Introduction
Craniopharyngioma is a slow-growing benign tumor
that develops in the parasellar or sellar region of the brain
(1,2). Accounting for 6–9% of brain tumors in
children (3), craniopharyngioma is
the third most common type of childhood intracranial tumor
(4) and the most common type of
pediatric tumor in the hypothalamus and pituitary region, worldwide
(5). In adults, craniopharyngioma
typically occurs after the age of 60 years. According to an
American study, the incidence rate of this tumor is low, at ~0.13
cases per 100,000 individuals/year, and does not vary with gender
or ethnicity (6). Although
craniopharyngioma can be highly aggressive and has a tendency to
recur following surgical removal, the literature indicates that it
rarely demonstrates malignant behavior (7–9).
Despite the tumor being histologically benign, it is connected to
surrounding vital structures, such as the pituitary gland, the
optic chiasm, the circle of Willis and the hypothalamus, creating
challenges for craniopharyngioma treatment and a high rate of
morbidity (10). As demonstrated by
data provided by the National Cancer Database, the five-year
survival rate of patients with these tumors is 80%, and this rate
decreases with increasing age (6).
Despite continuous progress in microsurgery
techniques and years of research, the treatment of
craniopharyngioma remains a significant problem, particularly for
children (11). The unique
anatomical structure of the suprasellar region and the connection
of the tumor to surrounding tissues with critical functions results
in difficulties in the removal of the tumor (3,12).
With the development of novel surgical techniques and
post-operative endocrine therapy, mortality and morbidity caused by
craniopharyngioma have been greatly reduced, with the rate of total
resection reaching up to 90% (12,13).
However, a certain degree of controversy remains regarding the
origin, histology and pathology of craniopharyngioma, as well as
the optimal treatment strategy (2,14,15).
In the present study, the ultrastructure of
craniopharyngioma was observed using electron microscopy and
immunohistochemistry, with the aid of digital image analysis
techniques, and survivin protein expression levels in
craniopharyngioma were assessed to determine the biological
characteristics and pathogenesis of craniopharyngioma.
Materials and methods
Patients and inclusion criteria
The paraffin-embedded samples of 50 patients
admitted to the West China Hospital of Sichuan University (Chengdu,
China) and diagnosed with craniopharyngioma following surgical
resection between January 2000 and December 2005 were selected for
use in the present study. The inclusion criteria were as follows:
i) A complete patient medical history must be available; ii) the
patient must have undergone pre-operative imaging (computed
tomography or magnetic resonance imaging); iii) the pathology
sample must be a sufficient size and have been established as
craniopharyngioma by the Department of Pathology of the West China
Hospital; and iv) the patient must have not have received radiation
therapy, so as to eliminate the impact of radiation. According to
the standard classification of central nervous system tumors
published by the World Health Organization in 2000 (16), 33/50 cases (66%) were
adamantinomatous craniopharyngioma and 17/50 cases (34%) were
squamous-papillary craniopharyngioma. The present study included 32
male and 18 female patients, aged 4–66 years old (mean age, 29.12
years old). All of the patients were followed up by phone until
November 2010. A total of 10 healthy brain tissue samples obtained
from epileptic patients that had undergone surgery were used as the
control group. This study was approved by the ethics committee of
West China Hospital of Sichuan University and written informed
consent was obtained from all patients.
Measuring survivin expression
Survivin protein expression levels in the
craniopharyngioma tissues were detected using immunohistochemistry
and then quantitatively analyzed. Apoptotic cells were stained with
transferase dUTP nick end labeling-peroxidase (TUNEL-POD; Roche,
Branchburg, NJ, USA) and observed using transmission electron
microscopy (Hitachi H-600IV; Hitachi, Ltd., Tokyo, Japan). Under
the light microscope, survivin-positive cells were observed as
brown granules in the nucleus or cytoplasm. For each section, a
charge-coupled device camera was used to capture at least five
fields of view at a magnification of ×400 (Olympus BX51 CCD; P70;
Olympus Corporation, Tokyo, Japan), and Image-Pro Plus software
(version 5.0; Media Cybernetics, Rockville, MD, USA) was used to
quantitatively analyze the images; integrated optical density (IOD)
was selected as the parameter to indicate survivin protein
expression levels and the average IOD of all the recorded images
was determined. Furthermore, TUNEL-POD stained the nuclei of the
apoptotic cells yellow or brown, while the nuclei of the
non-apoptotic cells were blue.
Statistical analysis
Statistical analysis was performed using SPSS
software, version 13.0 (SPSS, Inc., Chicago, IL, USA).
Non-parametric tests were performed for each factor, and
multinomial and ordinal logistic regression was performed.
P<0.05 was used to indicate a statistically significant
difference.
