Introduction
Linitis plastica is defined as a gastric cancer of
diffuse histotype (1) that presents
in the fundic gland area, and is characterized by thickening of the
stomach wall resulting in deformation of the stomach and a leather
bottle-like appearance. Since the majority of linitis plastica
patients are diagnosed at an advanced stage of the disease,
clinical outcomes are commonly observed, regardless of the extent
or type of primary resection that may have been performed (2). Linitis plastica-type gastric cancer
tumors tend to infiltrate the submucosa and muscularis propria of
the gastric wall, thus, superficial mucosal biopsies may be falsely
negative, and detecting the extent of the spread and depth of the
linitis plastica-type gastric cancer can be difficult
endoscopically. The present report describes a patient with linitis
plastica-type gastric cancer, in whom the characteristic
morphological changes in the folds of the gastric body facilitated
the determination of the spread and depth of tumor invasion.
Written informed consent was obtained from the patient.
Case report
A 66-year-old female was admitted to Kagawa
University Hospital (Kagawa, Japan) with the complaint of
intermittent epigastric pain that was exacerbated by fasting. The
patient had a history of hypertension and obstructive sleep apnea
syndrome. Physical examination upon admission revealed no anemia
(via conjunctival pallor examination), jaundice or pulmonary
abnormalities. On palpation, the abdomen of the patient was soft
and flat, with no areas of tenderness. Furthermore, pretibial edema
was not observed and superficial lymph nodes were not palpable.
Serum concentrations of the tumor markers, carcinoembryonic antigen
and carbohydrate antigen 19-9, were within the normal ranges (<5
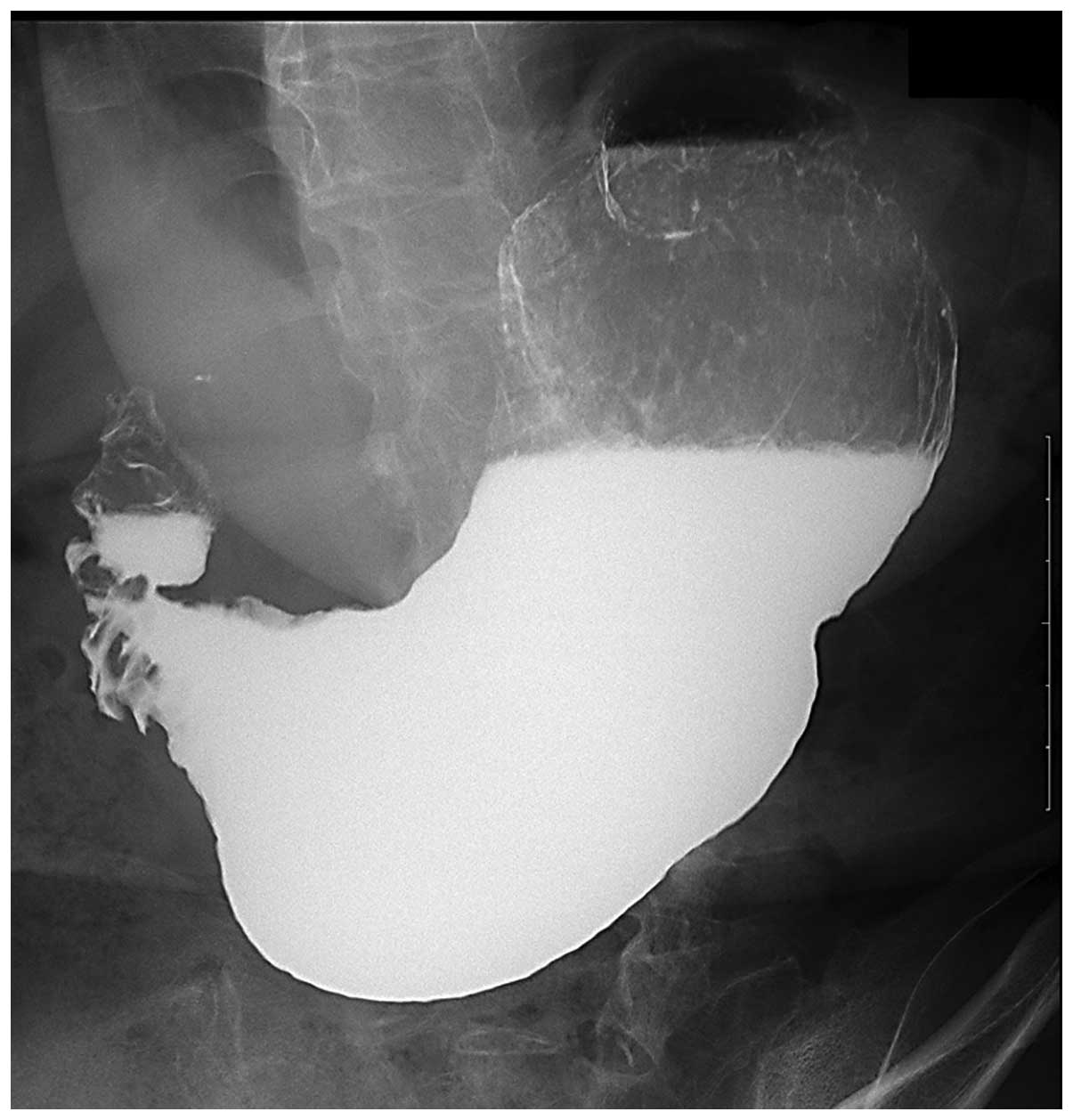
ng/ml and 0–37 U/ml, respectively). However, X-ray examination
indicated reduced gastric distension, as well as deformation of the
stomach, which exhibited a leather bottle-like appearance (Fig. 1). In addition, the lower gastric
body demonstrated luminal narrowing and increased rigidity, with a
depressed lesion (longest diameter, 20 mm) at the posterior wall of
the gastric antrum and abdominal computed tomography revealed
