Introduction
The majority of cases of intussusception occur in
infants and children, although ~5% of affected patients are adults
(1). Intussusception is the
invagination of a segment of bowel into the distal adjacent bowel
(2). Occurrence in the colon in
adults is rare and often originates from a malignant neoplasm
(3). Intussusception poses a
significant challenge due to the variety of symptoms that they may
present with, the diagnostic difficulties of radiological
confirmation and the management of the condition.
Signet ring cell carcinoma of the colon is a rare
histological subtype and accounts for 0.5–1% of all colon
adenocarcinomas. The neoplasm is characterized by a specific
morphological appearance of abundant intracytoplasmic mucin, which
pushes the nucleus to the periphery of the cell to give a signet
ring appearance (4,5). As the clinical symptoms tend to be
delayed, the majority of cases of signet ring cell carcinoma are
often detected at an advanced stage.
In the present study, a young male with adult
intussusception of the descending colon, caused by signet ring cell
carcinoma, was pre-operatively diagnosed by a computed tomography
(CT) scan. Written informed consent was obtained from the
patient.
Case report
A 27-year-old male who had experienced intermittent
left upper-quadrant abdominal pain without hematochezia for more
than six months was admitted to the Kunshan First People’s Hospital
Affiliated to Jiangsu University (Kunshan, China). The patient did
not complain of any other symptoms, such as vomiting, nausea or
fever, had no relevant medical or surgical history, and denied
smoking and alcohol consumption. A physical examination identified
left upper quadrant tenderness, but no rebound tenderness. Upon
palpation, no abdominal mass was identified and laboratory test
