Introduction
During development, the fetal bladder is connected
to the allantois via the three-layer canal known as the urachus. In
the fifth month of development, the bladder descends causing the
urachus to become stretched and a loss of the lumen (1). Subsequently, the urachus forms the
median umbilical ligament. A number of abnormalities of varying
significance may arise if this process is interrupted, including
urachal carcinoma, which is a lethal disease that remains dormant
until adulthood (2). However,
urachal malignancies are rare and account for 0.5–2% of all bladder
malignancies worldwide (3).
Consequently, the majority of the current knowledge surrounding the
disease originates from case reports and a few series performed at
selected medical centers (4,5).
Prognostic is often poor due to the advanced stage of the disease
at diagnosis.
The current study reviewed all the cases of urachal
carcinoma that were diagnosed and treated at the Peking University
Shenzhen Hospital (Shenzhen, China) and Peking University First
Hospital (Beijing, China) between 1998 and 2013, and describes the
experience of dealing with this rare neoplasm.
Patients and methods
Following obtaining approval from the Institutional
Review Board of Peking University Shenzhen Hospital, the records of
17 adult patients with urachal carcinoma investigated at Peking
University Shenzhen Hospital and Peking University First Hospital
between 1998 and 2013 were retrospectively evaluated. All available
clinical, laboratory, radiographic, treatment and pathological
results for each patient were reviewed. The TNM (American Joint
Commission on Cancer) staging system (6) was used to determine prognosis due to
its consistency and universal application. Kaplan-Meier survival
curves were calculated to analyze the survival data. Written
informed consent was obatined from all patients.
Results
Patient presentation
A review of the medical records of the 17 cases of
urachal cancer demonstrated that the median age of presentation was
50 years (range, 36–77 years). Males represented the majority of
cases, with a male to female ratio of 1.42:1. Hematuria was the
most common symptom that prompted the patient to seek medical
attention, and was the predominant finding on presentation (82.3%).
In two cases, the patient presented with a palpable mass in the
lower abdomen, and one with dysuria (Table I).
 | Table IClinical features of the patients at
diagnosis. |
Table I
Clinical features of the patients at
diagnosis.
| Variables | n |
|---|
| n | 17 |
| Gender |
| Male | 10 |
| Female | 7 |
| Age, years |
| <50 | 8 |
| ≥50 | 9 |
| Primary symptoms and
signs |
| Hematuria | 14 |
| Dysuria | 1 |
| Palpable mass | 2 |
Imaging findings
All 17 patients underwent ultrasound (US) and the
most common finding was a mass observed at the dome or frontier
wall of the bladder (94.1%). In addition, almost half of the masses
(47.1%) were found to be hypoechoic (Table II). Positive urine cytology results
were observed for one of the five patients tested (20%). Computed
tomography (CT) scans were performed in 15 patients and, among
these patients, the majority of the masses (93.3%) were identified
to be solid, with only one case (6.7%) presenting with a cystic
mass. Calcification was observed in seven of the 15 cases (46.6%)
and two of the 15 cases (13.3%) exhibited lymph node metastasis.
Thickening of the bladder dome and necrosis were also observed in
one of the 15 patients (6.7%). Cystoscopy was another prevalent
diagnostic test; this procedure was conducted in 16/17 patients
(94.1%). All mass lesions could be visualized using this technique,
with the exception of one case (6.3%). Chest X-ray also revealed
metastasis involving the lungs in one out of 17 patients (5.9%).
The median tumor diameter of all 17 patients was 4.0 cm (range, 1.8
– 7.2 cm).
| Table IIImaging findings. |
Table II
Imaging findings.
| Variables | n |
|---|
| Ultrasound | 17 |
| Hypoechoic mass | 8 |
| Hyperechoic
mass | 4 |
| Heterogeneous
mass | 5 |
| Urine cytology | 5 |
| Negative | 4 |
| Positive | 1 |
| Computed
tomography | 15 |
| Solid mass | 14 |
| Cystic mass | 1 |
| Thickened bladder
dome | 1 |
| Necrosis | 1 |
| Calcification | 7 |
| Lymph nodes
metastasis | 2 |
| Cystoscopy | 16 |
| Mass lesion
visualized | 15 |
| Normal
examination | 1 |
| Tumor diameter,
cm | 17 |
| ≥4 | 8 |
| <4 | 9 |
Treatment
With the exception of one patient with confirmed
metastasis who received conservation treatment, 16 patients
underwent surgical excision. Extended partial cystectomy with en
bloc resection of the entire urachus, including the umbilicus and
the posterior rectus fascia, was the main surgical approach (75%),
and pelvic lymph node dissections were performed in five of these
surgeries (Table III).