Results
Morphological observation
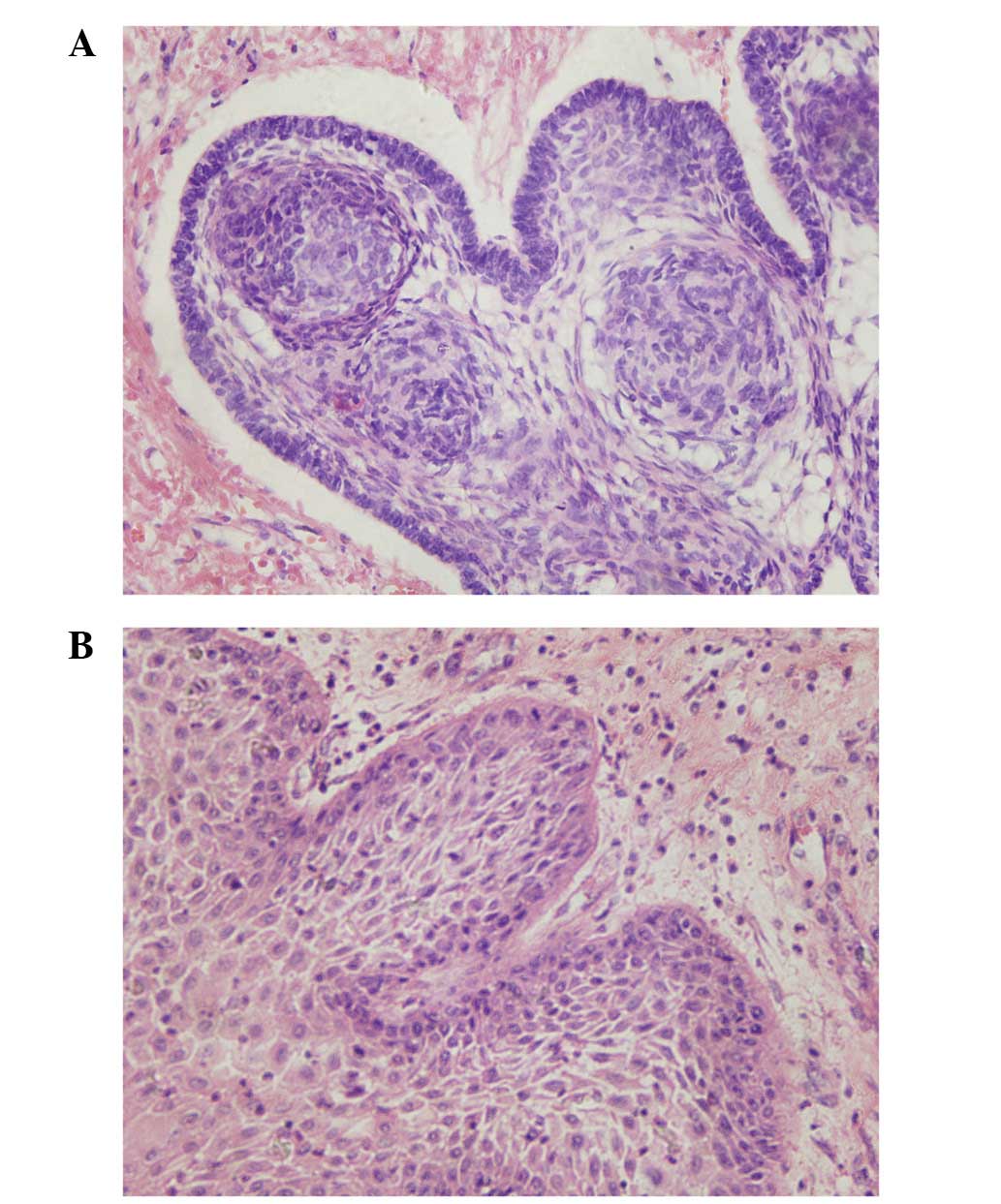
Adamantinomatous (Fig.
1A) and squamous-papillary (Fig.
