Introduction
Prostate cancer (PCa) is the most common type of
malignancy and the second leading cause of cancer mortality in
males in Western countries (1). In
the USA in 2011, there were 240,890 new cases of PCa diagnosed and
33,720 PCa-specific mortalities. In Taiwan, PCa is the seventh most
common cause of cancer-associated mortality and the incidence is
increasing, particularly in elderly populations. Due to the
widespread implementation of prostate-specific antigen (PSA)
screening, the earlier detection of PCa has increased. Although the
incidence of PCa has rapidly increased in Taiwan (30 cases per
100,000 individuals in 2010), this is significantly lower than that
of the USA and Europe (2). When the
PCa is not metastatic, it can be treated with radiotherapy or
surgery; however, the treatment of metastatic PCa is palliative.
PCa initially grows in an androgen-dependent manner, and therefore,
androgen deprivation therapy (ADT) may improve symptoms and reduce
PSA levels in ~80% of metastatic PCa patients (3). After an average of two years
undergoing hormone therapy, the majority of metastatic PCa cases
are likely to develop into castration-resistant PCa (CRPC)
(4). Chemotherapy for CRPC was
implemented for a number of years, although it had limited
efficacy, until two landmark randomized control trials were
reported. Once complete, the two phase III trials demonstrated that
a docetaxel-based combined chemotherapy regimen may improve
survival rates in CRPC patients (3,4). In
the TAX 327 study, the median overall survival (OS) time was
improved in the docetaxel plus prednisone treatment group compared
with the mitoxantrone plus prednisone treatment group (3). In the Southwest Oncology Group (SWOG)
study, the docetaxel plus estramustine regimen showed a survival
benefit versus the mitoxantrone plus prednisone regimen (5). Therefore, in 2004, docetaxel was
approved by the European Medicine Agency and the US Food and Drug
Administration as the first-line treatment for patients with CRPC.
The aim of the present study was to retrospectively evaluate the
efficacy and toxicity of treatment with docetaxel plus prednisolone
every four weeks in patients in Taiwan with CRPC, as there are few
studies of this type concerning Asian populations.
Patients and methods
Patients
A total of 26 patients with CRPC were reviewed
retrospectively between July 2007 and October 2012 at the Kaohsiung
Medical University Hospital (Kaohsiung, Taiwan). All patients
provided written informed consent. This study was approved by the
institutional review board of Kaohsiung Medical University Chung-Ho
Memorial Hospital (Kaohsiung, Taiwan). The eligibility criteria
included histopathologically diagnosed progressive prostate
adenocarcinoma with disease progression despite ADT and no previous
chemotherapy.
Treatment
All patients received docetaxel plus prednisone
therapy with or without estramustine. The regimen consisted of
docetaxel (70 mg/m2), which was administered over 60 min
through intravenous infusion once every four weeks, plus oral
prednisolone (5 mg) twice daily for five days (days one to five).
All cases were defined as CRPC according to the European
Association of Urology guideline 2011 (6). Serum PSA levels were measured every
four weeks during treatment. When each course was initiated, a
complete blood count was performed, and renal and liver function
were assessed. The time to PSA progression, PCa-specific survival,
OS and the PSA response of all patients were evaluated. The OS rate
was measured as the time between the initial docetaxel
administration and mortality. The definition of PSA response was a
reduction of ≥50% from the baseline levels for at least four weeks.
PSA progression was defined as a >50% increase from the PSA
nadir and an increase in the absolute PSA level by ≥5 ng/ml with
confirmation following at least one week (7). The PSA nadir was defined as the lowest
PSA level achieved during treatment. The time to PSA progression
was assessed between the day of treatment initiation and PSA
progression. Treatment with docetaxel was continued until disease
progression, unacceptable adverse effects, or the refusal of the
patient to receive further therapy.
The National Cancer Institute Common Toxicity
Criteria version 4.0 was used to evaluate the toxicity during every
cycle (8). Granulocyte
colony-stimulating factor (G-CSF) was administered when grade 3 or
4 leucopenia and febrile leucopenia occurred according to
physician’s experience. The definition of leucopenia was a white
blood cell count of <4,400/μl.