| Table IIIPrimary treatment modality. |
Table III
Primary treatment modality.
| Variables | n |
|---|
| n | 17 |
| Observation | 1 |
| Urachus excision | 1 |
| Transurethral bladder
tumor resection | 1 |
| Radical
cystectomy | 2 |
| Partial cystectomy +
urachus excision | 7 |
| Partial cystectomy +
urachus excision + pelvic lymph node dissection | 5 |
Tumor staging and pathology
Sheldon (6) and TNM
(6) staging systems were used to
determine tumor staging (Table
IV). According to the TNM staging system, seven cases were
defined as low grade and 10 as high grade. A review of the
pathology reports, which were available for 16 patients, revealed
that adenocarcinoma was the predominant type of tumor (87.5%), the
majority of which were mucin-producing (75%) (Table V). Two patients presented with a
pure transitional cell carcinoma. Tumors with mixed histology
(transitional cell carcinoma adenocarcinoma) and signet ring cell
adenocarcinoma were also observed. Of the five patients who
underwent lymph node dissection, two patients exhibited lymph node
invasion, which corresponded with the CT findings. A positive
surgical margin was observed in one case.
| Table IVUrachal tumor staging and grade
according to TNM staging. |
Table IV
Urachal tumor staging and grade
according to TNM staging.
| Variables | n |
|---|
| Sheldon tumor
stage |
| Ia | 0 |
| IIb | 2 |
| IIIc | 11 |
| IVd | 4 |
| TNM staging
system |
| T1N0M0 | 0 |
| T2N0M0 | 7 |
| T3N0M0 | 6 |
| T4N1M0 | 2 |
| T4N0M1 | 2 |
| Tumor grade |
| Low (grades 1 or
2) | 7 |
| High (grades 3 or
4) | 10 |
| Table VPathology of urachal carcinoma. |
Table V
Pathology of urachal carcinoma.
| Variables | n |
|---|
| n | 16 |
| Histology |
| Adenocarcinoma |
| Mucin producing
adenocarcinoma | 9 |
| Signet ring cell
adenocarcinoma | 3 |
| TCC | 2 |
| Adenocarcinoma +
TCC | 2 |
| Lymph node
dissection | 5 |
| Positive | 2 |
| Negative | 3 |
| Positive surgical
margin | 1 |
Survival
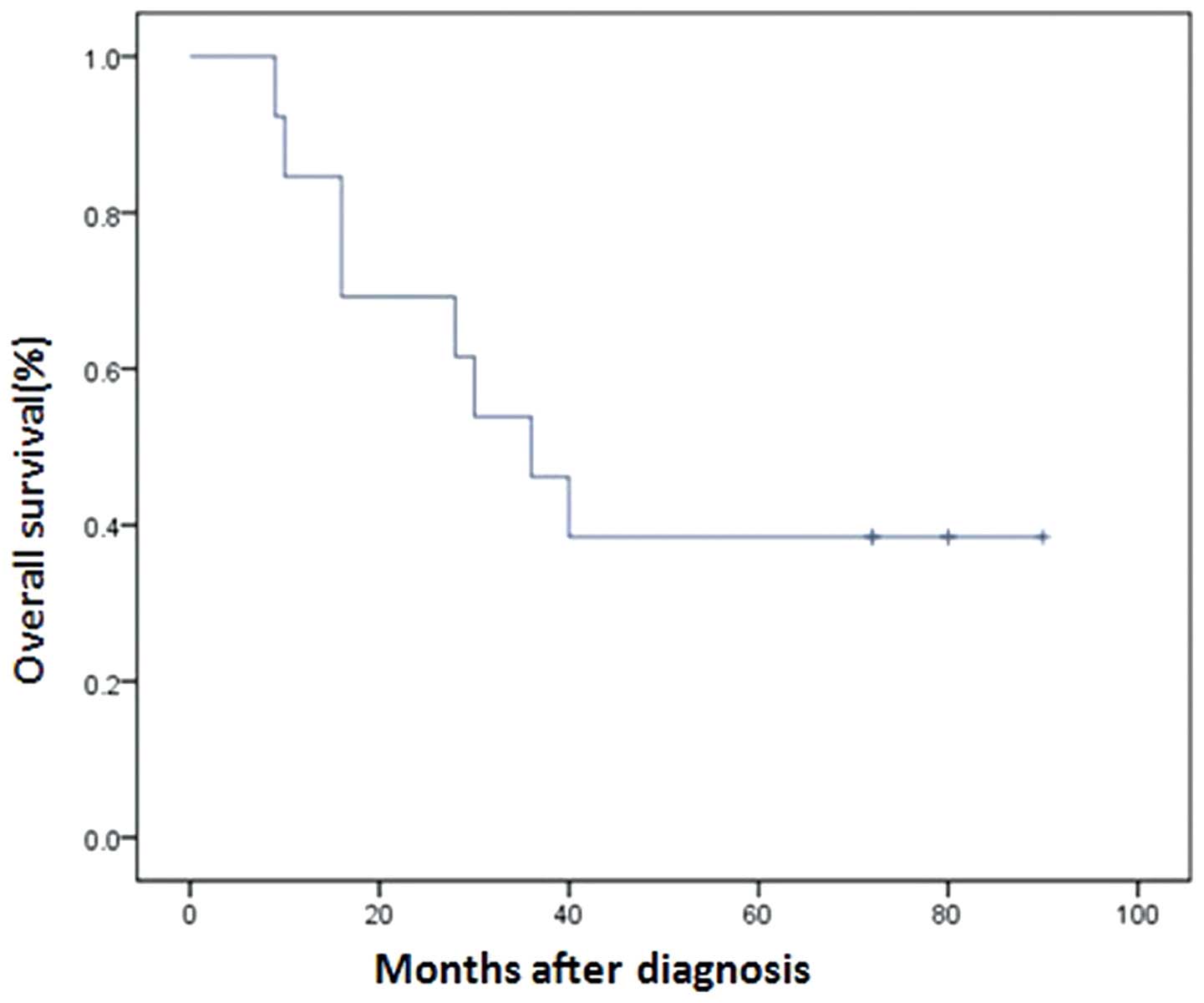
Survival data were available for all patients. Four
patients who were diagnosed later than 2008 were excluded for
survival analysis. The median overall survival time for all stages
was 57.6 months, with five patients (38.4%) alive for more than
five years following treatment (Fig.
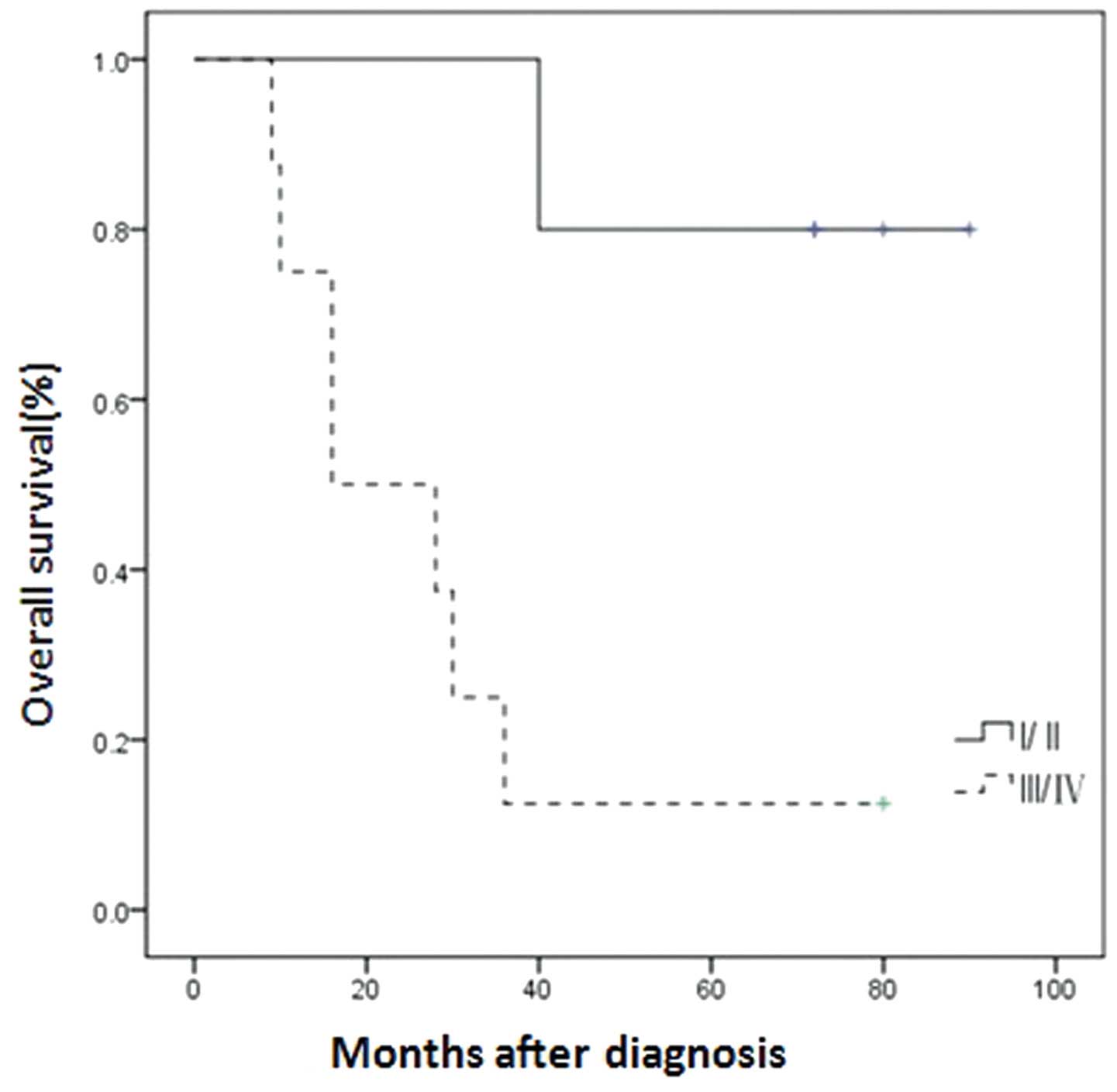
1). Using the TNM staging system, the differences in survival
were analyzed between local disease and stage II, as well as
