Introduction
The majority of thyroid cancers (90%) are
differentiated thyroid cancers (DTC), a term which includes both
papillary and follicular cancer (1). Thyroid carcinoma accounts for ~1% of
all new malignant disease and ~0.5 and 1.5% of cancers in males and
females, respectively (2). DTC
progression is generally slow, with a low grade malignancy and
excellent long-term survival rates. The overall 10-year survival
rate of DTC is >90% (3). Among
DTC, the incidence of papillary thyroid cancer (PTC) was 7.9 per
100,000 individuals, the mortality rate was ~0.4 per 100,000
individuals and the overall survival rate was 98.3% (4,5).
Patients with DTC respond to total thyroidectomy, radioiodine
ablation and levothyroxine suppression therapy. Distant metastases
occur during follow-up in 2.2–23% of patients (6–8), and
are usually identified in the lung and bone. Less frequently, they
are detected in the brain, liver or other sites, and indicate a
significantly poorer prognosis (9,10).
However, metastasis to the skeletal muscles from PTC is extremely
rare, particularly synchronous lung and skeletal muscle metastases
(11,12). The present study reports the case of
a 31-year-old male with PTC and concurrent metastasis to the left
gastrocnemius muscle and lungs. Written informed consent was
obtained from the patient.
Case report
In May 2007, a 31-year-old Chinese male presented to
the Department of Surgical Oncology with palpable nodules of the
thyroid in May 2007. An ultrasound (US) of the patient’s neck
revealed hypoechoic multinodules with microcalcification in the
bilateral thyroid, the largest of which was located in the left
lobe (~3.0 cm). Cervical lymph node enlargement was also observed
with microcalcification. Thyroid function tests indicated a
