Introduction
Biliary disease complicated with
cholangiobronchopleural fistula has rarely been reported in the
literature. It may occur in cases of multiple hepatobiliary stones
or biliary ascariasis-associated severe infection; however, there
has been no literature in China reporting complicated
cholangiobronchopleural fistula after endoscopic retrograde
cholangiopancreatography (ERCP) (1,2). The
present study describes a case of distal cholangiocarcinoma
complicated with cholangiobronchopleural fistula in a 60-year-old
female following ERCP for this rare disease. The study was approved
by the ethics committee of the Eastern Hepatobiliary Surgery
Hospital, The Second Military Medical University (Shanghai, China),
and written informed consent was obtained from the patient.
Case report
Patient characteristics
The present study describes a 60-year-old female
patient who was admitted to the Hepatic Surgery Center at the
Eastern Hepatobiliary Surgery Hospital (Shanghai, China) on October
25, 2004 due to of icteric skin and sclera accompanied with chill
and fever for more than one month. Physical examination revealed
the following: Conscious; deep tenderness of the upper abdomen
without rebound pain; and liver and spleen not palpable under
subcostal margin. ERCP prior to admission to this hospital revealed
a space-occupying lesion of the lower segment of the common bile
duct associated with dilation of intra- and extrahepatic biliary
ducts and cholecystitis, which were consistent with computed
tomography (CT) and magnetic resonance imaging findings following
admission. Laboratory evaluation revealed that the patient’s total
billirubin (TBIL) and direct billirubin (DBIL) levels were 210.1
(normal range, 5.1–17.1 μmol/l) and 167.5 μmol/l (normal range,
0–6.0 μmol/l), respectively. A clinical diagnosis of carcinoma of
the lower segment of the common bile duct was made. Liver
protection, nutritional support and symptomatic therapies were
instituted following admission. On November 1, 2004, liver function
re-examination showed the following: TBIL, 29.4 μmol/l; DBIL, 18.1
μmol/l; aspartate aminotransferase, 100.6 U/l (normal range, 8–35
U/l); alkaline phosphatase, 907 U/l (normal range, 25–100 U/l); and
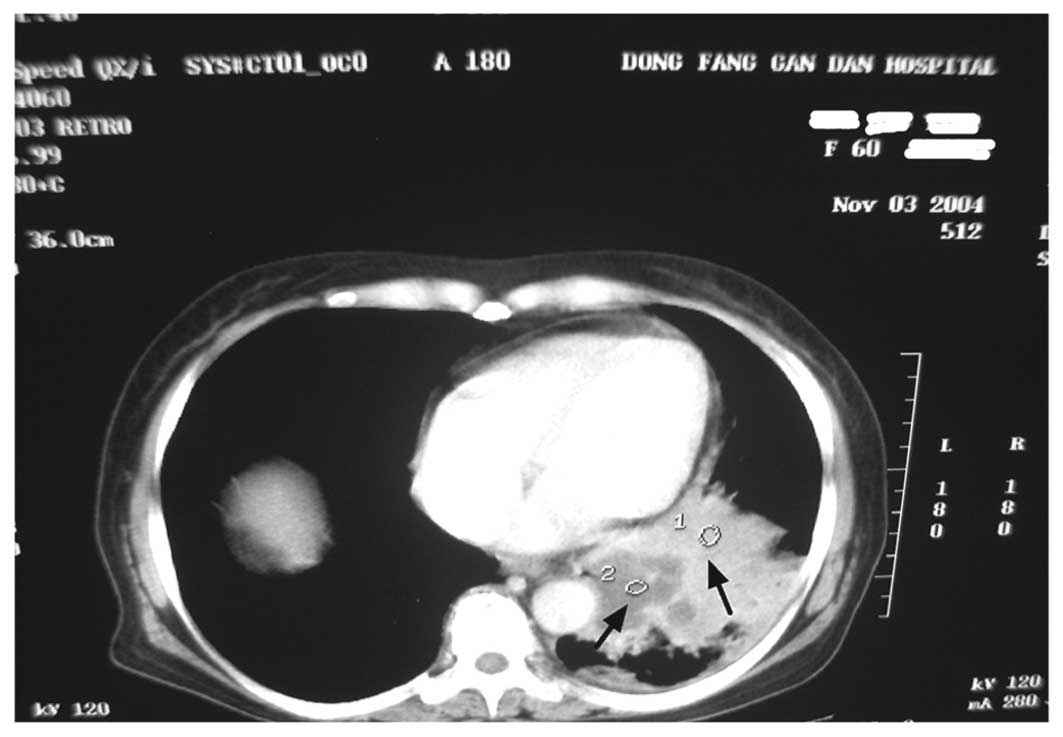
a normal albumin level of 35.5 g/l. On November 2, 2004 (the eighth
day following admission), the patient suddenly complained of chest
suffocation, shortness of breath and a cough producing ~300 ml
bile-like sputum per day. The patient did not experience fever,
nausea or vomiting. Physical examination showed icteric skin and
sclera as before; normal heart sound on auscultation; moderate
coarse rale audible in the right lung; abdomen flat and soft,
without tenderness or lump; shifting sound negative. An emergency
CT scan was performed for the chest, both lungs and the abdomen
(Fig. 1). Sputum and fistula fluid
biopsy pathological findings were bile with neutrophilic leukocyte
and lymphocytic infiltration. The diagnosis of a right
cholangiobronchopleural fistula was made.
