evolution. Clin Cancer Res. 14:370–378. 2008.
|
|
16
|
Tang W, Zhu J, Su S, et al: MiR-27 as a
prognostic marker for breast cancer progression and patient
survival. PLoS One. 7:e517022012.
|
|
17
|
Nie Y, Liu X, Qu S, et al: Long non-coding
RNA HOTAIR is an independent prognostic marker for nasopharyngeal
carcinoma progression and survival. Cancer Sci. 104:458–464.
2013.
|
|
18
|
Cao XX, Xu JD, Liu XL, et al: RACK1: A
superior independent predictor for poor clinical outcome in breast
cancer. Int J Cancer. 127:1172–1179. 2010.
|
|
19
|
Dillhoff M, Liu J, Frankel W, et al:
MicroRNA-21 is overexpressed in pancreatic cancer and a potential
predictor of survival. J Gastrointest Surg. 12:2171–2176. 2008.
|
|
20
|
Diakos C, Zhong S, Xiao Y, et al: TEL-AML1
regulation of survivin and apoptosis via miRNA-494 and miRNA-320a.
Blood. 116:4885–4893. 2010.
|
|
21
|
Hummel R, Wang T, Watson DI, et al:
Chemotherapy-induced modification of microRNA expression in
esophageal cancer. Oncol Rep. 26:1011–1017. 2011.
|
|
22
|
Salendo J, Spitzner M, Kramer F, et al:
Identification of a microRNA expression signature for
chemoradiosensitivity of colorectal cancer cells, involving
miRNAs-320a, -224, -132 and let7g. Radiother Oncol. 108:451–457.
2013.
|
|
23
|
Yu H, Giai M, Diamandis EP, et al:
Prostate-specific antigen is a new favorable prognostic indicator
for women with breast cancer. Cancer Res. 55:2104–2110. 1995.
|
|
24
|
Crowe JP, Hubay CA, Pearson OH, et al:
Estrogen receptor status as a prognostic indicator for stage I
breast cancer patients. Breast Cancer Res Treat. 2:171–176.
1982.
|
|
25
|
Marty M, Cognetti F, Maraninchi D, et al:
Randomized phase II trial of the efficacy and safety of trastuzumab
combined with docetaxel in patients with human epidermal growth
factor receptor 2-positive metastatic breast cancer administered as
first-line treatment: the M77001 study group. J Clin Oncol.
23:4265–4274. 2005.
|
|
26
|
Horiguchi J, Iino Y, Takei H, et al:
c-erbB-2 status is an independent predictor of survival after first
recurrence. Int J Oncol. 12:123–128. 1998.
|
|
27
|
Wu Y, Khan H, Chillar R and Vadgama JV:
Prognostic value of plasma HER-2/neu in African American and
Hispanic women with breast cancer. Int J Oncol. 14:1021–1037.
1999.
|
|
28
|
Fagerholm R, Sprott K, Heikkinen T, et al:
Overabundant FANCD2, alone and combined with NQO1, is a sensitive
marker of adverse prognosis in breast cancer. Ann Oncol.
24:2780–2785. 2013.
|
|
29
|
Chang J, Clark GM, Allred DC, et al:
Survival of patients with metastatic breast carcinoma: importance
of prognostic markers of the primary tumor. Cancer. 97:545–553.
2003.
|
|
30
|
Hall JS, Taylor J, Valentine HR, et al:
Enhanced stability of microRNA expression facilitates
classification of FFPE tumour samples exhibiting near total mRNA
degradation. Br J Cancer. 107:684–694. 2012.
|
|
31
|
Jung M, Schaefer A, Steiner I, et al:
Robust microRNA stability in degraded RNA preparations from human
tissue and cell samples. Clin Chem. 56:998–1006. 2010.
|
|
32
|
Ma Y, Zhang P, Wang F, et al: miR-150 as a
potential biomarker associated with prognosis and therapeutic
outcome in colorectal cancer. Gut. 61:1447–1453. 2012.
|