euthyroid state. The patient had no family history of thyroid
disease and denied any exposure to external or accidental
radiation. Serum thyroglobulin (Tg) level was measured at 82.2
ng/ml (normal range, <55 ng/ml), with negative anti-Tg
antibodies (TgAb). Following total thyroidectomy and central
cervical node dissection, the patient was diagnosed with
laryngotracheal invasion from PTC (pathological stage T4a N1a
M1pul, 2010 AJCC) (13). The
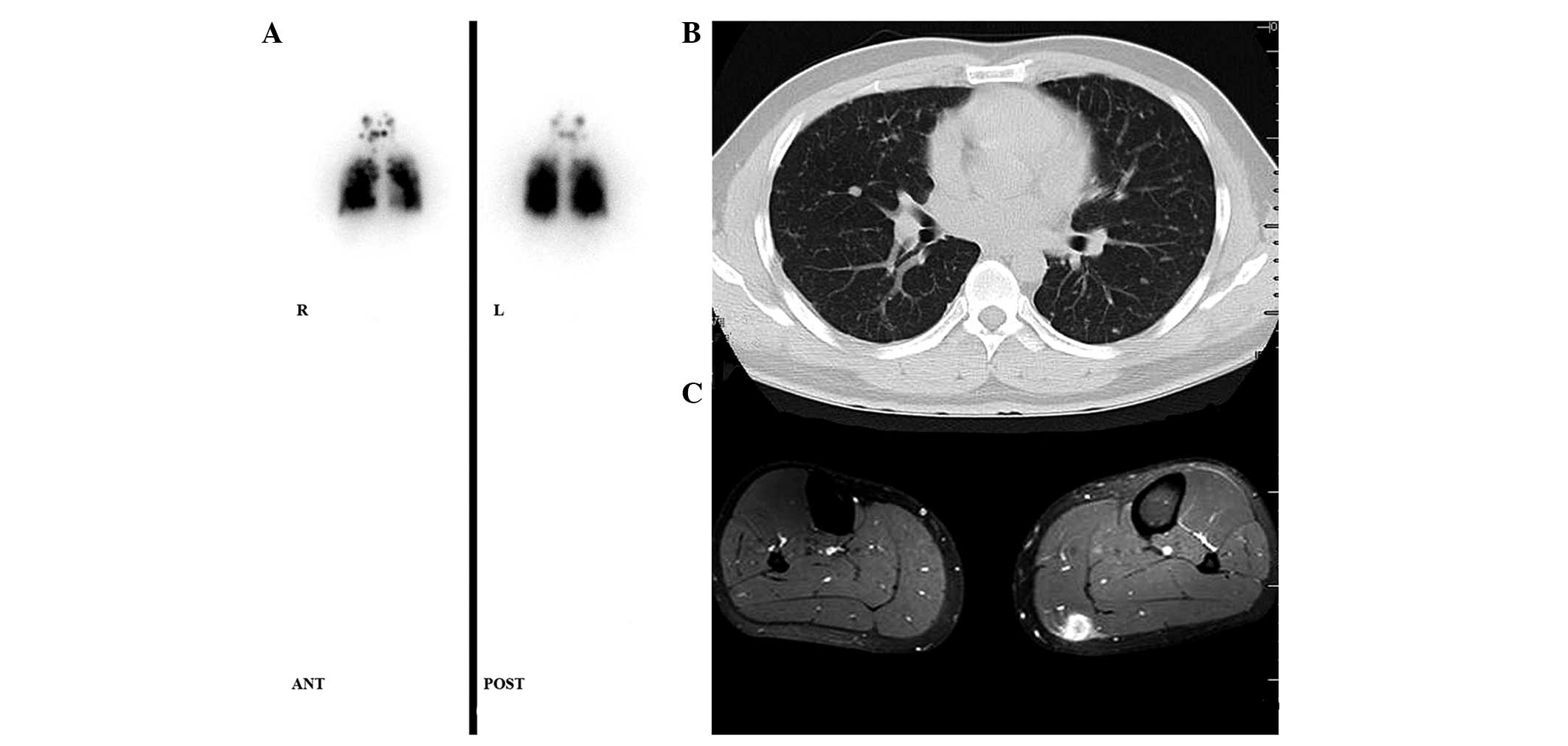
patient subsequently received radioiodine treatment four times
(total dose, 24050 MBq). A whole body scan (WBS) revealed
131Iodine uptake in the lung (Fig. 1A), consistent with visible lesions
on a computed tomography (CT) scan (Fig. 1B), which indicated pulmonary
metastases.
The patient was referred to the First Affiliated
Hospital (Hangzhou, China) in July 2013, with a three-month history
of a slowly increasing mass in the left gastrocnemius muscle. On
physical examination, the patient’s vital signs were stable, and a
soft mass of ~1.5 cm in size was palpable in the left leg with no
inflammatory surface. Serum Tg level was 80.2 ng/ml (normal range,
<1 ng/ml). However, TgAb level was not available during this
time. The results of tests for other biochemical tumor markers,
including α-fetoprotein (2.8 ng/ml; normal range, <20.0 ng/ml),
carcino-embryonic antigen (1.9 ng/ml; normal range, <5.0 ng/ml),
sugar antigen 199 (4.2 U/ml; normal range, <37 U/ml), sugar
antigen 125 (13.0 U/ml; normal range, <35 U/ml) and total
prostate specific antigen (2.103 ng/ml; normal range, <4.0
ng/ml), were within normal limits. Magnetic resonance imaging (MRI)
revealed a soft-tissue mass that was markedly low in signal
intensity on T1-weighted images, and enhanced after administration
of contrast material (Fig. 1C).