1B) craniopharyngioma were observed using light microscopy
following hematoxylin and eosin staining. Adamantinomatous
craniopharyngioma is often observed in children and has cell cord
and island similar to that of ameloblastoma. The observations
revealed that the outermost layer of cells were palisade basal
cells, which are cylindrical cubic epithelial cells, while the
middle layer of cells were stratified polygonal squamous epithelial
cells and the innermost layer of cells consisted of loosely
structured reticular cells and wet keratin. Furthermore, local
invasion of the surrounding healthy brain tissue was observed. By
contrast, squamous-papillary craniopharyngioma is predominantly
observed in adults, exhibiting a unique epithelium with a
fibrovascular center. The present observations revealed that no
microcapsules appeared to have formed, however, a palisade-like
nucleus, a keratin pearl, wet keratin, calcification and
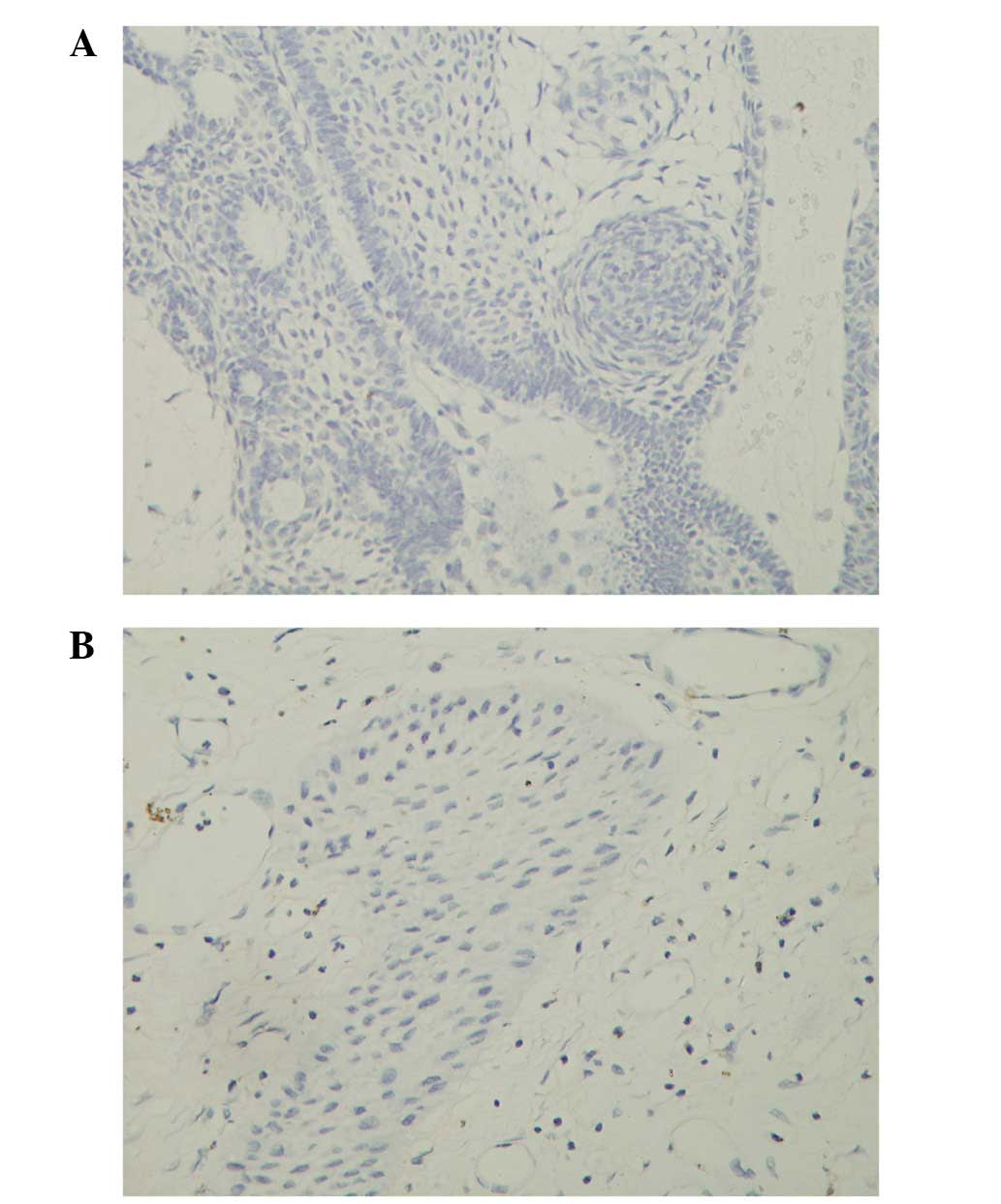
significant inflammation were observed. The majority of cells in
the adamantinomatous (Fig. 2A) and
squamous-papillary (Fig. 2B)
craniopharyngioma samples were not stained by TUNEL-POD, indicating
a low rate of apoptosis.