Statistical analysis
All analyses were performed using SPSS software,
version 19.0 (IBM, Armonk, NY, USA). The probability of
PCa-specific survival and OS between PSA response and no response
was calculated using Kaplan-Meier analysis. Following the
univariate analysis, a multivariate analysis was performed to
elucidate the effect of these combined variables. P<0.05 was
considered to indicate a statistically significant difference.
Results
Patient characteristics
The characteristics of 26 patients with CRPC are
summarized in Table I. In the
present study, prior to the introduction of docetaxel-based
chemotherapy, the mean serum PSA level was 335.58±501.87 ng/ml
(normal range, <20 ng/ml) and the mean serum hemoglobin (Hb)
level was 10.70±1.69 g/dl (normal range, 14–17 g/dl). During the
period of chemotherapy, a mean number of cycles (6.92±3.03) were
administrated and four patients received >10 cycles.
 | Table ICharacteristics of the 26 CRPC
patients. |
Table I
Characteristics of the 26 CRPC
patients.
| Characteristic | Value |
|---|
| Age, years | |
| Mean ± SD | 73.19±9.93 |
| Range | 54.00–88.00 |
| Cycles, n | |
| Median ± SD | 6.92±3.03 |
| Range | 2.00–14.00 |
| Serum PSA, ng/ml | |
| Mean ± SD | 335.58±501.87 |
| Range | 14.67–2363.56 |
| Hemoglobin, g/dl | |
| Mean ± SD | 10.70±1.69 |
| Range | 7.50–13.70 |
| Concomitant
estramustine, n (%) | 12 (46) |
| Site of metastasis, n
(%) | |
| Bone | 25 (96) |
| Lymph node | 8 (31) |
| Liver | 1 (4) |
| PSA response, n
(%) | 15 (58) |
| No PSA decrease, n
(%) | 3 (12) |
| PSA nadir, ng/ml | |
| Mean ± SD | 89.97±117.76 |
| Range | 0.84–448.59 |
| Time to PSA nadir,
months | |
| Mean ± SD | 4.65±3.60 |
| Range | 0.50–13.00 |
| Time to progression,
months | |
| Mean ± SD | 6.50±5.85 |
| Range | 0.00–23.00 |
| Survival time
following chemotherapy, months | |
| Mean ± SD | 14.69±10.14 |
| Range | 3–43 |
| Mortality, n (%) | 20 (77) |
| Side-effect, n
(%) | |
| Leucopenia | 23 (88) |
| Febrile
leucopenia | 4 (15) |
PSA response
A PSA decrease of >50% from the baseline was
observed in 15 (58%) of the 26 patients. During the treatment, the
mean PSA nadir level was 89.97±117.76 ng/ml and the time to PSA
nadir and progression was 4.65±3.60 and 6.50±5.85 months,
respectively. No significant differences were identified between
certain variables, including age, Hb level, PSA level, PSA nadir,
PSA decline and the number of cycles of estramustine, in the PSA
response and non-PSA response groups in Table II. However, the results indicated
that the occurrence of leucopenia may be associated with a higher
PSA response rate (P=0.032). In addition, the length of the time to
PSA nadir was shown to significantly affect PSA response. For the
variation in PSA kinetics, the PSA decline was calculated using an
algorithm according to the following formula: PSA decline = Log
[(PSA level prior to chemotherapy - PSA nadir)/survival time
(months)]. The results of univariate and multivariate Cox
regression analyses for the OS rate of 26 patients are summarized
in Table III. The univariate and
multivariate analyses revealed that the number of chemotherapy
cycles and time to PSA nadir were independent prognostic factors of
the OS rate (P<0.05).
| Table IIAssociated factors between PSA
response and PSA no response. |
Table II
Associated factors between PSA
response and PSA no response.