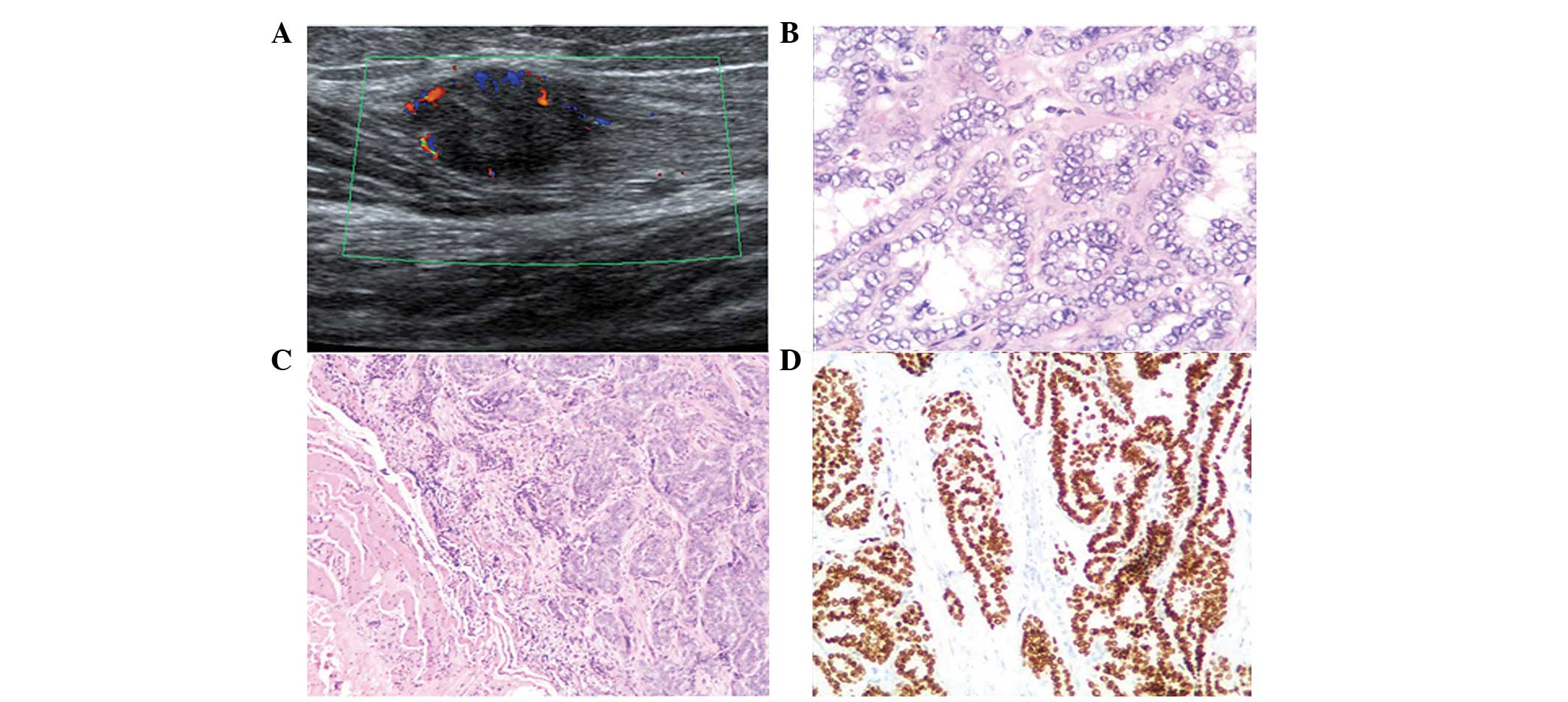
Doppler US showed a 1.7×1.2×1.5 cm solitary, hypoechoic nodule with
peripheral hypervascularity (Fig.
2A). A diagnosis of neurogenic tumor was highly suspected due
to the morphological features of the mass. A local marginal
resection was subsequently performed. Histopathology revealed the
mass to be a metastatic papillary tumor (Fig. 2B and C), and immunohistochemical
examination showed that the cells were positive for thyroid
transcription factor-1 (TTF-1) (Fig.
2D), indicating gastrocnemius muscle metastasis from PTC.
Concurrently, CT imaging of the chest revealed innumerable,
moderately well-circumscribed nodules in the lung with high
131Iodine uptake, indicating tumor metastases. After
surgery, the patient was treated with 131Iodine (6660
MBq). The patient’s Tg levels decreased to 40.6 ng/ml (normal
range, <1 ng/ml) and pulmonary metastases were stable after six
months of follow-up.
Discussion
Papillary thyroid cancer is commonly associated with
lymphatic spread to regional lymph nodes. Distant metastases occur
more rarely, usually involving the lungs and bone (1–7% of
patients) (14), but occasionally
occurs in the brain, sphenoid sinus, orbit, adrenal, kidney and
ovary (15–18). A retrospective review of the
literature revealed only two case reports of muscle metastases
arising from PTC (11,12). It has been hypothesized that
skeletal muscle is a hostile environment for proliferating cancer
cells, due to muscle motion and unadapted muscle pH (19), which may explain the lack of such
cases. Synchronous lung and skeletal muscle disease from PTC is an
extremely rare manifestation (18).
