Introduction
Brain metastases are common intracranial
malignancies, occurring in 15–40% of adult cancer patients. Only
3–5% of all brain metastases are located in the brainstem. The
primary tumor with the highest rate of brainstem involvement is
lung cancer, followed by breast cancer, ovarian cancer, colorectal
cancer, renal cell carcinoma and melanoma. Brainstem metastases
have a poor prognosis and are particularly challenging to manage;
clinical reviews of patients treated for brainstem metastases have
reported median survival times ranging from 1–11 months (1–12).
Surgical resection is rarely a viable option due to the high risk
of developing new neurological deficits or worsening of existing
deficits as the majority of drugs which penetrate the blood brain
barrier have been found to exhibit low efficacy in this context
(5–7). Chemotherapy is also of limited use in
brainstem metastases. Stereotactic radiosurgery (SRS) procedures,
including gamma knife radiosurgery (GKRS) and linear accelerator
(LINAC), have proven to be effective treatment modalities for
brainstem metastases (2–21). To the best of our knowledge, the
current study reports the first patient with
histopathologically-confirmed brainstem metastasis originating from
lung adenosquamous carcinoma, and discusses the outcome of
stereotactic aspiration and GKRS. Written informed consent was
obtained from the patient’s family.
Case report
A 59-year-old Chinese female presented to the
Department of Neurosurgery, The Affiliated Hospital of Beihua
University (Jilin, China) with a two-week history of vertigo and
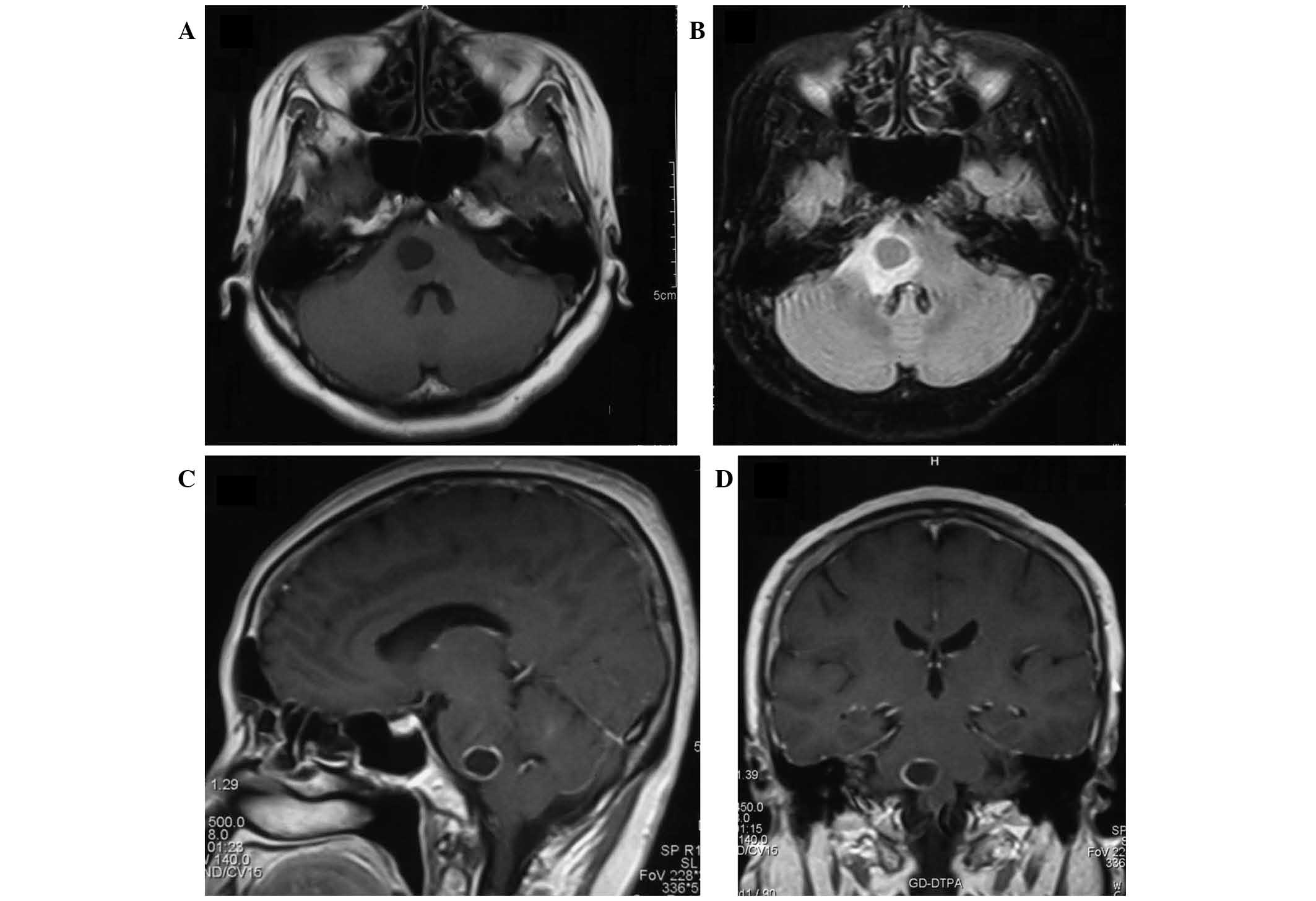
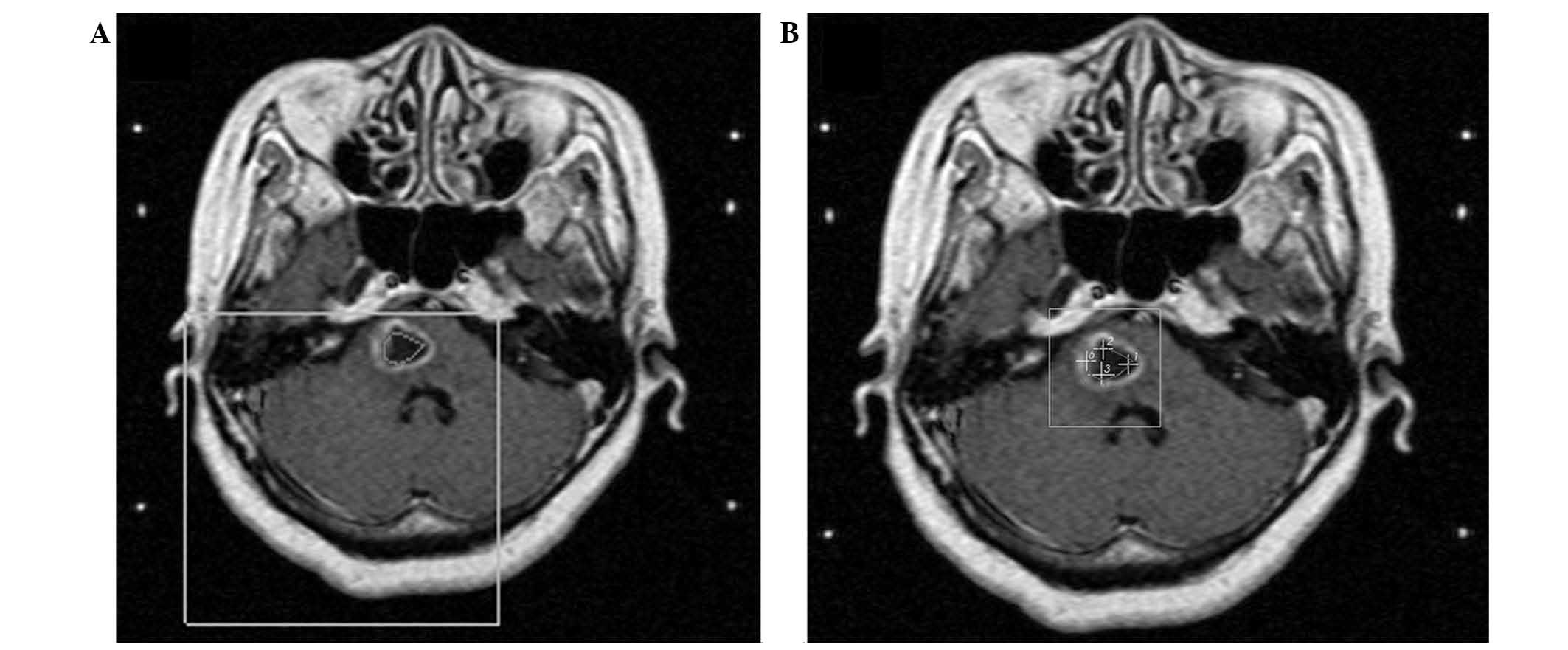
gait instability on May 19, 2012. Magnetic resonance imaging (MRI)
revealed a cystic mass located in the pons. The cystic brainstem
tumor initially measured 15×12×13 mm (volume, 1.3 cm3),
and the cyst wall exhibited annular enhancement (Fig. 1). The patient had undergone surgical
treatment for primary lung cancer, pathologically diagnosed as
adenosquamous carcinoma, at Jilin Province Cancer Hospital
(Changchun, China) two years prior to the current presentation.