| Factor | PSA response
(n=15) | PSA no response
(n=11) | P-value |
|---|
| Age, years | 72.33±9.68 | 74.36±10.61 | 0.616 |
| Hemoglobin, g/dl | 10.54±1.57 | 10.93±1.89 | 0.574 |
| PSA level, ng/ml | 424.38±625.90 | 214.48±230.83 | 0.301 |
| PSA nadir, ng/ml | 63.93±87.27 | 138.8±155.47 | 0.151 |
| Time to PSA nadir,
months | 5.77±3.77 | 2.56±2.13 | 0.039 |
| PSA declinea | 0.17±0.11 | 0.19±0.13 | 0.787 |
| Cycles, n | 7.80±3.51 | 5.73±1.74 | 0.061 |
| Leukopenia, n
(%) | | | 0.032 |
| Yes | 15 (65.20) | 8 (34.80) | |
| No | 0 (0.00) | 3 (100.00) | |
| Estramustine, n
(%) | | | 0.391 |
| Yes | 8 (66.70) | 4 (33.30) | |
| No | 7 (50.00) | 7 (50.00) | |
| Table IIIAssociated baseline factors of overall
survival by univariate and multivariate analysis. |
Table III
Associated baseline factors of overall
survival by univariate and multivariate analysis.
| Univariate | Multivariate |
|---|
|
|
|
|---|
| Baseline
characteristic | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years | 0.994 | (0.95–1.04) | 0.781 | 1.017 | (0.96–1.08) | 0.577 |
| Cycles, n | 0.741 | (0.60–0.92) | 0.006 | 0.704 | (0.53–0.93) | 0.015 |
| Hemoglobin, g/dl | 0.985 | (0.75–1.30) | 0.912 | 1.086 | (0.75–1.57) | 0.662 |