between locally advanced and metastatic disease in stages III and
IV. The results demonstrated that the median survival time for
stage I/II patients was 6.2 years compared with a median survival
of 1.8 years (log-rank, P<0.001) for patients with advanced
disease (stage III or above) (Fig.
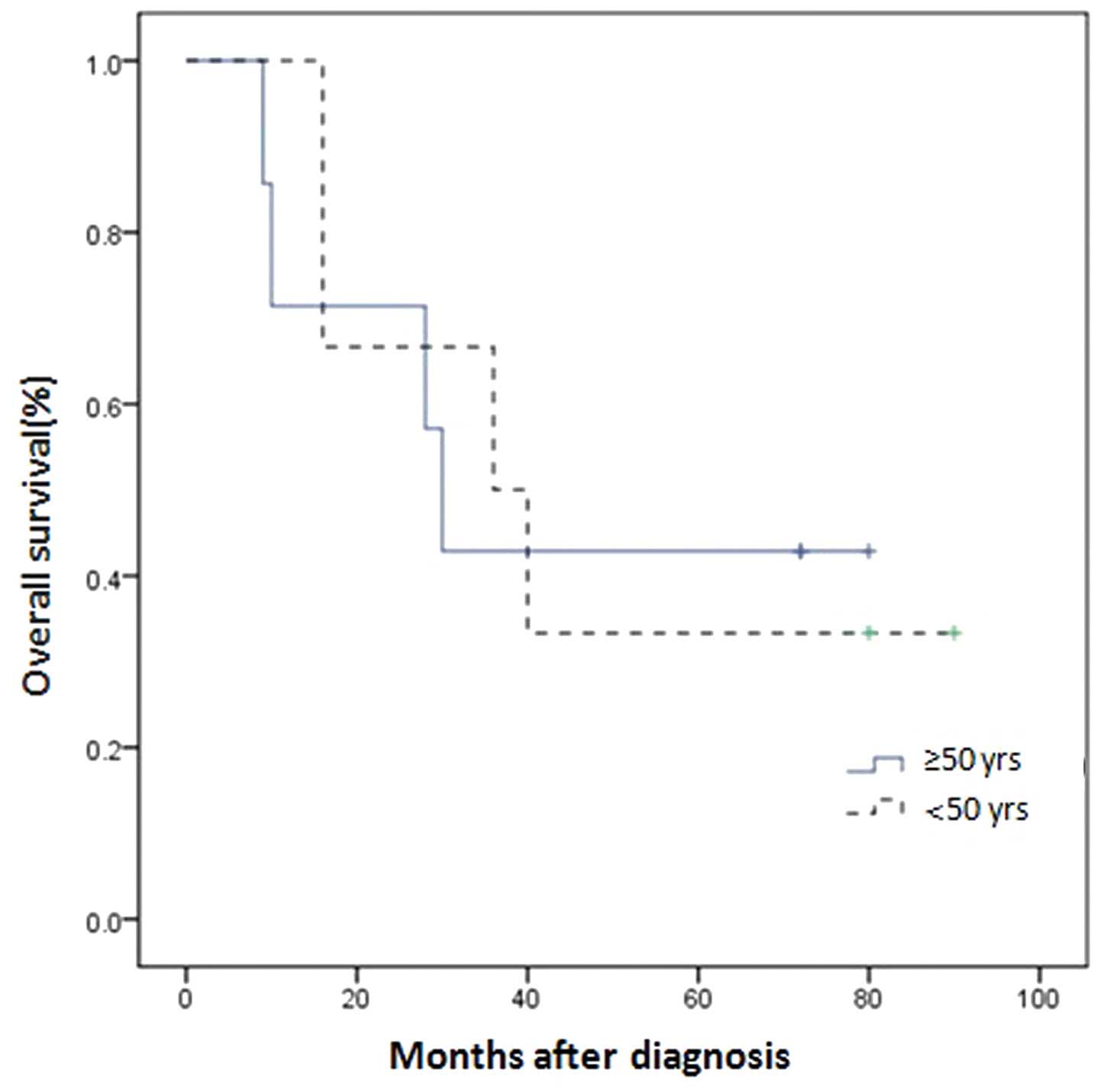
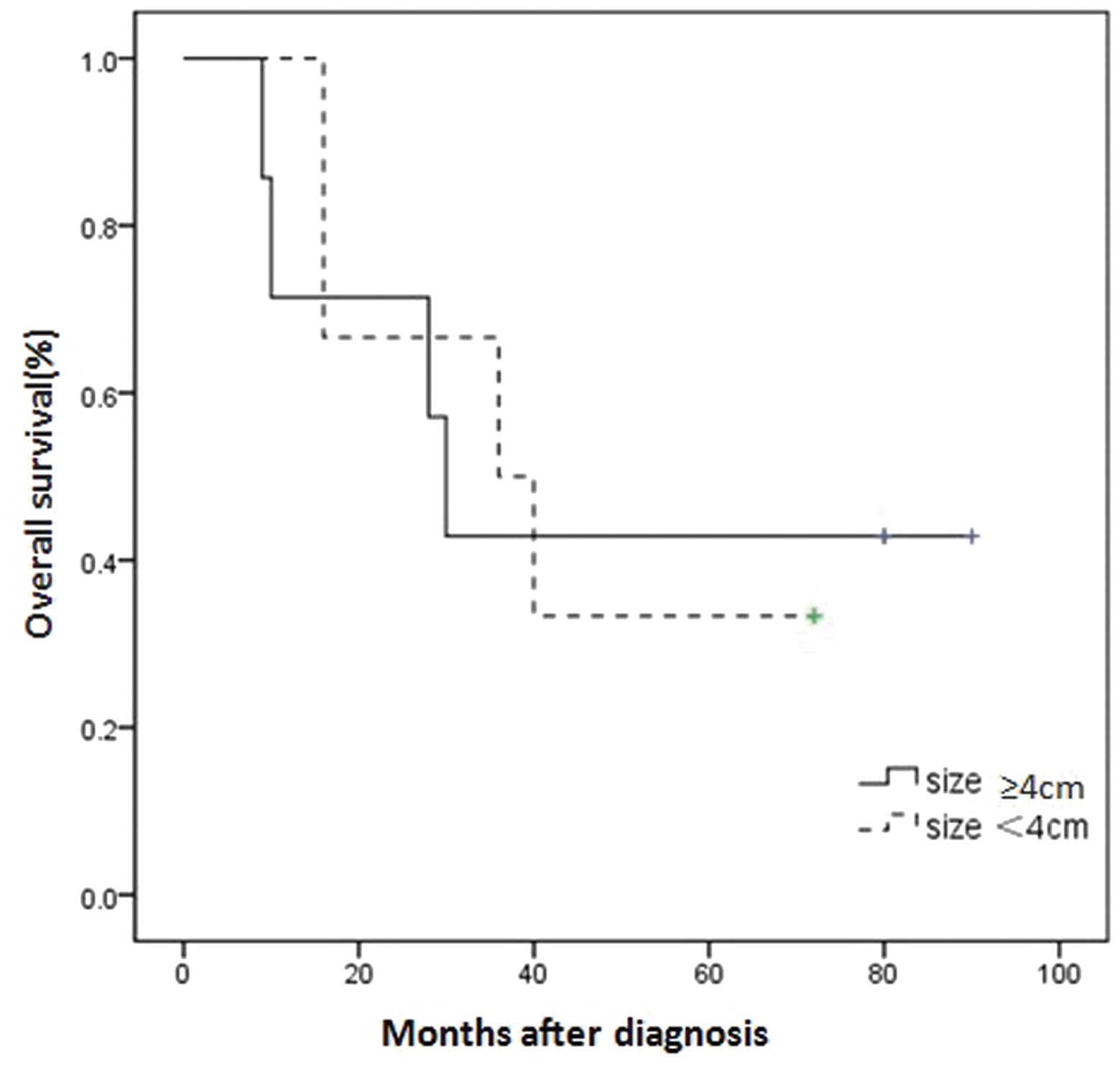
2 and Table VI). In addition,
tumor size and age showed no significant correlation with survival
(Figs. 3 and. 4).
| Table VIPrognosis according to stage of
carcinoma. |
Table VI
Prognosis according to stage of
carcinoma.
| Tumor stage | Median overall
survival time, years |
|---|
| I | NA |
| II | 6.2 |
| III | 2.4 |
| IV | 1.1 |
Discussion
The urachus usually involutes prior to birth and
remains in adults as the median umbilical ligament (7). Urachal anomalies in children often
present incidentally or with relatively benign symptoms (8), whereas in a considerable portion of
adults, urachal anomalies present as urachal carcinomas, a rare but
aggressive cancer with a poor prognosis (8).
Urachal carcinoma predominantly affects patients
between 40 and 70 years old and has a male predilection. The male
to female ratio in this series was 1.42:1, which is similar to that