Brainstem metastases were diagnosed based on the clinical and
neuroimaging findings, and the patient received initial GKRS for
the lesion in the pons over 40 days. The total radiosurgical dose
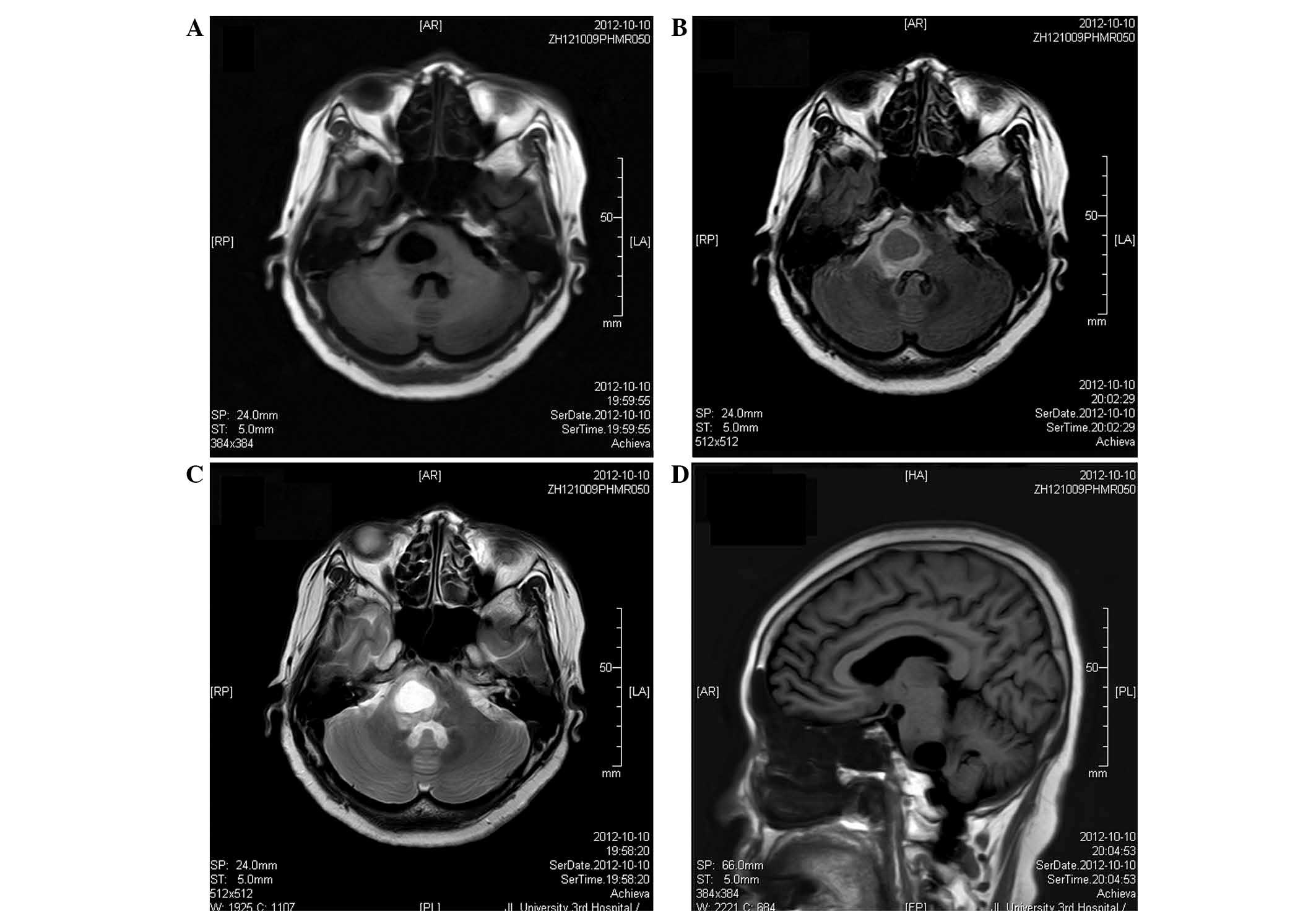
applied to the tumor was 54.0 Gy in 2 Gy daily fractions. MRI,
three months following the completion of GKRS, revealed that the
cystic mass had increased in size to 22×17×19 mm (volume, 3.9
cm3) (Fig. 2). The
patient was subsequently referred to the Department of
Neurosurgery, China-Japan Union Hospital of Jilin University
(Changchun, China) for further treatment.