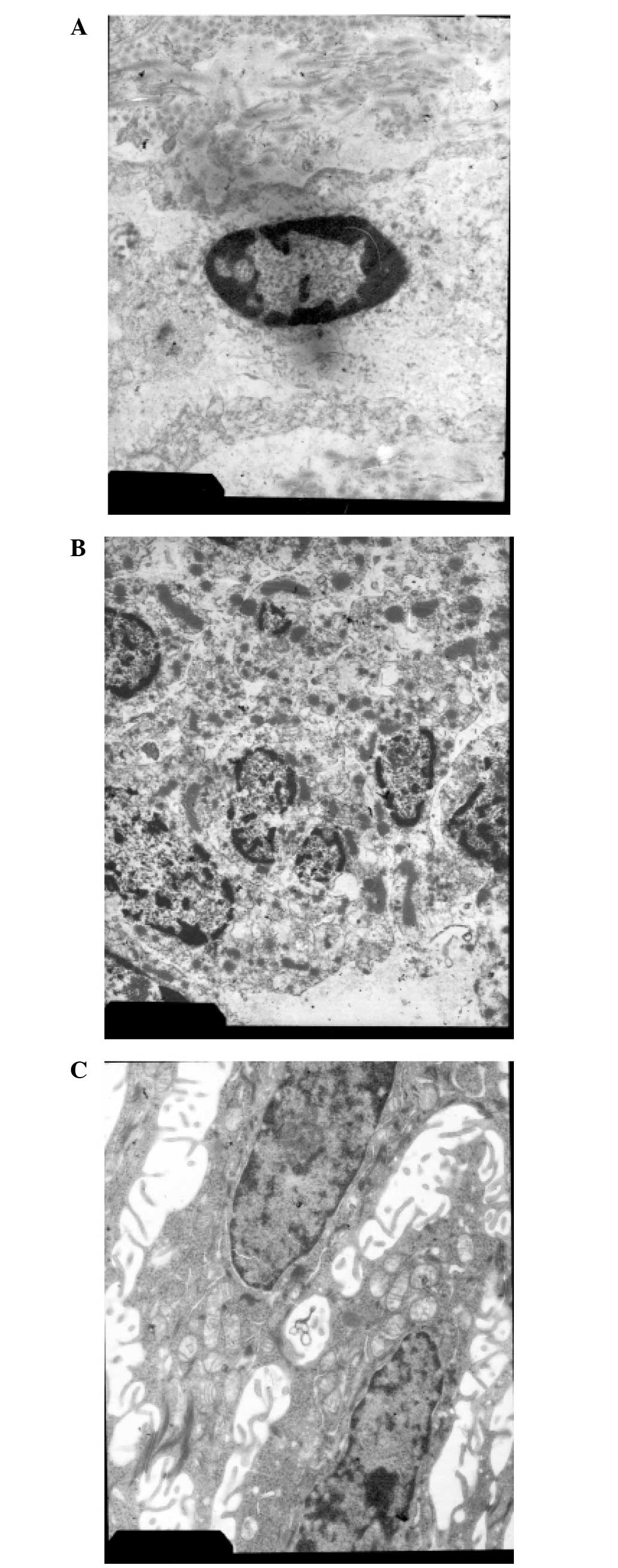
Different types of tumor cells were observed using
electron microscopy. The nuclei of the apoptotic tumor cells
(Fig. 3A) were oval in shape and
condensed into a uniformly dense structure. The chromatin had
migrated to the edge of the nucleus on the inner side of the
nuclear membrane, and the nuclear and cell membranes were
integrated. Necrotic tumor cells appeared to die in clusters with
damaged nuclear membranes and irregularly broken and condensed
chromatin, forming sparse reticular clots (Fig. 3B). The ultrastructure of the
craniopharyngioma cells was similar to that of squamous epithelial
cells (Fig. 3C). The cells were
densely packed into stratified epithelial clumps with a large,
oval-shaped and slightly deformed nucleus, and an integrated, but
rugged nuclear membrane. Chromatin distribution was even, abundant
tonofibrils were observed in the cytoplasm, and mitochondria, rough
endoplasmic reticulum, ribosomes and other organelles were clearly
visible. Furthermore, abundant microvilli were observed on the cell
surface, and the cells were loosely arranged with a vast cell gap
in which integrated intercellular desmosomes and multiple
connections appeared to have formed.