results were all within normal ranges. The chest X-ray, plain
abdominal X-ray and electrocardiography findings were non-specific.
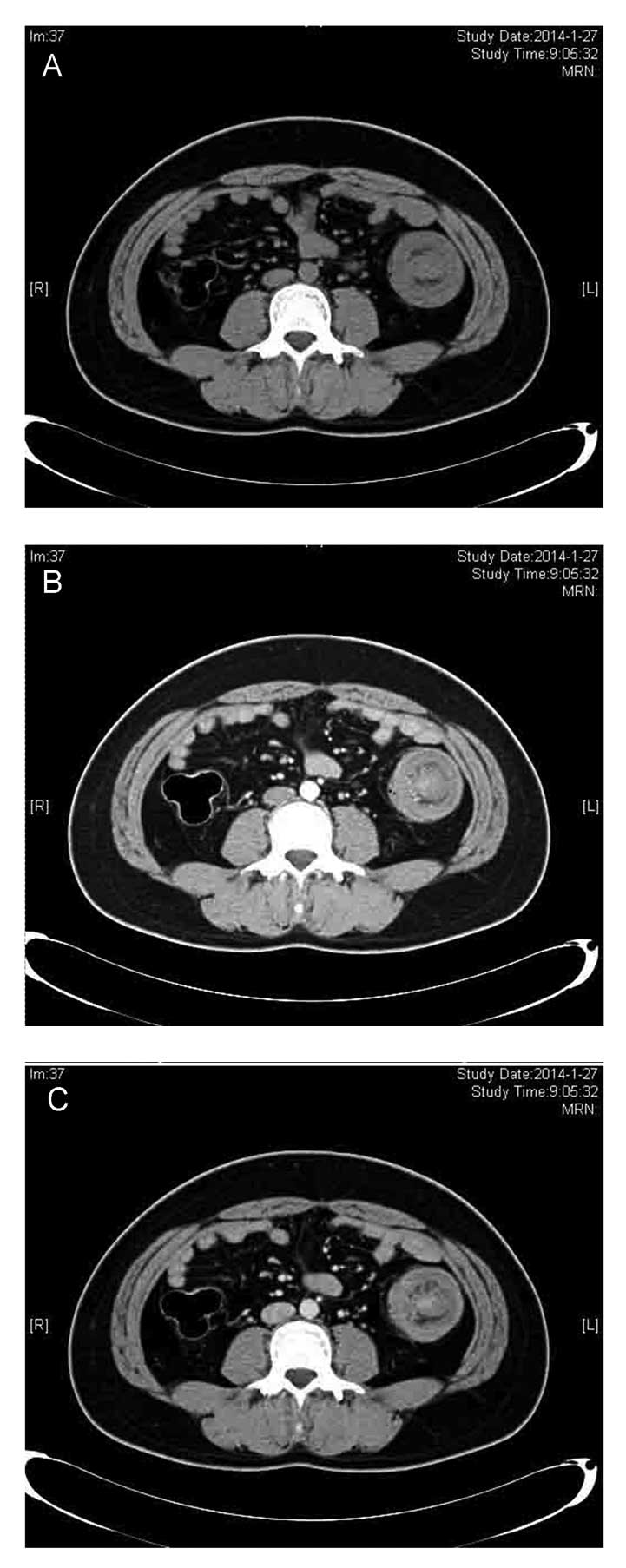
A CT scan showed the concentric-like structure of the descending
colon, which was typical of left colonic intussusception, but no
evidence of ischemic changes in the proximal colon were revealed
(Fig. 1).
Upon examination, there was no evidence of
intestinal obstruction. Elective surgery with a median laparotomy
was performed, which confirmed the diagnosis of intestinal
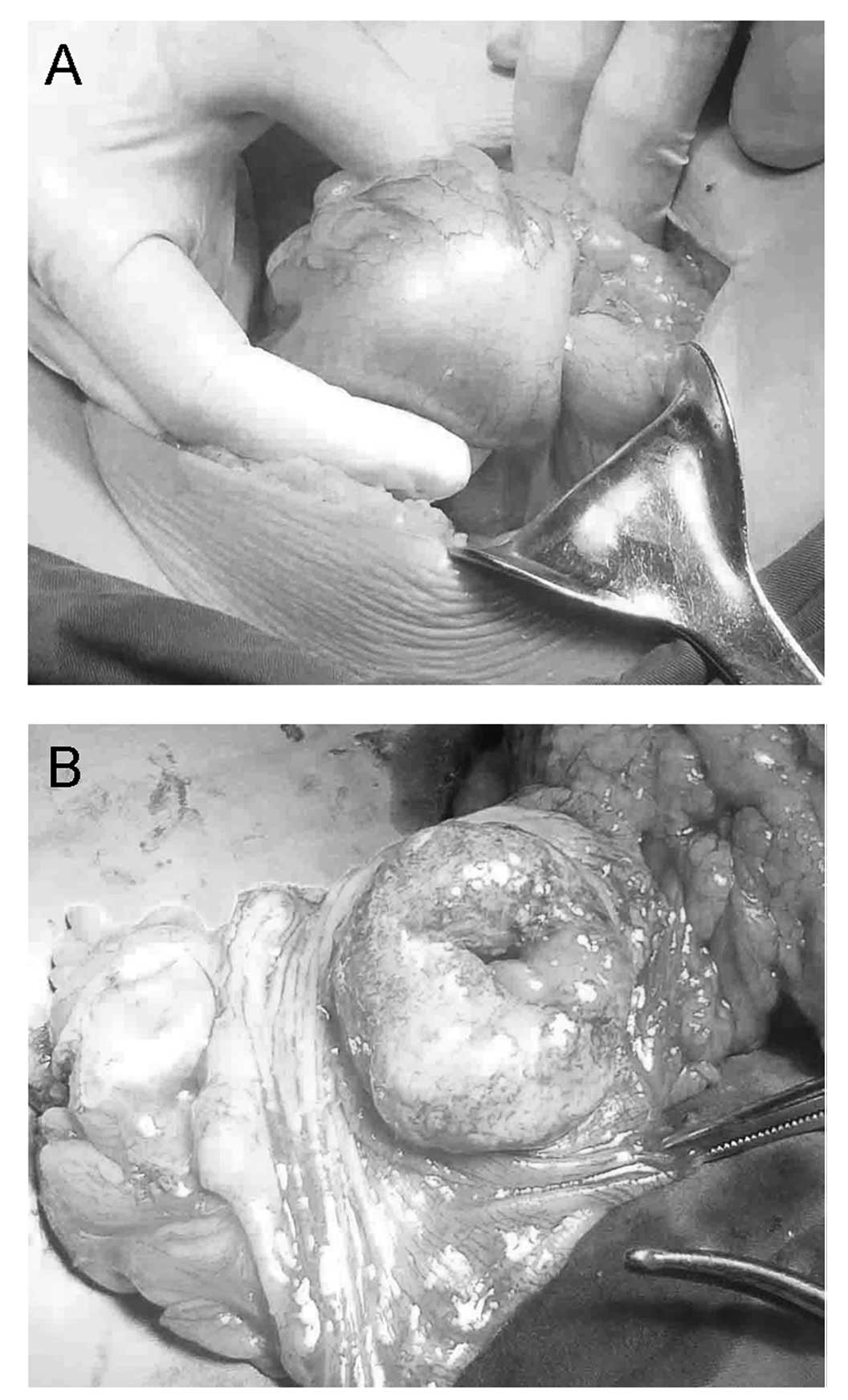
intussusception caused by a left colon carcinoma. Surgery revealed
that the tumor had caused the descending colon to intussuscept into
itself (Fig. 2A). To prevent the
neoplastic spread of the malignant tumor, manual disinvagination to
save the intestinal segments was not attempted. Instead, a left
hemicolectomy, which extended to the left region of the transverse
colon and a section of the sigmoid colon, was performed (Fig. 2B). Intestinal continuity was
restored with an end-to-side anastomosis between the transverse
colon and sigmoid colon. The histology report demonstrated a signet
ring cell carcinoma, which was classified as pT4aN2M0, according to
the American Joint Committee on Cancer TNM classification of
malignant tumors (6). The
post-operative course was uneventful and the patient was discharged
on the tenth post-operative day.
Discussion
Intussusception is the telescoping of the proximal
intestinal wall into the lumen of a distal intestinal segment
(2,7–9).
Whilst common in young patients, intussusception is rare in adults
and is primarily precipitated by a malignant neoplasm.
Intussusceptions have been classified into four categories
according to location, as follows: i) Entero-enteric, ii)