| PSA, ng/ml | 1.000 | (1.00–1.00) | 0.872 | 1.000 | (1.00–1.00) | 0.936 |
| PSA nadir, ng/ml | 1.002 | (1.00–1.01) | 0.243 | 1.002 | (1.00–1.01) | 0.402 |
| Time to PSA nadir,
months | 0.736 | (0.59–0.91) | 0.005 | 0.677 | (0.49–0.94) | 0.019 |
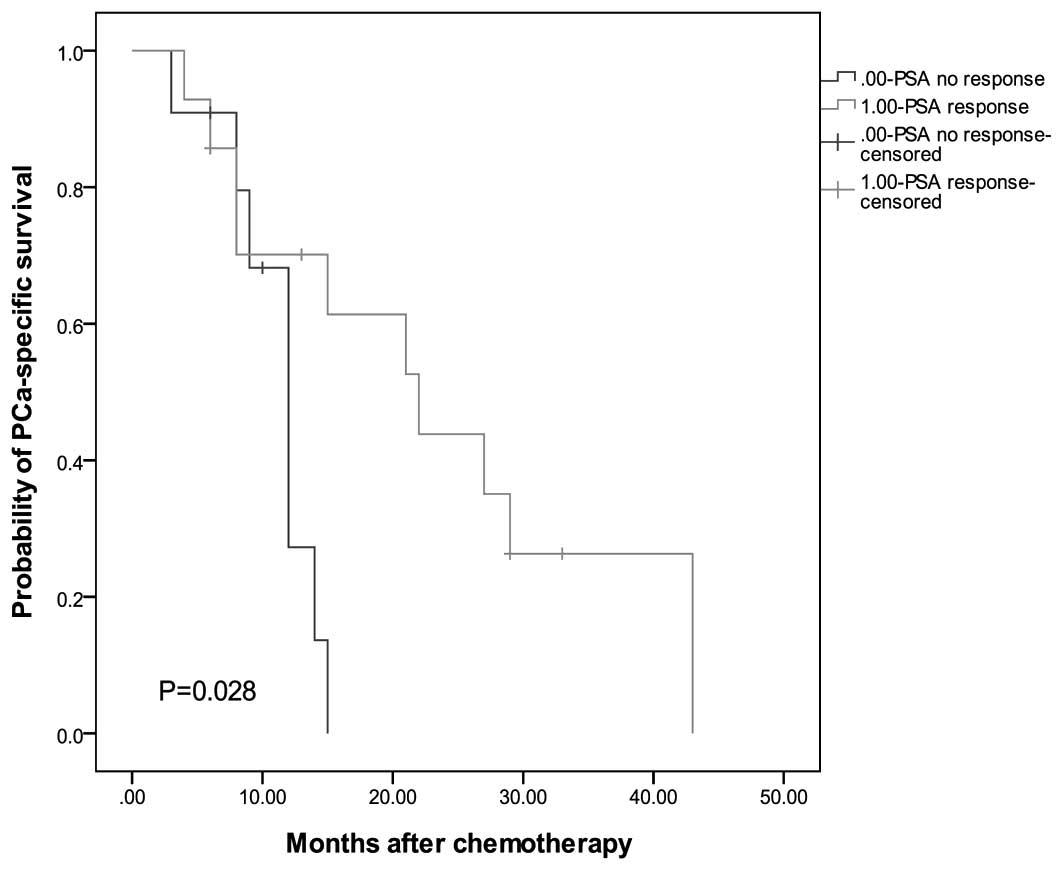
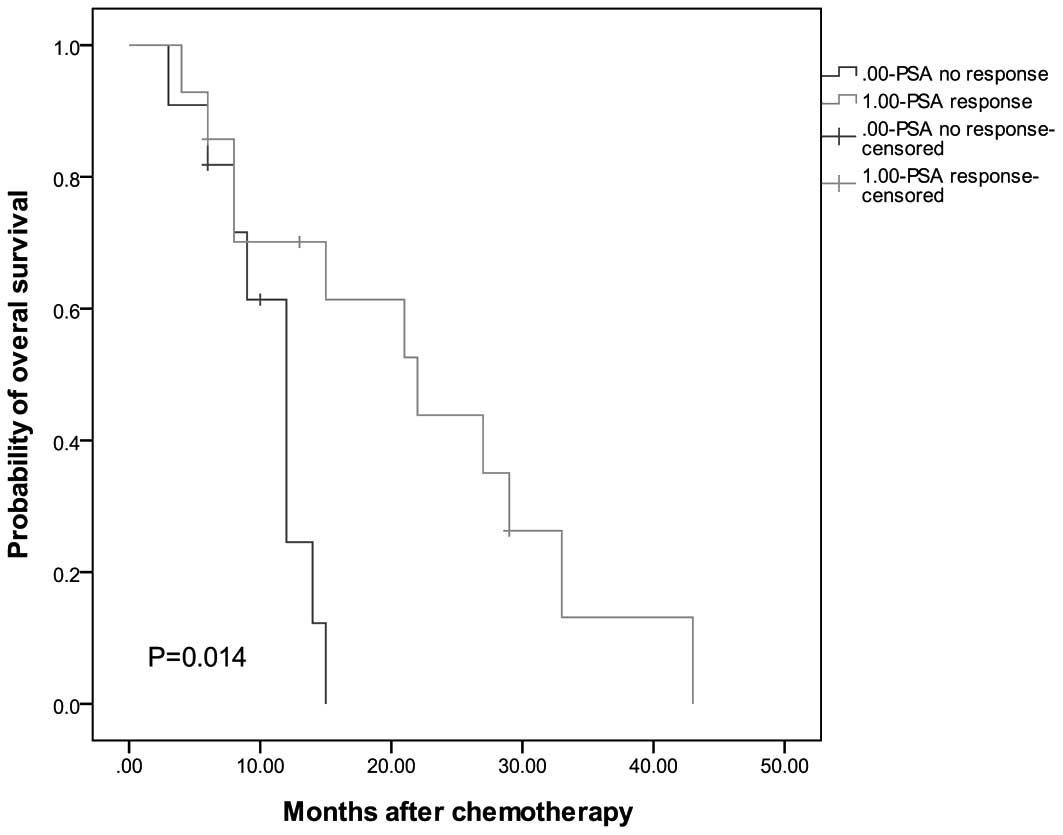
Kaplan-Meier analysis
As shown in Figs. 1
and 2, in order to identify the
possible prognostic factors of docetaxel-based chemotherapy, the
correlation between certain factors and survival rates was
analyzed. The results indicated that PSA response is a significant
predictor of OS (P=0.014) and PCa-specific survival (P=0.028).
Discussion
According to two large, randomized trials (3,5),
docetaxel-based chemotherapy is currently the standard chemotherapy
for CRPC due to its survival benefit. The present study
retrospectively assessed the oncologic outcomes of 26 patients with
CRPC to identify prognostic factors. At the Kaohsiung Medical
University Hospital, a docetaxel-based chemotherapy regimen,
consisting of 70 mg/m2 docetaxel once every four weeks
and 5 mg prednisolone twice daily on days one to five for each
cycle, was administered, which is a different protocol compared
with that of previous studies (3,5,7).
