Introduction
Primary sternal tumors are a rare type of bone and
soft tissue tumor, with chondrosarcoma being the most common.
Generally, the precise evaluation of such tumors requires a
thorough radiological examination since the clinically appreciable
mass usually involves the sternum (1). However, sternal chondrosarcomas are
resistant to chemotherapy and radiation and thus, wide resection is
the only curative option (2).
Sternal tumors have been considered a significant challenge in
surgery due to the difficulties in full-thickness resectioning
without compromising the stability and reconstruction of the
thoracic wall (1). Due to
improvements in surgical technique, it is now possible to perform
total sternectomies (1). Adequate
surgical excision and reconstruction may offer a definitive cure;
however, the surgical procedure may be difficult to perform due to
the local aggressiveness of these tumors and their high recurrence
rate and thus, reconstruction remains controversial (3). In addition, chest wall stability
following wide sternectomy may be achieved by using various
prosthetic materials, such as Marlex mesh or
polytetrafluoroethylene patches (4). The aims of the current study were to
report a rare case of chondrosarcoma of the manubrium sterni, which
was successfully treated via radical resection and reconstruction
with titanium mesh and steel wire and to evaluate the use of such
techniques. Written informed consent was obtained from the
patient.
Case report
In July 2013, a 37-year-old previously healthy
female, who had previously undergone one cesarean delivery,
presented at The First Affiliated Hospital of Wenzhou Medical
University (Wenzhou, China) with a lump and pain of the anterior
chest wall. On physical examination, a palpable mass was identified
on the manubrium sterni, which was not tender on palpation.
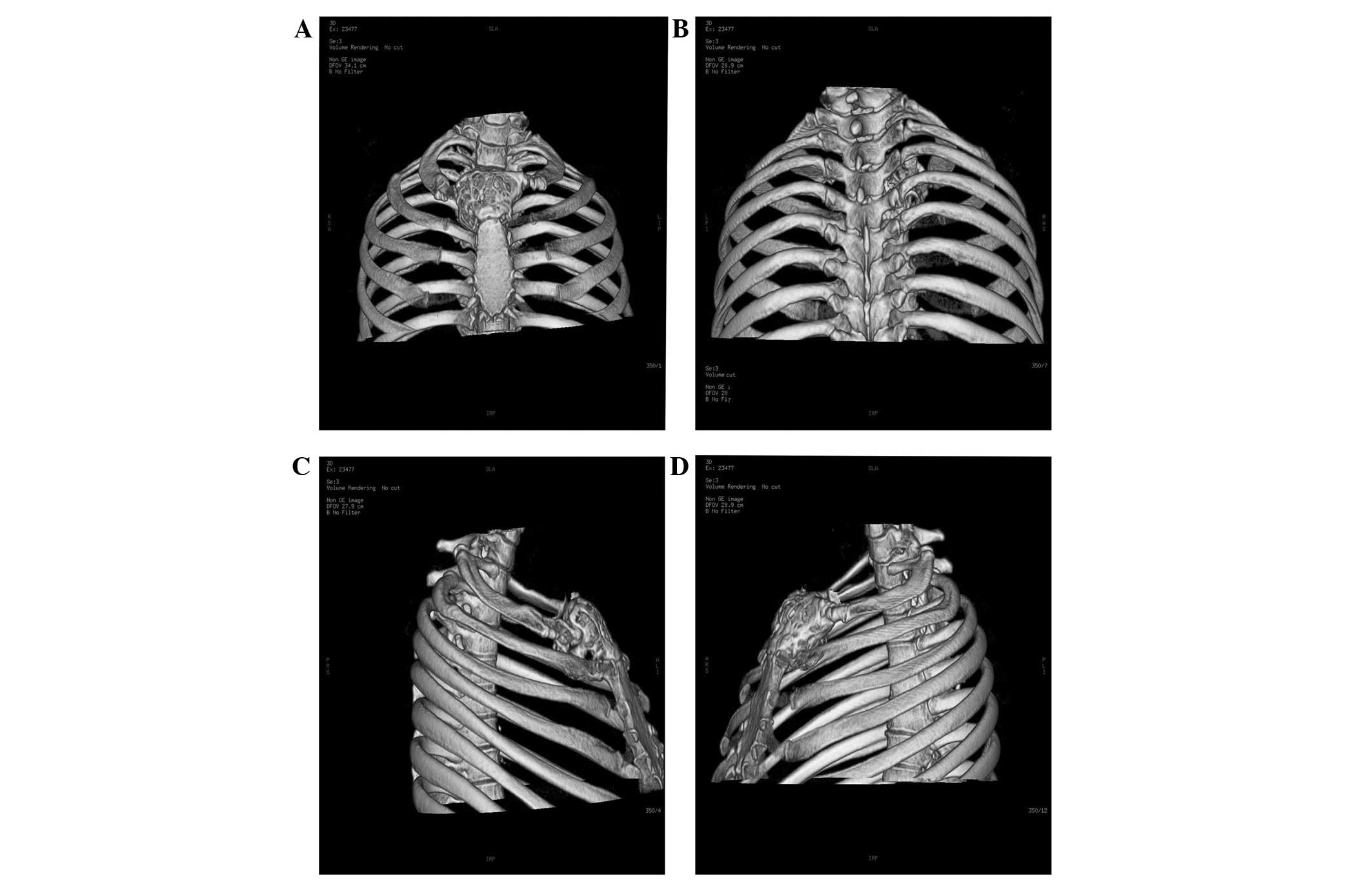
Laboratory tests revealed no abnormalities; however, a chest
computed tomography (CT) scan reconstruction demonstrated an
expansive localized, hypodense, round mass on the manubrium sterni
(diameter, ~5.1×4.2 cm; Fig. 1).
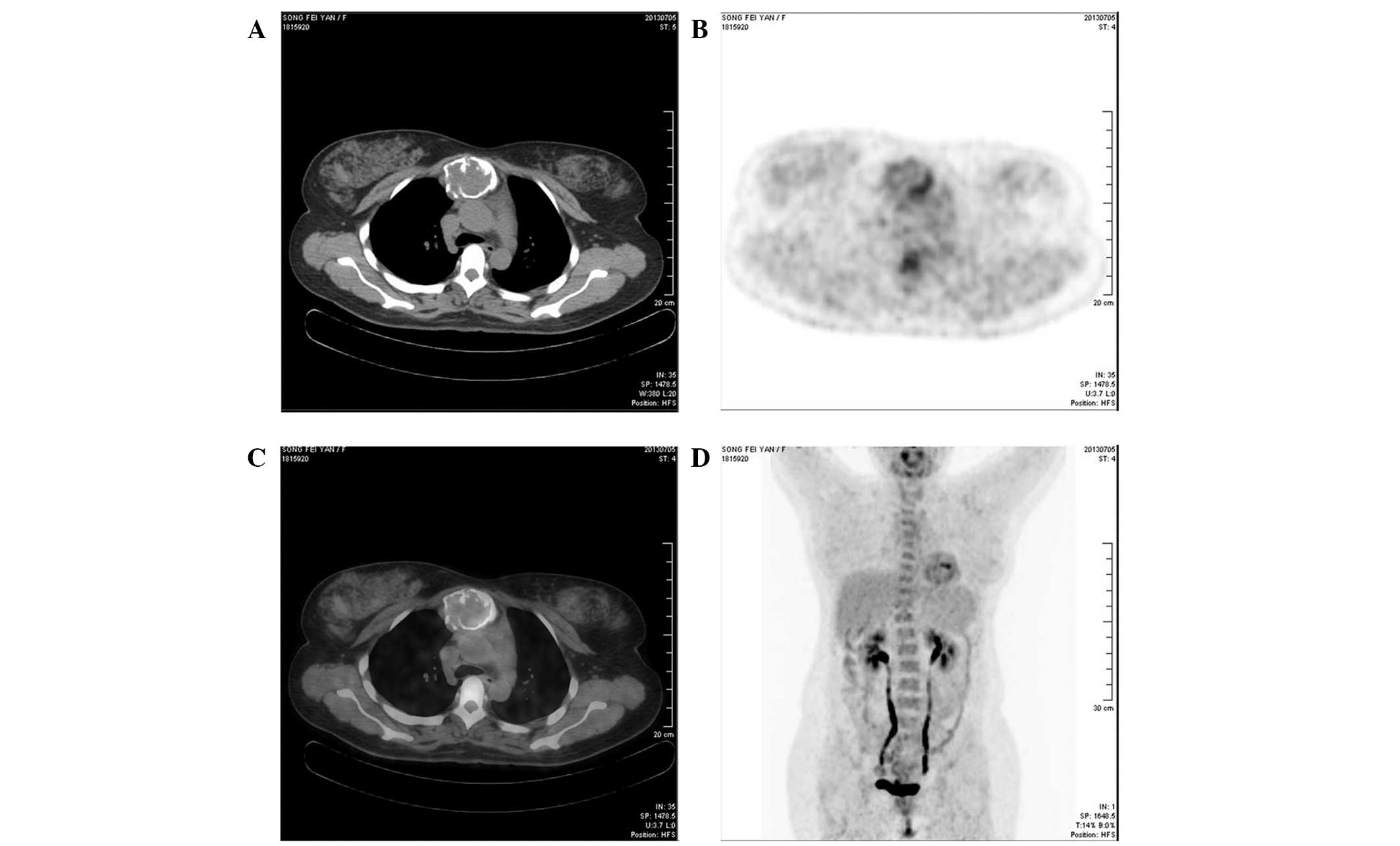
The CT indicated that the mass may be a giant cell tumor. Positron
emission tomography (PET)-CT revealed an expanding mass with an
irregular shape, arising from the manubrium sterni, with a maximum
diameter of 6 cm and a maximum standardized uptake value of 3.7
(Fig. 2). The mass was marginally
18F-fluorodeoxyglucose (FDG)-avid, however, there was no
evidence that the distant metastases were FDG-avid. On the basis of
the anatomic and metabolic findings, the PET-CT interpretation
strongly indicated a type of well-differentiated malignant tumor,
such as a giant cell tumor.
With a clear resection margin, a radical resection
and reconstruction using steel wire and titanium mesh (M3
system/model; OsteoMed Co., Addison, TX, USA) was performed.
Radical resection of the right and left sternoclavicular joints,
the second rib and the entire upper section of the sternum body was
performed, and a drainage tube was placed in the mediastinum.
Following surgery, the patient received antibiotics and expectorant
treatment, along with parenteral nutrition. The pain subsequently
diminished and became tolerable. On postoperative day five, the
removal of the mediastinal drainage tube was required; the patient
recovered well following surgery and was discharged on
postoperative day eight. The overall duration of the hospital stay
was 16 days. Follow-up CT scans were performed every three months
to monitor tumor recurrence. After 12 months of follow-up no tumor
reccurence was identified.