colo-colonic, iii) ileo-colonic and iv) ileo-cecal (10). Colo-colonic intussusceptions are
often located in the sigmoid colon or cecum (11). Intussusceptions of the descending
colon are more uncommon due to the anatomical attachment of the
descending colon to the retroperitoneum (12).
The first described case of primary signet ring cell
carcinoma of the colon and rectum was in 1951 (13). This particular type of neoplasm
accounts for <1% of all reported adenocarcinomas and most
frequently presents in young children. Furthermore, regardless of
tumor location, signet ring histology is associated with a more
advanced stage and higher tumor grade upon presentation, and a
poorer clinical outcome compared with other subtypes of
adenocarcinoma (4,14).
In the present study, a rare case of descending
colo-colonic intussusception caused by a primary signet ring cell
carcinoma of the colon was described. Unlike cases of childhood
intussusception, no attempt should be made to reduce a colonic
intussusception in adults by a barium enema; adult intussusception
is often accompanied with organic diseases and, in this case,
barium enema is ineffective in reduction (15,16).
The reduction of intussusceptions with suspected malignancy is
generally not advisable due to the possibility of bowel perforation
and tumor cell dissemination. The primary treatment approach for
intussusceptions is surgery (17).
For lesions of the descending colon, resection of the left half of
the transverse descending and sigmoid colon should be performed
alongside anastomosis of the proximal transverse colon to the
rectosigmoid. The performance of an anastomosis with or without
proximal decompression depends upon the judgment and skill of the
surgeon, and the condition of the bowel.