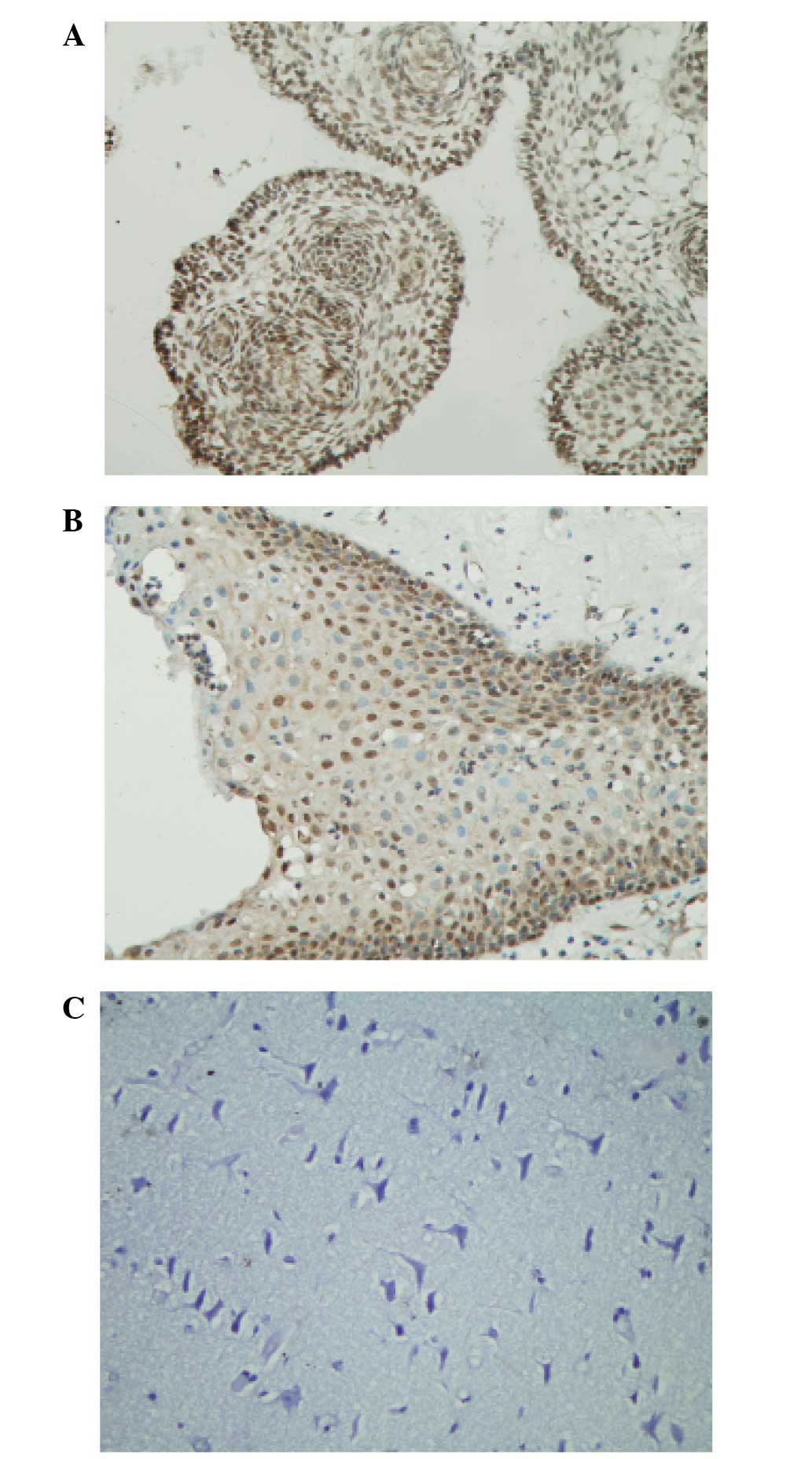
Survivin protein expression levels
Survivin protein expression was detected in all 50
craniopharyngioma samples in the cytoplasm or the nucleus. In
adamantinomatous craniopharyngioma (Fig. 4A), significant survivin expression
was detected in the majority of tissue sections and the cells
predominantly exhibited higher expression levels in the nucleus
compared with the cytoplasm. High survivin expression was
predominantly observed in the palisade-like epithelial cells, as
well as cells in the finger-like or clump-like cell clusters. The
stellate reticular cells exhibited relatively weak survivin
expression levels and the expression pattern in the
squamous-papillary craniopharyngioma (Fig. 4B) was similar to that of the
adamantinomatous craniopharyngioma. Furthermore, survivin-positive
cells were predominantly terminally differentiated squamous
epithelial cells. Survivin was highly expressed in the nucleus and
poorly expressed in the cytoplasm of the craniopharyngioma cells;
however, no survivin expression was detected in the 10 healthy
brain tissue sections (P<0.001; Fig.
4C).
The images of Fig. 4A, B
and C were analyzed using Image-Pro Plus software, and the IOD
was selected as the parameter to indicate survivin protein
expression level, with a higher IOD indicating higher survivin
expression. Survivin expression was found to be significantly
higher in the craniopharyngioma tissues (50 cases) compared with
the healthy control (10 cases) samples (P<0.001). All patients
≤16 years old exhibited adamantinomatous craniopharyngioma, while
among the 33 patients >16 years old, 16 exhibited the
adamantinomatous tumor type (48.5%) and 17 patients exhibited the
squamous-papillary type (51.5%). Furthermore, survivin expression
was significantly higher in adamantinomatous craniopharyngioma (33
cases) compared with squamous-papillary (17 cases)
craniopharyngioma (P=0.036). Compared with the female
craniopharyngioma patients (18 cases), the level of survivin
expression was significantly higher in the overall male
craniopharyngioma patient population (32 cases) (P=0.002) and in
those males with the adamantinomatous tumor type (P<0.001).