thickening of the antrum. No lymphadenopathy was observed.
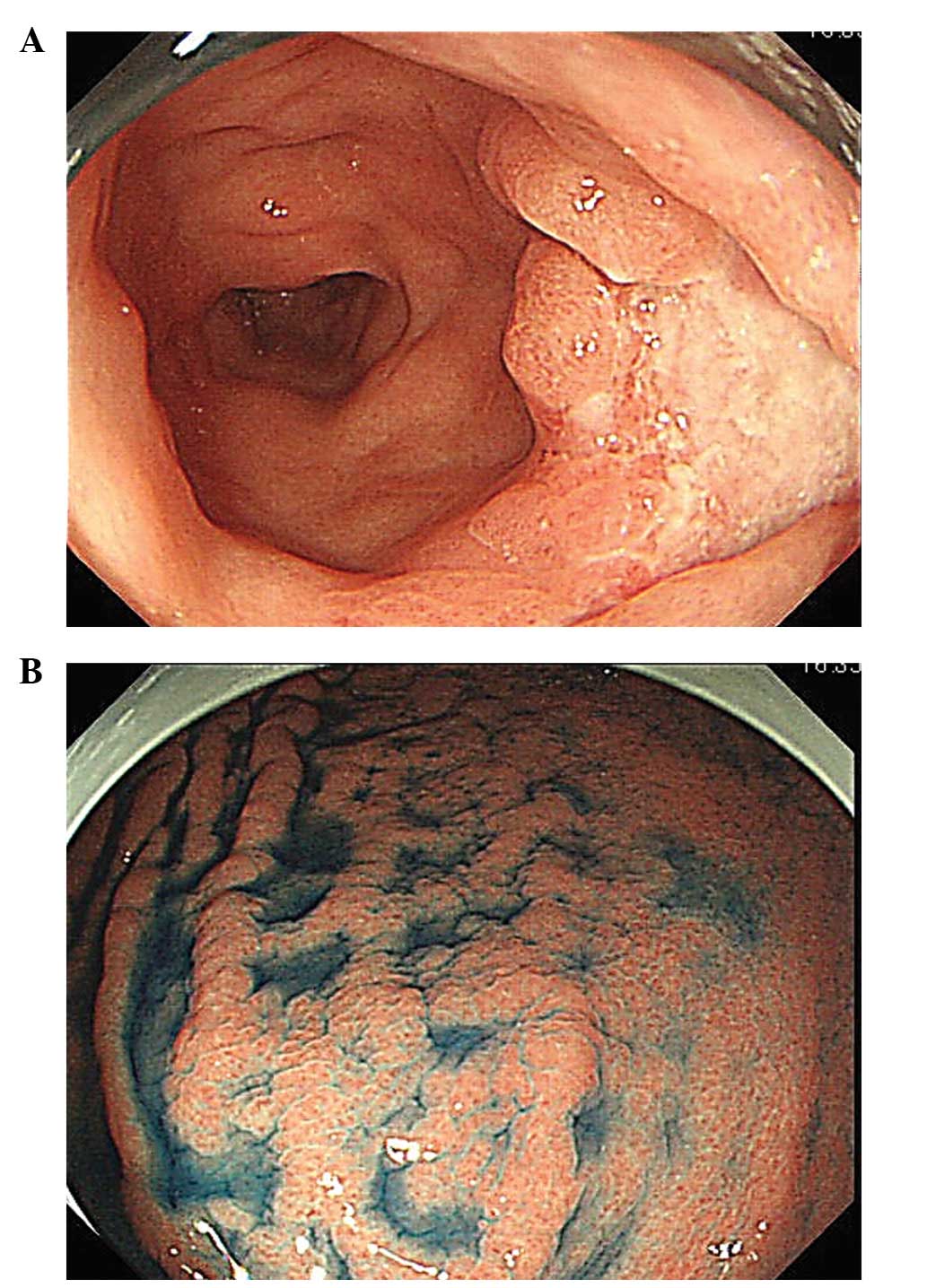
Additionally, endoscopy revealed an ulcerative lesion covered by a
white necrotic substance on the posterior wall of the antrum
(Fig. 2A) and severe luminal
narrowing, with poor distension of the lower gastric body. The
upper gastric body, however, demonstrated good extension when
compared with the middle and lower gastric bodies. The folds of the
gastric antrum were flexible, stretched smoothly, and crossed one
another, resulting in a waffle-like appearance on the greater
curvature of the upper gastric body (Fig. 2B). Analysis of biopsy specimens from
the ulcerative lesion revealed a poorly differentiated
adenocarcinoma containing signet ring cells, however, adenocarinoma
was absent from biopsy specimens obtained from the abnormally
crossed folds. Due to the morphological changes that occured in the
gastric folds, creating the waffle-like appearance, it was
determined that cancer cell invasion of the upper gastric body was
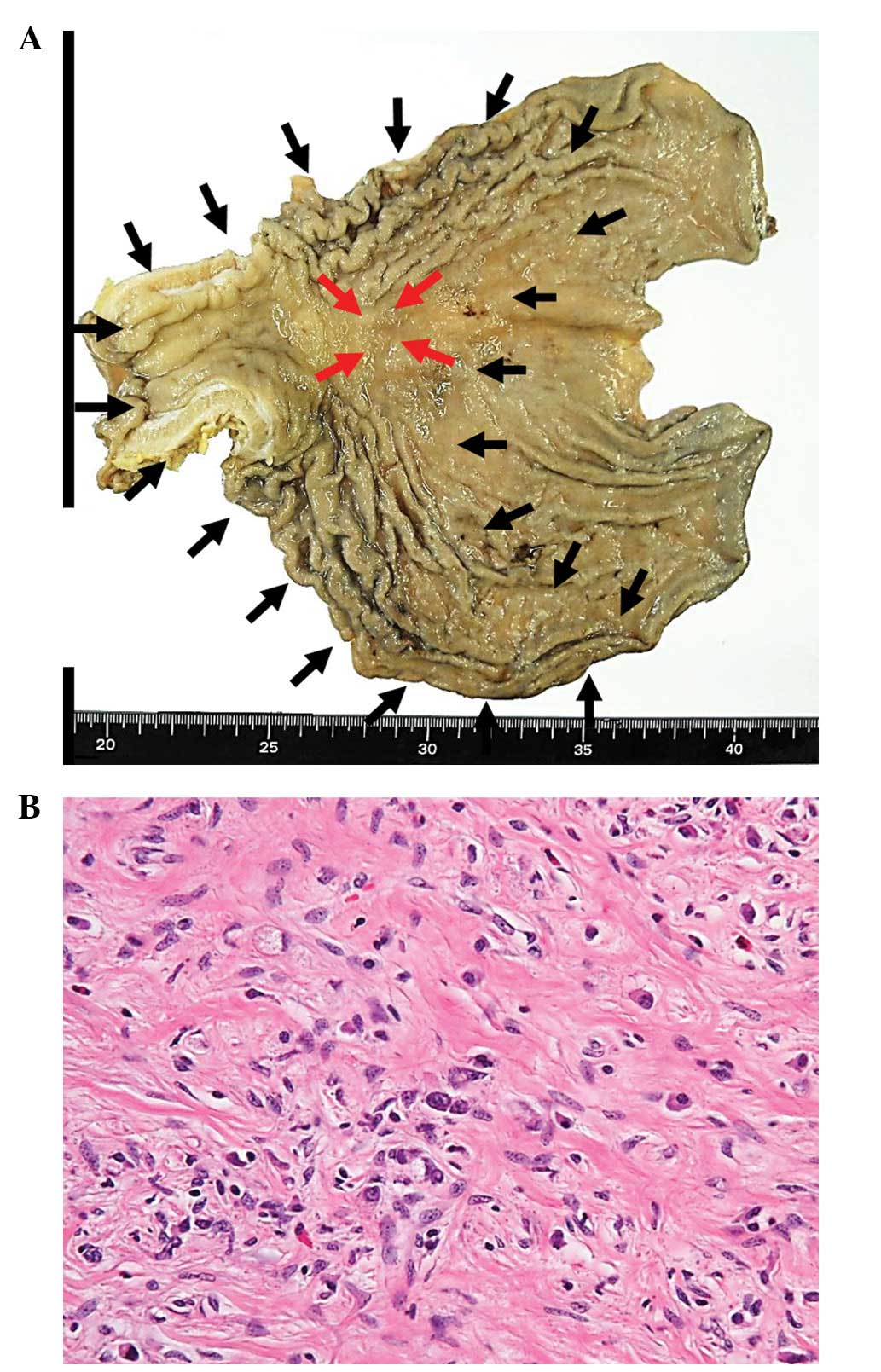
likely, and a total gastrectomy was performed. The resected
specimen revealed the wall thickening and crossing folds of the
gastric body (Fig. 3A) that were
previously observed by endoscopy. Microscopic examination revealed
that cancer cells had spread throughout the upper gastric body and
had infiltrated the vessels in the submucosa, predominately into
the muscularis propria, and marginally into the serosa (Fig. 3B). Immunohistochemical examination
revealed positive staining for MUC5AC and MUC6 (gastric marker
mucins) and negative staining for MUC2 and CD10 (intestinal marker
mucins), indicating gastric-type mucin expression. The final
diagnosis, according to the Japanese Classification of Gastric
Carcinoma (3), was T4aN3aM0,
clinical stage IIIC advanced gastric cancer. The patient was
discharged 17 days after surgery without complications and
commenced three cycles of S-1 adjuvant chemotherapy (80 mg/day,
days 1–28) for 16 weeks. Following three courses of chemotherapy
for 16 weeks, treatment was terminated due to patient fatigue. The
patient has survived and is without disease recurrance 14 months
after surgery.