To the best of our knowledge, only two cases have been previously
reported (Table I). Bruglia et
al (11) reported the case of a
44-year-old male with PTC, with a poorly differentiated thyroid
carcinoma component and metastases to the thigh muscle, skin, lung,
mediastinum and brain. The aggressiveness of the tumor led to
mortality eight years following total thyroidectomy. Luo et
al (12) reported the case of a
29-year-old male patient who had unusual metastasis sites in the
lung, kidney and erector spinae from PTC. The authors concluded
that suspected tumors must be considered as potential metastases
from thyroid carcinomas in the clinical setting. The current study
reports a rare case of PTC associated with diffuse metastases to
the lung and gastrocnemius muscle, six years following total
thyroidectomy and radioiodine treatment.
 | Table ISynchronous lung and skeletal muscle
metastases from PTC reported previously in the literature. |
Table I
Synchronous lung and skeletal muscle
metastases from PTC reported previously in the literature.
| Author | Age, y/gender | Histology | TNM classification
after operation | Extrathyroid
extension | Site of
metastasis | Survival after
diagnosis of metastasis |
|---|
| Bruglia et al
(11) | 44/male | PTC | T3N1bM0 | Yes | Biceps femoris, lung,
skin, brain | 7 years |
| Luo et al
(12) | 29/male | PTC | TXN1M1 | NA | Erector spinae, lung,
kidney | - |
| Present case | 31/male | PTC | T4N1aM1 | Yes | Gastrocnemius muscle,
lung | Alive |
The particularly good prognosis and long-term
survival of PTC patients are significantly reduced in those with
distant metastasis (DM). The early differential diagnosis of
distant metastases of thyroid carcinoma remains difficult using
common diagnostic modalities such as US, Tg levels and
131I-WBS. Although postoperative serum Tg levels and
131I-WBS scans are sensitive methods in the detection of
metastatic disease, accurately localizing the source of the
abnormalities can be problematic, particularly in soft tissues. In
addition, radioiodine-negative thyroid cancer may account for ≤20%
of cases of DTC, which presents challenges in the localization of
metastatic lesions, even if the serum Tg level is evaluated
(20). Other imaging modalities,
including MRI and 2-deoxy-2-(18F)fluoro-D-glucose
(18FDG)-positron emission tomography (PET), may also be
valuable in the follow-up of thyroid cancer metastases,
particularly in patients with elevated Tg levels and normal
radioiodine WBS (21).
Various factors may contribute to the development of
DM, including large and multifocal primary tumors, extrathyroidal
extension, aggressive histology and advanced age (>45 years)
(22). Due to the rarity of
synchronous lung and skeletal muscle metastasis of PTC,
characteristic risk factors have not yet been identified. In the
present case, postoperative pathology revealed that DTC had invaded
the laryngotracheal region. Microscopic or gross invasion of the
tumor into the perithyroid, aggressive histology or vascular
invasion may be associated with an intermediate-high risk of
recurrence (23). Mortality is
increased in patients with distant metastases, particularly in
those aged >45 years (6).
Notably, the patient in the present study was only 37 years of age,
and remains alive six years following total thyroidectomy and
radioiodine treatment, which may support this observation.
In conclusion, this study presents a rare case of
synchronous skeletal muscle and lung metastasis from PTC. We
propose that Tg measurement, WBS and other imaging modalities,
including US, MRI and 18FDG-PET, must be utilized during
follow-up of patients with PTC, to detect possible uncommon distant
metastases, particularly in cases of PTC that exhibit aggressive
pathological behavior.
References
|
1
|
Sherman SI: Thyroid carcinoma. Lancet.
361:501–511. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Figge J: Epidemiology of thyroid cancer.
Thyroid Cancer: A Comprehensive Guide to Clinical Management.