Clinically, it is common to add steroids to docetaxel-based
chemotherapy in CRPC. The mechanism of the combination of docetaxel
and prednisolone may increase the cytotoxic efficacy and
antiangiogenic activity of docetaxel by steroids (9).
In the present study, the PSA response was 58%,
which was similar or superior to the results observed in previous
studies. For example, Hideaki et al (10) reported a PSA response rate of 55.6%.
In addition, Naito et al (11) and Lee et al (12) reported PSA response rates of 44.4%
and 51%, respectively. The median OS time of the current patients
following chemotherapy was 14.84 months, which was shorter than
that observed in the two landmark studies (19.2 months in the
TAX327 study and 17.5 months in the SWOG 99-16 study). However, the
mean PSA levels prior to chemotherapy in these two studies (114
ng/ml in the TAX327 study and 84 ng/ml in the SWOG 99-16) were
lower than those identified in the current study. The results
indicated that the survival time is associated with pretreatment
PSA levels. Although, different patient characteristics and the
small sample size may also be influencing factors. Further
comparisons are required between the various therapy periods to
assess whether a duration of four weeks is more effective than that
of three weeks.
Furthermore, the results demonstrated that PSA
response is an important predictor factor of OS and PCa-specific
survival rates. However, it is important to be aware of the PSA
flare-up phenomenon, which leads to a transient PSA elevation
following chemotherapy (13). In
the current study, two patients exhibited an increase in their PSA
levels on initiation of treatment, which was followed by a decline
in PSA levels after five weeks (Table
IV). This may occur between one and eight weeks following a
drop in the level of serum PSA (14). There is no firm hypothesis for the
mechanism of post-chemotherapy PSA surge syndrome. However, one
theory proposes that PSA is released on the destruction of cancer
cells or the increase may be due to local inflammation (15,16).
Therefore, chemotherapy may be continued for at least three cycles
to avoid inadequate therapy, provided no severe side effects
develop.
| Table IVPSA kinetics in patients with
flare-up phenomenon. |
Table IV
PSA kinetics in patients with
flare-up phenomenon.
| Patient | PSA at baseline,
ng/ml | PSA at peak,
ng/ml | Time to decline,
weeks | Nadir, ng/ml |
|---|
| 1 | 74.38 | 80.39 | 5 | 56.41 |
| 2 | 319.39 | 342.03 | 5 | 97.97 |
Although 10 cycles of docetaxel are generally used
as the standard treatment and a recent study has concluded that
>10 cycles of docetaxel-based chemotherapy for CRPC does not
improve overall survival, in the present study, treatment was
continued for >10 cycles (17).
The number of cycles administered was based on the patient’s
medical condition and disease progression. Of the 26 patients, four
received >10 cycles of treatment and these four patients all
exhibited a PSA response and had survival times of more than two
years.
The most common adverse effect was leucopenia and
this affected 88% of patients in the present study. Of these
patients, four cases of febrile leucopenia were identified, and
antibiotics were administered in these instances. The incidence of
leucopenia was higher than that observed in Western populations
(7). There has been an assumption
that the polymorphisms of CYP3A isoenzymes cause the difference
between ethnic backgrounds (7). In
the current study, the white blood cell count was measured prior to
and following chemotherapy in the patients that exhibited an
associated infection. If patients had fever or grade 3 or 4
neutropenia, the administration of G-CSF was proposed. Among these
cases, interstitial pneumonitis was observed in one patient, who
presented with a fever, a cough with sputum, dyspnea and diffuse
lung infiltrates. Although chemotherapy were discontinued, the
patient succumbed as a result of respiratory failure. Previous
studies have demonstrated that the incidence of interstitial
pneumonitis is ~0.2% and it is considered that this may result from
docetaxel administration (7,16). In
the majority of cases, patients recover following the
discontinuation of docetaxel-based chemotherapy; however, it can be
lethal, as observed in the current study. In cases of severe
interstitial pneumonitis, lung function is examined prior to
commencing chemotherapy, particularly on elderly patients or those
with a history of lung disease. In addition, luteinizing
hormone-releasing hormone agonists and non-steroidal anti-androgens
may also cause interstitial pneumonitis; the latency of which may
persist for up to eight months (18). Prior to the onset of CRPC, all
patients in the present study received hormone therapy, thus,
clinicians must aim to prevent vulnerable patients from developing
interstitial pneumonitis. The results of the current study
indicated that the onset of leucopenia may be associated with PSA
response. The assumption is that the more susceptible the PCa is to
treatment with docetaxel, the more susceptible the patient is to
adverse effects.