Discussion
The Japanese Classification of Gastric Carcinoma has
defined Type IV diffuse infiltrative gastric cancer as tumors
lacking marked ulceration or raised margins, but with thickened and
indurated gastric walls, and poorly defined margins (3). Type IV carcinoma, or scirrhous gastric
carcinoma, is therefore a diffuse infiltrating adenocarcinoma,
which is predominantly poorly differentiated and lacking a
circumscribed lesion. Tumor involvement of the entire stomach wall
results in a condition termed linitis plastica (4). Despite improved treatment outcomes for
other types of gastric carcinoma in Japan, the prognosis of
patients with linitis plastica remains particularly poor (5,6).
Endoscopic brush cytology and biopsy techniques have
an overall sensitivity of 95–98% in the detection of gastric cancer
(7,8). However, the accuracy of endoscopy
ranges widely, depending on the gross tumor growth pattern and the
anatomic location of the tumor (9),
with a sensitivity of only 33–73% observed in linitis plastica
patients (9–12). The predominant reason for the poor
sensitivity of endoscopy in the detection of scirrhous gastric
cancer is the healthy appearance of the mucosa.
Although the invasion and spread of linitis
plastica-type gastric cancer is difficult to diagnose prior to
surgery, the presence of depressed lesions and marginal changes in
the gastric folds may be indicators for diagnosis. Endoscopic
findings that are characteristic of scirrhous gastric cancer
include poor distension of the gastric walls, morphological changes
in the gastric folds and the presence of primary lesions (13). The differential diagnosis of
thickened gastric folds includes Ménétrier’s disease, hypertrophic
gastritis, malignant lymphoma, rare types of aberrant pancreas,
syphilis and cytomegalovirus gastritis (14). Morphological changes in the gastric
folds of linitis plastica patients include the presence of giant,
swollen, straight, furrowed and crossed folds. These morphological
changes are important for distinguishing linitis plastica from
other diseases. Further diagnostic indicators of linitis plastica
include poor distention of the stomach, and a leather bottle-like
appearance as observed by gastrointestinal (GI) series, indicating
that an upper GI series may be superior to endoscopic examination
in the diagnosis and localization of these types of lesions
(15). By contrast, certain linitis
plastica-type gastric cancer patients do not demonstrate the
typical deformity, poor distension, or irregular folds via upper GI
series, however, exhibit focal alterations in infiltrated areas
(16).
Linitis plastica is also characterized by poorly
differentiated tumor cells that diffusely infiltrate the gastric
wall, thus leading to reactive fibrosis (17). Early stage, undifferentiated [0-IIC
morphological type (3)], linitis
plastica-type gastric cancer is present in the mucosa of the
gastric wall, progressing by diffuse infiltration into the
submucosal layer prior to ulceration of the primary lesion, with
the cancer cells extending beyond the fibrous tissue. In patients
with mild fibrosis, the stomach distends well upon air
insufflation, with the gastric body occasionally exhibiting a
waffle-like appearance; these observations may be important in the
accurate diagnosis of the spread of cancer cell invasion.
Recently, we performed a bloc biopsy, using the
submucosal endoscopy mucosal flap to diagnose submucosal tumors
(18–20). This technique lead to
histopathological diagnosis without any complications, such as
hemorrhage or dissemination of tumor. In the future, this method
may exhibit potential diagnosis value for accurately diagnosing a
linitis plastica-type gastric cancers.
In conclusion, accurately diagnosing the spread and
depth of linitis plastica-type gastric cancer requires examination
of the morphological changes in the gastric folds, as well as
examination of the primary depressed lesion. The use of novel
methods, such as bloc biopsy, may improve the accuracy of linitis
plastic-type gastric cancer diagnosis.
References
|
1
|
Lauren P: The two histological main types
of gastric carcinoma: diffuse and so-called intestinal-type
carcinoma. An attempt at a histo-clinical classification. Acta
Pathol Microbiol Scand. 64:31–49. 1965.PubMed/NCBI
|
|
2
|
Pedrazzani C, Marrelli D, Pacelli F, et
al: Gastric linitis plastica: which role for surgical resection?
Gastric Cancer. 15:56–60. 2012. View Article : Google Scholar
|
|
3
|
Japanese Gastric Cancer Association.