However, the difference in survivin expression levels between the
male and female squamous-papillary craniopharyngioma patients was
not statistically significant. Survivin expression was
significantly higher in the patients ≤16 years old (17 cases)
compared with the patients >16 years old (33 cases) (P=0.002).
No statistically significant differences were detected between the
three subtypes of craniopharyngioma (cystic, 26 cases; solid, 13
cases; and mixed-type, 11 cases); or between the different disease
courses (≤12-month disease course, 39 cases; and >12-month
disease course, 11 cases). However, the survivin expression levels
were significantly higher in the recurrent craniopharyngioma tumors
(9 cases) compared with the non-recurrent tumors (41 cases)
(P=0.011).
Regression analysis
All the patients in the present study were followed
up by phone until the end of November 2010; however, the required
information was only collected from 46 patients. The cases of
craniopharyngioma were divided into five grades: Grades I, II, III
and IV, as described by Carmel et al (17), plus mortality. Multinomial and
ordinal logistic regression was performed to evaluate the candidate
risk factors for prognosis. In the present model, prognosis was
defined as a dependent variable, and pathological type, age, tumor
subtype, complications and survivin expression level (IOD value)
were defined as independent variables.
A significant correlation was demonstrated between
complication as a risk factor for the prognosis of
craniopharyngioma patients and prognosis (P<0.05); patients with
no complications exhibited a significantly more favorable prognosis
compared with patients who experienced complications. However, no
significant correlation was detected among all other candidate risk
factors.
Discussion
Controversy regarding the origin of
craniopharyngioma has always been present, and two expounding
theories currently exist: The embryonic origin theory and the
metaplasia theory. Certain individuals believe that it is the
residual ectoderm cells in the primary cranial pharyngeal tube and
anterior pituitary that form craniopharyngioma (18,19).
In the present study, it was identified that all patients ≤16 years
old exhibited adamantinomatous craniopharyngioma. We speculate that
adamantinomatous craniopharyngioma may originate from residual
ectoderm cells, which appears to support Erdheim’s embryonic origin
theory (20). However, it is
unlikely that squamous-papillary craniopharyngioma also originates
from residual embryonic ectoderm cells, since the present study
identified no cases of squamous-papillary craniopharyngioma in
patients ≤16 years old. Instead, it was proposed that
squamous-papillary craniopharyngioma may have a different origin.
The metaplasia theory states that craniopharyngioma originates from
metaplasia of adenohypophysis and the anterior infundibular
squamous epithelium (2,14,21).
In the present study, it was identified that no individuals ≤16
years old exhibited squamous-papillary craniopharyngioma,
contradicting the embryonic origin theory, in which such a cell
nest should be primarily be observed in children. In addition, such
cell nests are commonly observed in patients who are >20 years
old (22). However, the present
study identified that survivin is expressed in significantly higher
levels in adamantinomatous craniopharyngioma tissues compared with
squamous-papillary craniopharyngioma tissues. Under normal
circumstances, survivin is only expressed during embryonic and
fetal development, and not in adults, thus, it was speculated that
adamantinomatous craniopharyngioma originates from residue embryo
tissues, while squamous-papillary craniopharyngioma originates from
squamous metaplasia.
Histologically, craniopharyngioma can be divided
into the adamantinomatous and squamous-papillary types. The
majority of children with craniopharyngioma exhibit the
adamantinomatous form, however, an equal proportion of the two
types are observed in adults (2).
Furthermore, Tavangar et al (23) identified that squamous-papillary
craniopharyngioma only occurs in adults; this form of the disease
has fewer clinical manifestations and a lower risk of recurrence
compared with adamantinomatous craniopharyngioma. Additionally,
Crotty et al (24)
identified that adamantinomatous craniopharyngioma predominantly
occurs in adolescents and was more invasive than squamous-papillary
craniopharyngioma. Consistent with these previous studies, the
present study observed that all the patients who were ≤16 years old
exhibited adamantinomatous craniopharyngioma and that all the
patients who were >16 years old had an equal chance of
developing each type of craniopharyngioma. A low recurrence rate
was observed (9/50 cases; 18%), in accordance with the benign
nature of adamantinomatous craniopharyngioma. Of the nine cases of
recurrence, two (22.2%) were of a squamous-papillary type and seven
(77.8%) were adamantinomatous, consistent with the above mentioned
studies. Light microscopy demonstrated that adamantinomatous
craniopharyngioma often invaded the surrounding healthy tissue,
however, this phenomenon was not observed in the squamous-papillary
craniopharyngioma tissues, thus, adamantinomatous craniopharyngioma
appeared to exhibit a higher level of invasiveness. However,
electron microscopy of 10 cases of craniopharyngioma by Kawano
et al (25) demonstrated
that although the microscopic morphology of the two types of
craniopharyngioma were significantly different, their
ultrastructure was largely similar. In the present study, abundant
mitochondria were identified in the craniopharyngioma cells,
indicating active metabolism, and well-developed rough endoplasmic
reticulum and ribosomes were clearly visible, which is typical of
fully differentiated and actively functioning cells. Despite the
benign clinical manifestation and biological behavior of
craniopharyngioma observed in the present study, these features
appear to oppose the traditionally recognized benign nature of
craniopharyngioma. Furthermore, the ultrastructure of
craniopharyngioma appears to exhibit malignant potential. A high
ratio of euchromatin, a large number of nuclear pores and large
nucleoli were observed in the nucleus of the craniopharyngioma
cells, indicating a high level of protein synthesis. Therefore,
craniopharyngioma may not be benign as previously hypothesized. In
addition, electron microscopy identified that craniopharyngioma
features abundant tonofibrils and microvilli; the latter is
associated with the solidity and material transport, indicating
solidity of craniopharyngioma and active cell contraction,
including movement, cytoplasm flow, phagocytosis and excretion.