observed in other reported series (9,10). No
differences have been observed in the clinical/pathological
characteristics or in the prognosis of males versus females
(5). Hematuria, dysuria and a
palpable mass have been identified to be the most frequent symptoms
(1).
US can provide a general impression of the lesion,
for example the size of the mass and location, as well as
calcification, as observed in the current study. CT is used to
confirm the US findings and provide further information with regard
to the local extent of the disease, pelvic lymph node involvement
and systemic metastases. Similar to other mucinous adenocarcinomas,
urachal carcinomas may also produce calcifications, which occur in
50–70% of cases and are considered almost pathognomonic for urachal
adenocarcinoma (7).
With the exception of patients with metastases to
distant sites, the recommended treatment is primarily surgical,
with extended partial cystectomy and en bloc excision of the
urachal mass, urachal tract and umbilicus. Removal of the adjacent
organs is also required if they are involved with the cancer tissue
(3). In the current series, two
patients underwent surgery without umbilectomy, and relapsed two
and six years following surgery. Ashley et al (11) also validated a poorer survival rate
for patients who failed to undergo umbilectomy. Furthermore, the
authors presented the hypothesis that negative surgical margin
status is one of the most significant predictors of prognosis,
which was then supported by Herr et al (12).
Bruins et al (9) demonstrated that there was no
significant difference in survival between patients who underwent
pelvic lymph node dissection and those who did not undergo
lymphadenectomy. This was substantiated by the cases presented in
the current study. With the exception of two cases with confirmed
lymph node involvement by preoperative CT and pathology, the
remaining three patients who underwent pelvic lymph node dissection
were identified to be negative for lymph node involvement, as
confirmed by pathological verification. Therefore, we recommend
that lymph node dissection is not necessary unless lymph node
involvement has been confirmed by preoperative examination.
Patients with localized disease may respond well to surgery when
umbilical resection is performed and negative surgical margins are
pursued. If this is the case, partial cystectomy provides outcomes
comparable to radical cystectomy (9).