In total, 12 of the 26 patients received concomitant
estramustine therapy, which appeared to provide no survival
benefit, however, the small sample size may not be representative.
It has been proposed that the addition of estramustine is likely to
increase the risk of cardiovascular events, including thrombosis
and myocardial infarction. Although no associated lethal adverse
effects were observed during this study, this possibility cannot be
ignored, and prophylactic anticoagulant agents may therefore be
prescribed to patients who have a history of, or who are at risk
of, cardiovascular toxicity (19).
However, Qi et al (20)
concluded that the survival rates with regard to PSA response rate
were not improved with the addition of estramustine to
docetaxel-based chemotherapy (4).
Therefore, the toxicity profile must be considered prior to the
addition of estramustine to the therapeutic regimen.
Multivariate analysis of the prognostic factors
revealed a significant correlation between OS rates, and the number
of chemotherapy cycles and time to PSA nadir. The results revealed
that an increased number of treatment cycles and longer time to PSA
nadir correlate with a longer OS. Therefore, time to PSA nadir may
represent an adaptive ability. However, the mechanism of
association requires confirmation; a significant heterogeneity in
CRPC may lead to this result (21).
Previous studies have evaluated prognostic factors as a method of
predicting survival outcomes for CRPC patients prior to
chemotherapy. The retrospective analysis presented by Qu et
al (22) showed that the
measurement of PSA doubling time, baseline Hb concentration,
baseline alkaline phosphatase concentration, number of chemotherapy
cycles and time to castration resistance, may provide predictive
information. However, due to the retrospective nature and small
sample size of the current study, future prospective studies with
larger populations of patients are required.
In conclusion, docetaxel and prednisolone
combination chemotherapy was an effective treatment regimen in
Taiwanese CRPC patients, with high rates of PSA response and
improved survival rates. The most common side effect was
leucopenia, which can be controlled by administration of G-CSF.
However, a careful assessment prior to therapy is required for the
prevention of lethal adverse effects, including interstitial
pneumonitis and cardiovascular events. This retrospective study
demonstrated that PSA response, number of chemotherapy cycles and
time to PSA nadir may provide prognostic factors for OS. However,
further prospective studies investigating a larger population are
required to evaluate more prognostic factors within Asian
populations.
Acknowledgements
This study was supported by a grant from the
Ministry of Health and Welfare (grant no. MOHW103-TD-B-111-05).
References
|
1
|
Matsuda T, Marugame T, Kamo K, et al:
Cancer incidence and incidence rates in Japan in 2005: based on
data from 12 population-based cancer registries in the Monitoring
of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol.
41:139–147. 2011.
|
|
2
|
Chen CH, Yao HH, Huang SW, et al: Using
age-referenced prostate-specific antigen percentile to predict
survival outcomes in screened Taiwanese men. Int J Cancer.
132:1927–1932. 2013.
|
|
3
|
Tannock IF, de Wit R, Berry WR, et al; TAX
327 Investigators. Docetaxel plus prednisone or mitoxantrone plus
prednisone for advanced prostate cancer. N Engl J Med.
351:1502–1512. 2004.
|
|
4
|
Kuramoto T, Inagaki T, Fujii R, et al:
Docetaxel in combination with estramustine and prednisolone for
castration-resistant prostate cancer. Int J Clin Oncol. 18:890–897.
2013.
|
|
5
|
Petrylak DP, Tangen CM, Hussain MH, et al:
Docetaxel and estramustine compared with mitoxantrone and
prednisone for advanced refractory prostate cancer. N Engl J Med.