Wartofsky L: Humana Press; Totowa, NJ: pp. 77–83. 1999
|
|
3
|
Gilliland FD, Hunt WC, Morris DM and Key
CR: Prognostic factors for thyroid carcinoma: A population-based
study of 15,698 cases from the Surveillance, Epidemiology and End
Results (SEER) program 1973–1991. Cancer. 79:564–573. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chen AY, Jemal A and Ward EM: Increasing
incidence of differentiated thyroid cancer in the United States,
1988–2005. Cancer. 115:3801–3807. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Albores-Saavedra J, Henson DE, Glazer E
and Schwartz AM: Changing patterns in the incidence and survival of
thyroid cancer with follicular phenotype - papillary, follicular,
and anaplastic: a morphological and epidemiological study. Endocr
Pathol. 18:1–7. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nixon IJ, Whitcher MM, Palmer FL, et al:
The impact of distant metastases at presentation on prognosis in
patients with differentiated carcinoma of the thyroid gland.
Thyroid. 22:884–889. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mihailovic J, Stefanovic L and Malesevic
M: Differentiated thyroid carcinoma with distant metastases:
probability of survival and its predicting factors. Cancer Biother
Radiopharm. 22:250–255. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Goffredo P, Sosa JA and Roman SA:
Differentiated thyroid cancer presenting with distant metastases: a
population analysis over two decades. World J Surg. 37:1599–1605.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lin JD, Chao TC, Chou SC and Hsueh C:
Papillary thyroid carcinomas with lung metastases. Thyroid.
14:1091–1096. 2004. View Article : Google Scholar
|
|
10
|
Pittas AG, Adler M, Fazzari M, Tickoo S,
Rosai J, Larson SM and Robbins RJ: Bone metastases from thyroid
carcinoma: clinical characteristics and prognostic variables in one
hundred forty-six patients. Thyroid. 10:261–268. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bruglia M, Palmonella G, Silvetti F, et
al: Skin and thigh muscle metastasis from papillary thyroid cancer.
Singapore Med J. 50:e61–e64. 2009.PubMed/NCBI
|
|
12
|
Luo Q, Luo QY, Sheng SW, et al:
Localization of concomitant metastases to kidney and erector spinae
from papillary thyroid carcinoma using (131)I-SPECT and CT.
Thyroid. 18:663–664. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
NCCN guidelines: Thyroid carcinoma.
Version 3. 2011
|
|
14
|
Tahmasebi FC, Farmer P, Powell SZ, et al:
Brain metastases from papillary thyroid carcinomas. Virchows Arch.
462:473–480. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liou MJ, Lin JD, Chung MH, Liau CT and
Hsueh C: Renal metastasis from papillary thyroid microcarcinoma.
Acta Otolaryngol. 125:438–442. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brogioni S, Viacava P, Tomisti L, et al: A
special case of bilateral ovarian metastases in a woman with
papillary carcinoma of the thyroid. Exp Clin Endocrinol Diabetes.
115:397–400. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rocha Filho FD, Lima GG, Ferreira FV, Lima
MG and Hissa MN: Orbital metastasis as primary clinical
manifestation of thyroid carcinoma - case report and literature
review. Arq Bras Endocrinol Metabol. 52:1497–1500. 2008. View Article : Google Scholar
|
|
18
|
Argibay Vázquez S, Lancha Hernández C and
Martínez Muñiz A: Metastases in the sphenoidal sinus in a patient
with papillary thyroid cancer. Clin Transl Oncol. 7:324–327. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Seely S: Possible reasons for high
resistance of muscle to cancer. Med Hypotheses. 6:133–137. 1980.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bae SY, Lee SK, Koo MY, et al: Distant,
solitary skeletal muscle metastasis in recurrent papillary thyroid
carcinoma. Thyroid. 21:1027–1031. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dong MJ, Liu ZF, Zhao K, et al: Value of
18F-FDG-PET/PET-CT in differentiated thyroid carcinoma with
radioiodine-negative whole-body scan: a meta-analysis. Nucl Med
Commun. 30:639–650. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Toubert ME, Hindie E, Rampin L, Al-Nahhas
A and Rubello D: Distant metastases of differentiated thyroid
cancer: diagnosis, treatment and outcome. Nucl Med Rev Cent East
Eur. 10:106–109. 2007.
|
|
23
|
American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid
Cancer. Cooper DS, Doherty GM, Haugen BR, et al: Revised American
Thyroid Association management guidelines for patients with thyroid
nodules and differentiated thyroid cancer. Thyroid. 19:1167–1214.
2009. View Article : Google Scholar : PubMed/NCBI
|