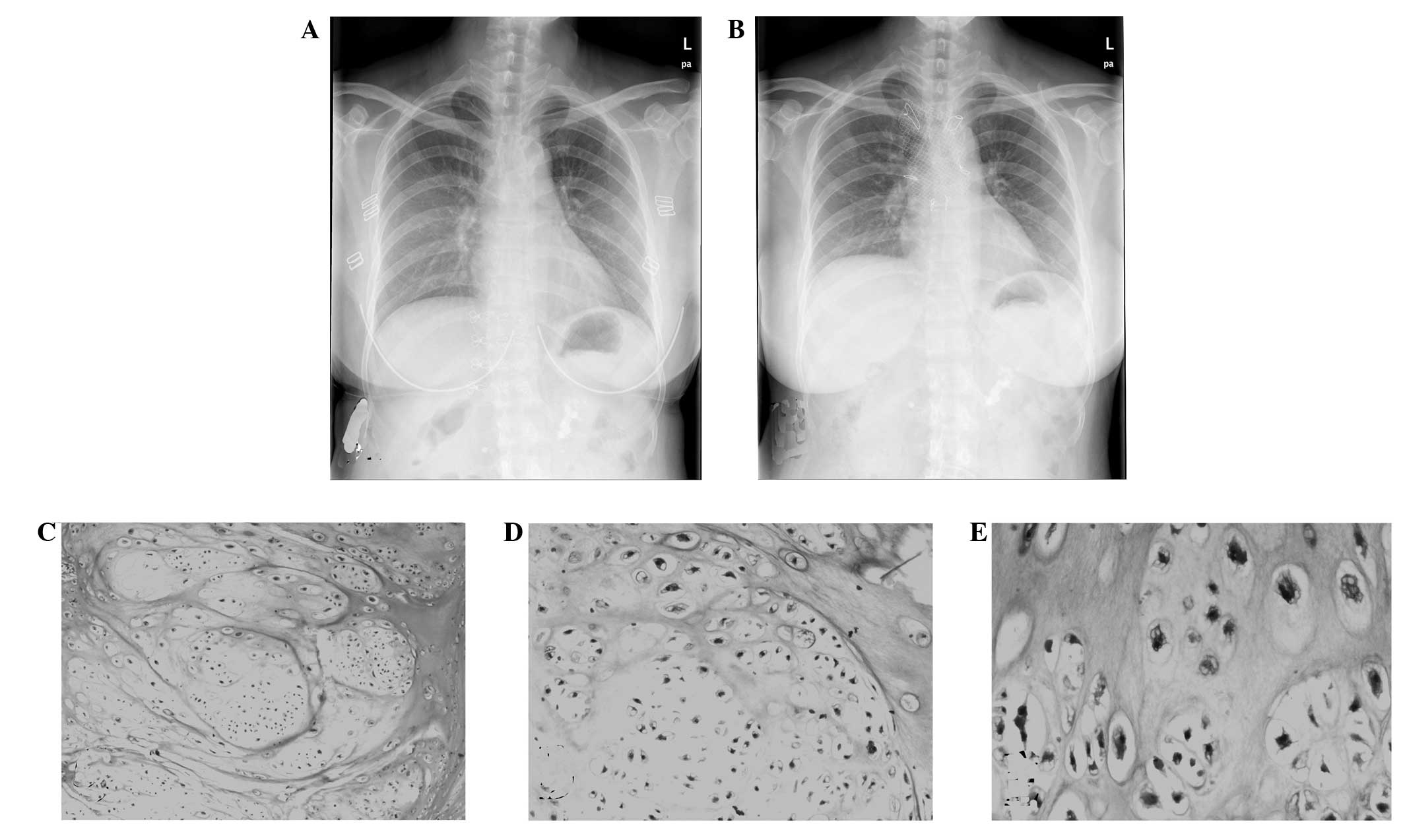
Histological analysis of a surgical specimen
revealed well-differentiated malignant cartilaginous cells,
consistent with a grade I (considered to be low grade)
chondrosarcoma (Fig. 3). The tumor
cells were located within the medullary bone, resulting in bone
expansion and destruction of the bone cortex. The chondrosarcoma
was predominantly composed of hyaline cartilage cells and exhibited
a chondromyxoid cartilage matrix, as well as atypical cells,
including binucleated cells.
Discussion
Primary sternal tumors are uncommon and account for
only ~1% of primary bone neoplasms, worldwide (1,5).
Chondrosarcoma, a type of malignant cartilage-forming tumor, is
considered to be the most common primary malignancy of the anterior
thoracic wall. However, chondrosarcomas remain a rare type of
lesion in the sternum and the majority of neoplasms are secondary
sternal tumors, which arise from metastases originating in areas,
such as the thyroid, breasts and lungs (6,7).