In 1984, Sheldon proposed a staging system for
urachal cancers (Table IV)
(6). However, the Sheldon staging
system does not account for the fact that urachal tumors may occur
at any part of the urachus from the umbilicus to the bladder, and
that these extravesical cancers may invade the bladder (6). As discussed, hematuria is the
predominant symptom for patients presenting with urachal carcinoma
when initially seeking medical attention, which may be a sign of
bladder invasion. According to the Sheldon staging system, a high
proportion of patients were classified as high grade (IIIA or
above) in the this study, as only two cases were classified as low
grade. The TNM staging system was implemented and confirmed that
the anatomic location may be extrapolated to prognosis.
In this study, the median overall survival time for
all stages was 4.8 years. The determination of prognosis based on
the TNM staging system demonstrated that when the tumor is confined
to the urachus itself (stage II), the median overall survival time
is 6.2 years. However, a significant reduction in life expectancy
was observed if the patient exhibited involvement of the regional
lymph nodes or distant metastasis. The median overall survival time
for patients with distant metastatic disease was almost one year.
Patients with early-stage disease (stage II) exhibited a
statistically significant difference in survival (P<001)
compared with those with late-stage disease (stage III or IV)
(Fig. 2 and Table VI), confirming the significance of
the TNM system applied in urachal cancer. By contrast, tumor size
and age exhibited no significant correlation with survival.
In conclusion, urachal carcinomas are usually
locally advanced at presentation with a high risk of distant
metastases. Surgical excision with extended partial cystectomy, en
bloc excision of the urachal mass, urachal tract and umbilicus is
recommended. Lymph node dissection is not necessary unless lymph
node involvement has been confirmed by preoperative examinations.
The current results indicate that the most significant predictor of
prognosis is the tumor grade. In addition, the present study may
aid in the diagnosis and management of this rare tumor.
Acknowledgements
This study was supported by the National Natural
Science Foundation of China (grant no. 81101922), the Medical
Scientific Research Foundation of Guangdong Province of China
(grant nos. A2012584 and A2013606) and the Science and Technology
Development Fund Project of Shenzhen (grant no.
JCYJ20130402114702124).
References
|
1
|
Ashley RA, Inman BA, Routh JC, et al:
Urachal anomalies: a longitudinal study of urachal remnants in
children and adults. J Urol. 178(4 Pt 2): 1615–1618. 2007.
|
|
2
|
Snyder CL: Current management of umbilical
abnormalities and related anomalies. Semin Pediatr Surg. 16:41–49.
2007.
|
|
3
|
Paras FA Jr and Maclennan GT: Urachal
adenocarcinoma. J Urol. 180:7202008.
|
|
4
|
Siefker-Radtke AO, Gee J, Shen Y, et al:
Multimodality management of urachal carcinoma: the M. D. Anderson
Cancer Center experience. J Urol. 169:1295–1298. 2003.
|
|
5
|
Thieblemont C, Fendler JP, Trillet-Lenoir
V, et al: Prognostic factors of survival in infiltrating urothelial
bladder carcinoma. A retrospective study of 158 patients treated by
radical cystectomy. Bull Cancer. 83:139–146. 1996.(In French).
|
|
6
|
Molina JR, Quevedo JF, Furth AF, et al:
Predictors of survival from urachal cancer: a Mayo Clinic study of
49 cases. Cancer. 110:2434–2440. 2007.
|
|
7
|
Monteiro V and Cunha TM: Urachal
carcinoma: imaging findings. Acta Radiol Short Rep. 1:42012.
|
|
8
|
Yiee JH, Garcia N, Baker LA, et al: A
diagnostic algorithm for urachal anomalies. J Pediatr Urol.
3:500–504. 2007.
|
|
9
|
Bruins HM, Visser O, Ploeg M, et al: The
clinical epidemiology of urachal carcinoma: results of a large,
population based study. J Urol. 188:1102–1107. 2012.
|
|
10
|
Pinthus JH, Haddad R, Trachtenberg J, et
al: Population based survival data on urachal tumors. J Urol.
175:2042–2047. 2006.
|
|
11
|
Ashley RA, Inman BA, Sebo TJ, et al:
Urachal carcinoma: clinicopathologic features and long-term
outcomes of an aggressive malignancy. Cancer. 107:712–720.
2006.
|
|
12
|
Herr HW, Bochner BH, Sharp D, et al:
Urachal carcinoma: contemporary surgical outcomes. J Urol.
178:74–78. 2007.
|