Japanese classification of gastric carcinoma: 3rd English edition.
Gastric Cancer. 14:101–112. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Whitehead R, Johansen A and Rubio CA:
Other tumors of the stomach. Gastrointestinal and Oesophageal
Pathology. Whitehead R: 2nd edition. Churchill Livingstone; New
York, NY: pp. 823–836. 1995
|
|
5
|
Otsuji E, Kuriu Y, Okamoto K, et al:
Outcome of surgical treatment for patients with scirrhous carcinoma
of the stomach. Am J Surg. 188:327–332. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kodera Y, Yamamura Y, Ito S, et al: Is
Borrmann type IV gastric carcinoma a surgical disease? An old
problem revisited with reference to the result of peritoneal
washing cytology. J Surg Oncol. 78:175–182. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Qizilbash AH, Castelli M, Kowalski MA and
Churly A: Endoscopic brush cytology and biopsy in the diagnosis of
cancer of the upper gastrointestinal tract. Acta Cytol. 24:313–318.
1980.PubMed/NCBI
|
|
8
|
Llanos O, Guzmán S and Duarte I: Accuracy
of the first endoscopic procedure in the differential diagnosis of
gastric lesions. Ann Surg. 195:224–226. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Winawer SJ, Posner G, Lightdale CJ,
Sherlock P, Melamed M and Fortner JG: Endoscopic diagnosis of
advanced gastric cancer. Factors influencing yield.
Gastroenterology. 69:1183–1187. 1975.PubMed/NCBI
|
|
10
|
An-Foraker SH and Vise D: Cytodiagnosis of
gastric carcinoma, linitis plastica type (diffuse, infiltrating,
poorly differentiated adenocarcinoma). Acta Cytol. 25:361–366.
1981.PubMed/NCBI
|
|
11
|
Levine MS, Kong V, Rubesin SE, Laufer I
and Herlinger H: Scirrhous carcinoma of the stomach: radiologic and
endoscopic diagnosis. Radiology. 175:151–154. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Evans E, Harris O, Dickey D and Hartley L:
Difficulties in the endoscopic diagnosis of gastric and oesophageal
cancer. Aust N Z J Surg. 55:541–544. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maruyama Y, Kageoka M, Nagata K, et al:
Endoscopic diagnosis based on typical findings of scirrhous gastric
cancer. Stomach Intestine. 45:445–455. 2010.
|
|
14
|
Murata Y, Yamasaki T, Kitamura Y, et al:
Diagnostic points of endoscopic ultrasonographic findings in
scirrhous gastric cancer. Stomach Intestine. 45:457–467. 2010.
|
|
15
|
Park MS, Ha HK, Choi BS, et al: Scirrhous
gastric carcinoma: endoscopy versus upper gastrointestinal
radiography. Radiology. 231:421–426. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yamamoto T, Nagahama R, Nakashima H, et
al: Basis of the diagnosis and feature of scirrhous gastric cancer.
Stomach Intestine. 45:428–444. 2010.
|
|
17
|
Kodera Y, Nakanishi H, Ito S, et al:
Detection of disseminated cancer cells in linitis plastica-type
gastric carcinoma. Jpn J Clin Oncol. 34:525–531. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kobara H, Mori H, Rafiq K, et al:
Evaluation of gastric submucosal tumors using endoscopically
visualized features with submucosal endoscopy. Oncol Lett.
8:161–168. 2014.PubMed/NCBI
|
|
19
|
Kobara H, Mori H, Fujihara S, et al: Bloc
biopsy by using submucosal endoscopy with a mucosal flap method for
gastric subepithelial tumor tissue sampling (with video).
Gastrointest Endosc. 77:141–145. 2013. View Article : Google Scholar
|
|
20
|
Kobara H, Mori H, Fujiwara S, Nishiyama N,
Kobayashi M and Masaki T: Bloc biopsy by tunneling method using
endoscopic submucosal dissection for an upper gastrointestinal
submucosal tumor. Endoscopy. 44(Suppl 2): S197–S198. 2012.
View Article : Google Scholar
|