In cases of chondrosarcoma, the CT scan usually
indicates a hypodense, rounded mass that is located in the sternum;
the bone is expansive and the cortex is thin and damaged. PET-CT
may occasionally distinguish benign from malignant bone neoplasms,
however, certain well-differentiated tumors may be only marginally
FDG-avid on PET-CT imaging, therefore, it can be challenging to
differentiate the tumor types. Although the histopathological
findings of the excised mass are the only true determinant of the
nature of the cancer, PET-CT remains a valuable and meaningful
measure for assessing the nature and extent of the tumor.
Histopathologically, chondrosarcoma exhibit a
distinctive architecture, with high numbers of hyaline cartilage
cells and the presence of a chondromyxoid cartilage matrix. The
atypical cells are comprised of oval or round nuclei and a deeply
eosinophilic cytoplasm (8).
Bone autografts and allografts from the ribs or
iliac bone have been reported as an alternative to synthetic
materials for use when rebuilding chest wall defects (9). However, omental flaps and titanium
plates offer increased stability and safety for reconstruction
following extensive sternocostal resection (10). Due to its biocompatibility and
flexibility, titanium mesh may also be an effective material for
reconstructing defects without limitations (5). It has been associated with minimal
trauma, fewer infections and reduced postoperative pain.
Furthermore, following surgery, patients recover well, which
results in a short hospital stay.
In conclusion, the current study reports a rare case
of primary chondrosarcoma of the sternum, which was successfully
treated by radical resection and reconstruction using steel wire
and titanium mesh. Therefore, in future cases, the use of titanium
mesh and steel wire may be considered as highly beneficial
materials for use during the reconstruction of defects of the
sternum.
References
|
1
|
Lequaglie C, Massone PB, Giudice G and
Conti B: Gold standard for sternectomies and plastic
reconstructions after resections for primary or secondary sternal
neoplasms. Ann Surg Oncol. 9:472–479. 2002.
|
|
2
|
Kużdżał J, Warmus J, Grochowski Z and
Gądek A: Reconstruction of the sternal manubrium. J Thorac
Cardiovasc Surg. 147:1986–1988. 2014.
|
|
3
|
Chapelier AR, Missana MC, Couturaud B, et
al: Sternal resection and reconstruction for primary malignant
tumors. Ann Thorac Surg. 77:1001–1006; discussion 1006–1007.
2004.
|
|
4
|
McCormack P, Bains MS, Beattie EJ Jr and
Martini N: New trends in skeletal reconstruction after resection of
chest wall tumors. Ann Thorac Surg. 31:45–52. 1981.
|
|
5
|
Liu ZC and Zhao H: Titanium internal
fixation system used for sternum reconstruction after resection of
chondrosarcoma. Chin Med J (Engl). 123:2621–2622. 2010.
|
|
6
|
Alpert JB, Nonaka D, Chachoua A, Pass HI
and Ko JP: Increasing dyspnea due to an anterior mediastinal mass.
Chest. 139:217–223. 2011.
|
|
7
|
Stanić V, Vulović T, Novaković M, et al:
Radical resection of giant chondrosarcoma of the anterior chest
wall. Vojnosanit Pregl. 65:64–68. 2008.
|
|
8
|
Waisberg DR, Abrão FC, Fernandez A, Terra
RM, Pêgo-Fernandes PM and Jatene FB: Surgically-challenging
chondrosarcomas of the chest wall: five-year follow-up at a single
institution. Clinics (Sao Paulo). 66:501–503. 2011.
|
|
9
|
Marulli G, Hamad AM, Cogliati E, Breda C,
Zuin A and Rea F: Allograft sternochondral replacement after
resection of large sternal chondrosarcoma. J Thorac Cardiovasc
Surg. 139:e69–e70. 2010.
|
|
10
|
Rocco G, Fazioli F, La Manna C, et al:
Omental flap and titanium plates provide structural stability and
protection of the mediastinum after extensive sternocostal
resection. Ann Thorac Surg. 90:e14–e16. 2010.
|