In 1997, survivin, a novel inhibitor of apoptosis,
was identified (26). A high level
of survivin expression was found in all common human malignancies
at the mRNA and protein levels. Hassounah et al (27) evaluated survivin expression levels
in various benign neurological tumors and the results indicated
that survivin expression may be an early event in tumorigenesis,
providing a favorable condition for the development of malignant or
benign tumors. In the present study, it was identified that
survivin protein is expressed at varying levels in
craniopharyngioma, however, it is not expressed in healthy brain
tissue. It is proposed that survivin expression levels in
craniopharyngioma may exhibit anti-apoptotic effects. In addition,
it was identified that survivin expression levels are significantly
different in different pathological types, genders and age groups,
and between recurrent and non-recurrent craniopharyngioma patients.
The present study provided novel data regarding survivin expression
levels in neurological benign tumors, highlighting the importance
of survivin in the occurrence and development of brain tumors. In
addition, survivin is expressed at higher levels in
adamantinomatous craniopharyngioma compared with squamous-papillary
craniopharyngioma, which may partially explain the higher
recurrence rate of the adamantinomatous tumor type. Furthermore, it
was identified that males have higher ratio of adamantinomatous to
squamous-papillary craniopharyngioma compared with females. Among
the adamantinomatous craniopharyngioma patients, survivin
expression levels were higher in the males compared with the
females, while male and female squamous-papillary craniopharyngioma
patients demonstrated no significant difference in survivin
expression. The higher proportion of male adamantinomatous
craniopharyngioma patients and the higher survivin expression
levels in male adamantinomatous craniopharyngioma patients may have
resulted in the typically high survivin expression levels observed
overall in males compared with females. The results of the present
study indicate that survivin may exhibit a stronger anti-apoptotic
affect in male patients compared with female patients, indicating a
higher invasiveness of craniopharyngioma in males, however,
additional clinical observation is required to clarify this
hypothesis. Furthermore, it was identified that survivin protein
expression levels are higher in recurrent craniopharyngioma cases
compared with non-recurrent cases, indicating that higher survivin
expression levels may inhibit apoptosis and promote tumor
recurrence.
In conclusion, the current study indicates that
survivin may regulate the cell cycle and apoptosis in the
tumorigenesis of craniopharyngioma. Survivin may significantly
inhibit the apoptosis of the tumor cells, thus increasing the
aggressiveness of benign tumors and the malignancy of malignant
tumors, as well as increasing the likelihood of tumor recurrence.
Therefore, survivin may be useful as a predictor of
craniopharyngioma patient prognosis, however, additional studies on
larger patient samples are required to confirm this
association.
References
|
1
|
Tena-Suck ML, Hernández-Campos ME,
Ortiz-Plata A, et al: Intracerebral injection of oil cyst content
of human craniopharyngioma (oil machinery fluid) as a toxic model
in the rat brain. Acta Histochem. 116:448–456. 2014. View Article : Google Scholar
|
|
2
|
Larkin SJ and Ansorge O: Pathology and
pathogenesis of craniopharyngiomas. Pituitary. 16:9–17. 2013.
View Article : Google Scholar
|
|
3
|
Fiorito CM, Giglione E, Bellone S, et al:
Craniopharyngioma in children: importance of a multidisciplinary
approach and therapeutic strategies in the treatment of relapsing.
Minerva Pediatr. 65:673–676. 2013.(In Italian). PubMed/NCBI
|
|
4
|
El-Gaidi MA: Descriptive epidemiology of
pediatric intracranial neoplasms in Egypt. Pediatr Neurosurg.