Treatment
Based on the diagnosis, ultrasound-guided
percutaneous transhepatic cholangiodrainage (PTCD) was instituted
to eliminate jaundice, and 60 ml bile was drained promptly. The
patient fasted and therapies were instituted for inhibition of bile
secretion, reduction of bronchial mucous secretion, maintenance of
airway passage, resolution of phlegm, protection of liver function,
normalization of bile secretion, nutritional support and anti
infection. The detailed protocol was as follows: i) Subcutaneous
injection of 0.1 mg sandostatin three times a day on days 1 and 2
for inhibition of bile secretion; ii) ceftazidime pentahydrate,
ofloxacin and metronidazo1e once a day for anti-infection effects;
iii) total parenteral nutrition (TPN) support once a day; and iv)
intravenous push of 60 mg ambroxol three times a day. Following
this treatment, ~80 ml bile was drained by PTCD. The cough symptoms
improved significantly, and the bile-like substance that the
patient coughed up gradually decreased. On day 3, sandostatin (0.1
mg) was administered twice a day, and the therapies in the detailed
protocol remained unchanged. Bile drainage from PTCD reduced to
20ml daily and the cough symptoms further improved, without the
bile-like substance. At day 4, sandostatin (0.1 mg) was
administered daily, and bile drainage from PTCD reduced to 3 ml. At
day 5, sandostatin was withdrawn. The condition of the patient had
become stable by the day of surgery, without cough or bile-like
substance. On November 15, 2004, cholecystectomy and Roux-en-Y
cholangiojejunoostomy were performed with written informed consent
obtained from the patient and the patient’s family, lest the
patient should not be able to tolerate pancreatoduodenectomy.
Following discharge, the patient did not have any complaints or
associated symptoms and, on January 25, 2005, the patient was
re-admitted due to the patient’s wish for pancreatoduodenectomy.
The postoperative recovery was uneventful and the patient has since
remained in good health.
Discussion
Fistula communications between the biliary tract and
bronchopleural space are rare, but have been reported by
Dasmahapatra et al (3) in
advanced breast carcinoma. The most common cause of acquired
pleurobiliary and bronchobiliary fistula is thoracoabdominal
trauma. However, ERCP could be an incentive for
cholangiobronchopleural fistula, due to its invasive means of
examination and treatment, as observed in the current case.
According to our analysis, the present complication was likely due
to the inability to control retrograde infection following ERCP.
This resulted in dissemination of the infection, causing mixed
infection involving the diaphragm and pleura, and further
penetrating the bronchus. As ERCP is an invasive means of
examination and treatment, ERCP-associated morbidity is almost
unavoidable. For example, the occurrence of
hyperpancreatoamylasemia including acute pancreatitis (AP) after
ERCP is as high as 40–50% (4). The
most common diagnostic ERCP-associated complication is AP, and the
next is cholangitis. Hemorrhage and perforation are relatively rare
(5,6). Based on our experience in the present
case, we suggest that inhibition of bile secretion, PTCD drainage,
starvation and TPN are of primary importance, of which subcutaneous
administration of sandostatin is of vital importance.
We propose that it is possible to prevent this
complication from occurring. Positive, initiative, timely and
complete anti-infection therapy, nutritional support and drainage
(when necessary) should be considered as early as possible before
performing procedures including ERCP and surgical operation, or
treating hepatobiliary stones which are liable to cause infection,
or any other disease which may be free of infection for the time
being but may cause potential infection (7). In the case of any sign of infection,
the cause should be sought as soon as possible and dealt with
immediately. However, as we only have experience of one case of
hepatobiliary disease-complicated cholangiobronchopleural fistula,
further study is necessary to gain more experience in dealing with
such a complication.
Acknowledgements
The present study was supported by the China
Postdoctoral Science Foundation specific funded project (grant no.
201003380); the Natural Science Foundation of Ningbo (grant no.
2011A610057); the Natural Science Foundation of China (grant no.
81372212); the Natural Science Foundation of Jiangsu (grant no.
BK2011251); Jiangsu Provincial Special Program of Medical Science
(grant no. BL2013012); the Health Talents Project for Jiangsu
(grant nos. LJ201157; RC2011038; BRA2011038); and the Natural
Science Foundation of Ningbo (grant no. 2011A610057).
References
|
1
|
Habib E and Elhadad A: Digestive
complications of gallstones lost during laparoscopic
cholecystectomy. HPB (Oxford). 5:118–122. 2003.
|
|
2
|
Delcò F, Domenighetti G, Kauzlaric D,
Donati D and Mombelli G: Spontaneous biliothorax (thoracobilia)
following cholecystopleural fistula presenting as an acute
respiratory insufficiency. Successful removal of gallstones from
the pleural space. Chest. 106:961–963. 1994.
|
|
3
|
Dasmahapatra HK and Pepper JR:
Bronchopleurobiliary fistula. A complication of intrahepatic
biliary stent migration. Chest. 94:874–875. 1988.
|
|
4
|
Nøjgaard C, Hornum M, Elkjaer M, et al:
Does glyceryl nitrate prevent post-ERCP pancreatitis? A
prospective, randomized, double-blind, placebo-controlled
multicenter trial. Gastrointest Endosc. 69:e31–e37. 2009.
|
|
5
|
Williams EJ, Hamlyn A, Logan RF, Martin D,
Wilkinson ML and Lombard M: Consenting patients for endoscopic
retrograde cholangiopancreatography: results of a survey of 182 UK
endoscopists and 2059 of their patients. Eur J Gastroenterol
Hepatol. 21:1351–1357. 2009.
|
|
6
|
Cennamo V, Fuccio L, Repici A, et al:
Timing of precut procedure does not influence success rate and
complications of ERCP procedure: a prospective randomized
comparative study. Gastrointest Endosc. 69:473–479. 2009.
|
|
7
|
Lin CT, Hsu KF, Yu JC, et al:
Choledochoduodenal fistula caused by cholangiocarcinoma of the
distal common bile duct. Endoscopy. 41(Suppl 2): E319–E320.
2009.
|