351:1513–1520. 2004.
|
|
6
|
Mottet N, Bellmunt J, Bolla M, et al: EAU
guidelines on prostate cancer. Part II: Treatment of advanced,
relapsing, and castration-resistant prostate cancer. Eur Urol.
59:572–583. 2011.
|
|
7
|
Miura N, Numata K, Kusuhara Y, et al:
Docetaxel-prednisolone combination therapy for Japanese patients
with hormone-refractory prostate cancer: a single institution
experience. Jpn J Clin Oncol. 40:1092–1098. 2010.
|
|
8
|
National Cancer Institute. National Cancer
Institute common terminology criteria for adverse events version
4.0. http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf.
Accessed April 20, 2013
|
|
9
|
Wilson C, Scullin P, Worthington J, et al:
Dexamethasone potentiates the antiangiogenic activity of docetaxel
in castration-resistant prostate cancer. Br J Cancer. 99:2054–2064.
2008.
|
|
10
|
Miyake H, Sakai I, Terakawa T, Harada K
and Fujisawa M: Oncological outcome of docetaxel-based chemotherapy
for Japanese men with metastatic castration-resistant prostate
cancer. Urol Oncol. 31:733–738. 2013.
|
|
11
|
Naito S, Tsukamoto T, Koga H, et al:
Docetaxel plus prednisolone for the treatment of metastatic
hormone-refractory prostate cancer: a multicenter Phase II trial in
Japan. Jpn J Clin Oncol. 38:365–372. 2008.
|
|
12
|
Lee JL, Kim JE, Ahn JH, et al: Efficacy
and safety of docetaxel plus prednisolone chemotherapy for
metastatic hormone-refractory prostate adenocarcinoma: single
institutional study in Korea. Cancer Res Treat. 42:12–17. 2010.
|
|
13
|
Nelius T, Klatte T, de Riese W and Filleur
S: Impact of PSA flare-up in patients with hormone-refractory
prostate cancer undergoing chemotherapy. Int Urol Nephrol.
40:97–104. 2008.
|
|
14
|
Thuret R, Massard C, Gross-Goupil M, et
al: The postchemotherapy PSA surge syndrome. Ann Oncol.
19:1308–1311. 2008.
|
|
15
|
Olbert PJ, Hegele A, Kraeuter P, et al:
Clinical significance of a prostate-specific antigen flare
phenomenon in patients with hormone-refractory prostate cancer
receiving docetaxel. Anticancer Drugs. 17:993–996. 2006.
|
|
16
|
Ide H, Kikuchi E, Kono H, et al: Docetaxel
in combination with prednisolone for hormone refractory prostate
cancer. Jpn J Clin Oncol. 40:79–84. 2010.
|
|
17
|
Pond GR, Armstrong AJ, Wood BA, et al:
Evaluating the value of number of cycles of docetaxel and
prednisone in men with metastatic castration-resistant prostate
cancer. Eur Urol. 61:363–369. 2012.
|
|
18
|
Masago T, Watanabe T, Nemoto R and Motoda
K: Interstitial pneumonitis induced by bicalutamide given for
prostate cancer. Int J Clin Oncol. 16:763–765. 2011.
|
|
19
|
Matsumoto A, Inoue A, Yokoi S, et al:
Evaluation of docetaxel plus estramustine in the treatment of
patients with hormone-refractory prostate cancer. Int J Urol.
16:687–691. 2009.
|
|
20
|
Qi WX, Shen Z and Yao Y: Docetaxel-based
therapy with or without estramustine as first-line chemotherapy for
castration-resistant prostate cancer: a meta-analysis of four
randomized controlled trials. J Cancer Res Clin Oncol.
137:1785–1790. 2011.
|
|
21
|
Huang SP, Bao BY, Wu MT, et al: Impact of
prostate-specific antigen (PSA) nadir and time to PSA nadir on
disease progression in prostate cancer treated with
androgen-deprivation therapy. Prostate. 71:1189–1197. 2011.
|
|
22
|
Qu YY, Dai B, Kong YY, Ye DW, Yao XD,
Zhang SL, et al: Prognostic factors in Chinese patients with
metastatic castration-resistant prostate cancer treated with
docetaxel-based chemotherapy. Asian J Androl. 15:110–115. 2013.
|