47:385–395. 2011. View Article : Google Scholar
|
|
5
|
Chakrabarty A, Mitchell P and Bridges LR:
Craniopharyngioma invading the nasal and paranasal spaces, and
presenting as nasal obstruction. Br J Neurosurg. 12:361–363. 1998.
View Article : Google Scholar
|
|
6
|
Bunin GR, Surawicz TS, Witman PA, et al:
The descriptive epidemiology of craniopharyngioma. J Neurosurg.
89:547–551. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ujifuku K, Matsuo T, Takeshita T, et al:
Malignant transformation of craniopharyngioma associated with
moyamoya syndrome. Neurol Med Chir (Tokyo). 50:599–603. 2010.
View Article : Google Scholar
|
|
8
|
Lauriola L, Doglietto F, Novello M, et al:
De novo malignant craniopharyngioma: case report and literature
review. J Neurooncol. 103:381–386. 2011. View Article : Google Scholar
|
|
9
|
Gao S, Shi X, Wang Y, Qian H and Liu C:
Malignant transformation of craniopharyngioma: case report and
review of the literature. J Neurooncol. 103:719–725. 2011.
View Article : Google Scholar
|
|
10
|
Rath SR, Lee S, Kotecha RS, et al:
Childhood craniopharyngioma: 20-year institutional experience in
Western Australia. J Paediatr Child Health. 49:403–408. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Van Effenterre R and Boch AL:
Craniopharyngioma in adults and children: a study of 122 surgical
cases. J Neurosurg. 97:3–11. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Müller HL: Childhood craniopharyngioma:
treatment strategies and outcomes. Expert Rev Neurother.
14:187–197. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hoffman HJ, De Silva M, Humphreys RP, et
al: Aggressive surgical management of craniopharyngiomas in
children. J Neurosurg. 76:47–52. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ogawa Y, Watanabe M and Tominaga T:
Rathke’s cleft cysts with significant squamous metaplasia - high
risk of postoperative deterioration and close origins to
craniopharyngioma. Acta Neurochir (Wien). 155:1069–1075. 2013.
View Article : Google Scholar
|
|
15
|
Yang I, Sughrue ME, Rutkowski MJ, et al:
Craniopharyngioma: a comparison of tumor control with various
treatment strategies. Neurosurg Focus. 28:E52010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Janzer RC, Burger PC, Giangaspero F and
Paulus W: Craniopharyngioma. World Health Organization
Classification of Tumours of the Central Nervous System. Kleihues P
and Cavenee WK: IARC Press; Lyon: pp. 244–246. 2000
|
|
17
|
Carmel PW, Antunes JL and Chang CH:
Craniopharyngiomas in children. Neurosurgery. 11:382–389. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Goodrich JT, Post KD and Duffy P: Ciliated
craniopharyngioma. Surg Neurol. 24:105–111. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Garcia-Lavandeira M, Saez C,
Diaz-Rodriguez E, et al: Craniopharyngiomas express embryonic stem
cell markers (SOX2, OCT4, KLF4, and SOX9) as pituitary stem cells
but do not coexpress RET/GFRA3 receptors. J Clin Endocrinol Metab.
97:E80–E87. 2012. View Article : Google Scholar
|
|
20
|
Barkhoudarian G and Laws ER:
Craniopharyngioma: history. Pituitary. 16:1–8. 2013. View Article : Google Scholar
|
|
21
|
Sato K, Oka H, Utsuki S, et al: Ciliated
craniopharyngioma may arise from Rathke cleft cyst. Clin
Neuropathol. 25:25–28. 2006.PubMed/NCBI
|
|
22
|
Zoicas F and Schöfl C: Craniopharyngioma
in adults. Front Endocrinol (Lausanne). 3:462012.
|
|
23
|
Tavangar SM, Larijani B, Mahta A, et al:
Craniopharyngioma: a clinicopathological study of 141 cases. Endocr
Pathol. 15:339–344. 2004. View Article : Google Scholar
|
|
24
|
Crotty TB, Scheithauer BW, Young WF Jr, et
al: Papillary craniopharyngioma: a clinicopathological study of 48
cases. J Neurosurg. 83:206–214. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kawano N, Oka H, Suwa T, et al: Origin of
craniopharyngioma: an electron microscopic study. Noshuyo Byori.
10:117–123. 1993.PubMed/NCBI
|
|
26
|
Ambrosini G, Adida C and Altieri DC: A
novel anti-apoptosis gene, survivin, expressed in cancer and
lymphoma. Nat Med. 3:917–921. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hassounah M, Lach B, Allam A, et al:
Benign tumors from the human nervous system express high levels of
survivin and are resistant to spontaneous and radiation-induced
apoptosis. J Neurooncol. 72:203–208. 2005. View Article : Google Scholar : PubMed/NCBI
|