In the present case, one month followng surgery, the
patient received six cycles of standardized chemotherapy, with each
cycle lasting for four weeks, at the Department of Oncology,
Kunshan First People’s Hospital Affiliated to Jiangsu University.
The latest CT scan, three months after the cyclo of chemotherapy,
did not show any recurrence. In a previous study, a total of 60% of
colonic intussusceptions were caused by malignant neoplasms, in
patients with colonic intussusceptions (18). It may be difficult to distinguish
between colonic intussusceptions that harbour a benign or a
malignant lesion. Therefore, we propose that in colonic
intussusceptions, colonoscopy is a necessary preoperative
procedure.
References
|
1
|
Gollub MJ: Colonic intussusception:
clinical and radiographic features. AJR Am J Roentgenol.
196:W580–W585. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gupta RK, Agrawal CS, Yadav R, et al:
Intussusception in adults: institutional review. Int J Surg.
9:91–95. 2011. View Article : Google Scholar
|
|
3
|
Xu XQ, Hong T, Liu W, et al: A long adult
intussusception secondary to transverse colon cancer. World J
Gastroenterol. 19:3517–3519. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hyngstrom JR, Hu CY, Xing Y, et al:
Clinicopathology and outcomes for mucinous and signet ring
colorectal adenocarcinoma: analysis from the National Cancer Data
Base. Ann Surg Oncol. 19:2814–2821. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Thota R, Fang X and Subbiah S:
Clinicopathological features and survival outcomes of primary
signet ring cell and mucinous adenocarcinoma of colon:
retrospective analysis of VACCR database. J Gastrointest Oncol.
5:18–24. 2014.PubMed/NCBI
|
|
6
|
Shia J, Klimstra DS, Bagci P, et al: TNM
staging of colorectal carcinoma: issues and caveats. Semin Diagn
Pathol. 29:142–153. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Howard N, Pranesh N and Carter P:
Colo-colonic intusussception secondary to a lipoma. Int J Surg Case
Rep. 3:52–54. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Abbes Orabi N, Paterson HM and Kartheuser
A: Adult colo-colonic intussusception. Tech Coloproctol. 14:95–96.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yakan S, Calkiskan C, Makay O, et al:
Intussusception in adults: clinical characteristics, diagnosis and
operative strategies. World J Gastroenterol. 15:1985–1989. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Amoruso M, D’Abbicco D, Praino S, et al:
Idiopathic adult colo-colonic intussusception: case report and
review of the literature. Int J Surg Case Rep. 4:416–418. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang L, Chen P, Zong L, et al: Colon
angiolipoma with intussusception: a case report and literature
review. World J Surg Oncol. 11:692013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fukuchi M, Tsukagoshi R, Sakurai S, et al:
Adult intussusception caused by descending colon cancer during
chemotherapy of stomach cancer recurrence. Case Rep Gastroenterol.
6:88–93. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Laufman H and Saphir O: Primary linitis
plastica type of carcinoma of the colon. AMA Arch Surg. 62:79–91.
1951. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim JH, Park SJ, Park MI, et al:
Early-stage primary signet ring cell carcinoma of the colon. World
J Gastroenterol. 19:3895–3898. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sanders GB, Hagan WH and Kinnaird DW:
Adult intussusception and carcinoma of the colon. Ann Surg.
147:796–804. 1958.PubMed/NCBI
|
|
16
|
Azar T and Berger DL: Adult
intussusception. Ann Surg. 226:134–138. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Marinis A, Yiallourou A, Samanides L, et
al: Intussusception of the bowel in adults: a review. World J
Gastroenterol. 15:407–411. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Goh BK, Quah HM, Chow PK, et al:
Predictive factors of malignancy in adults with intussusception.
World J Surg. 30:1300–1304. 2006. View Article : Google Scholar : PubMed/NCBI
|