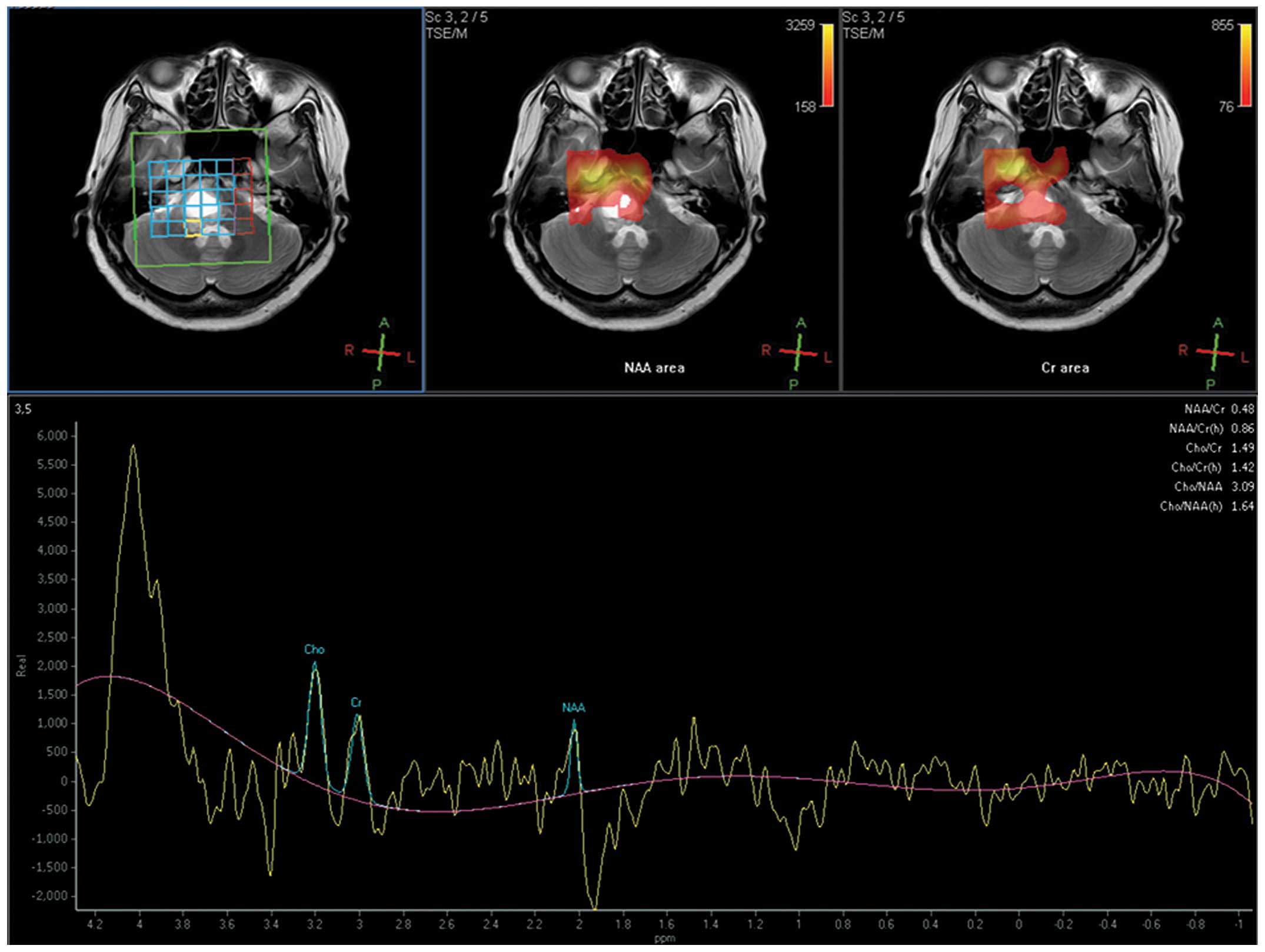
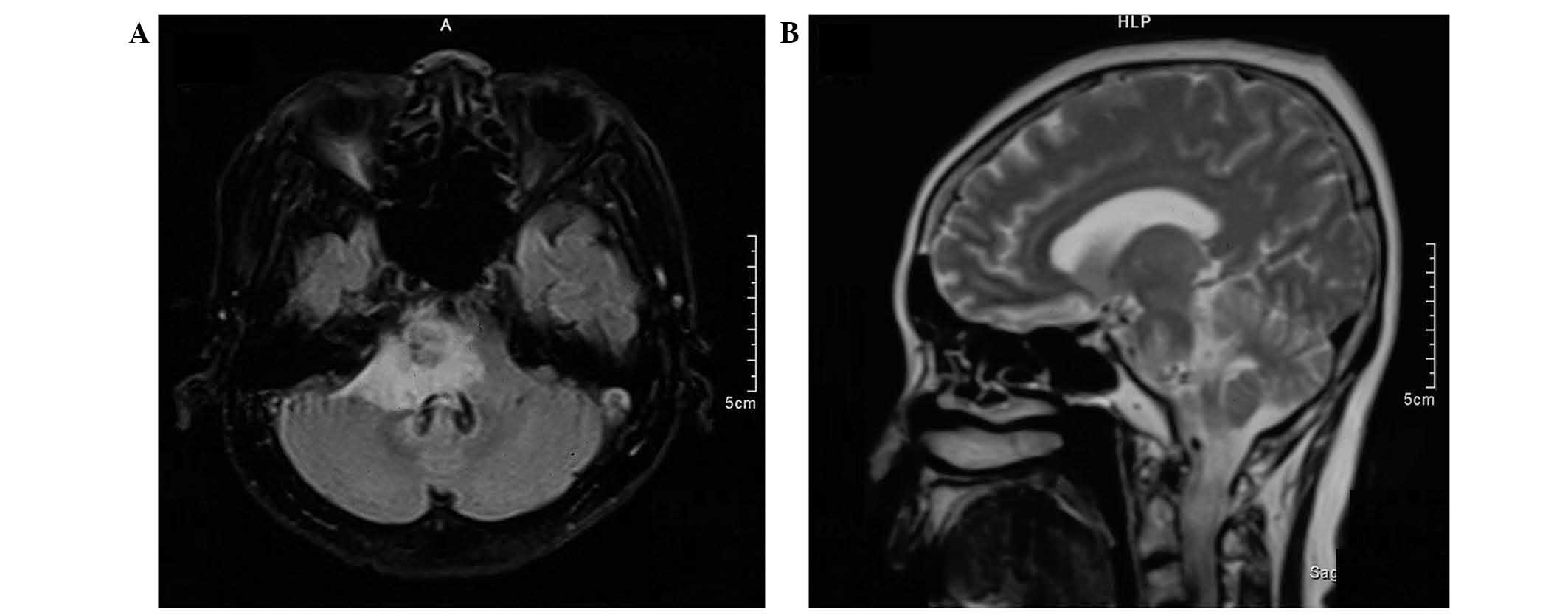
Upon admission, magnetic resonance spectroscopy
(MRS) with peritumoral measurements revealed that the
choline/N-acetylaspartate (Cho/NAA) ratio was 3.09 (Fig. 3). Computed tomography-guided
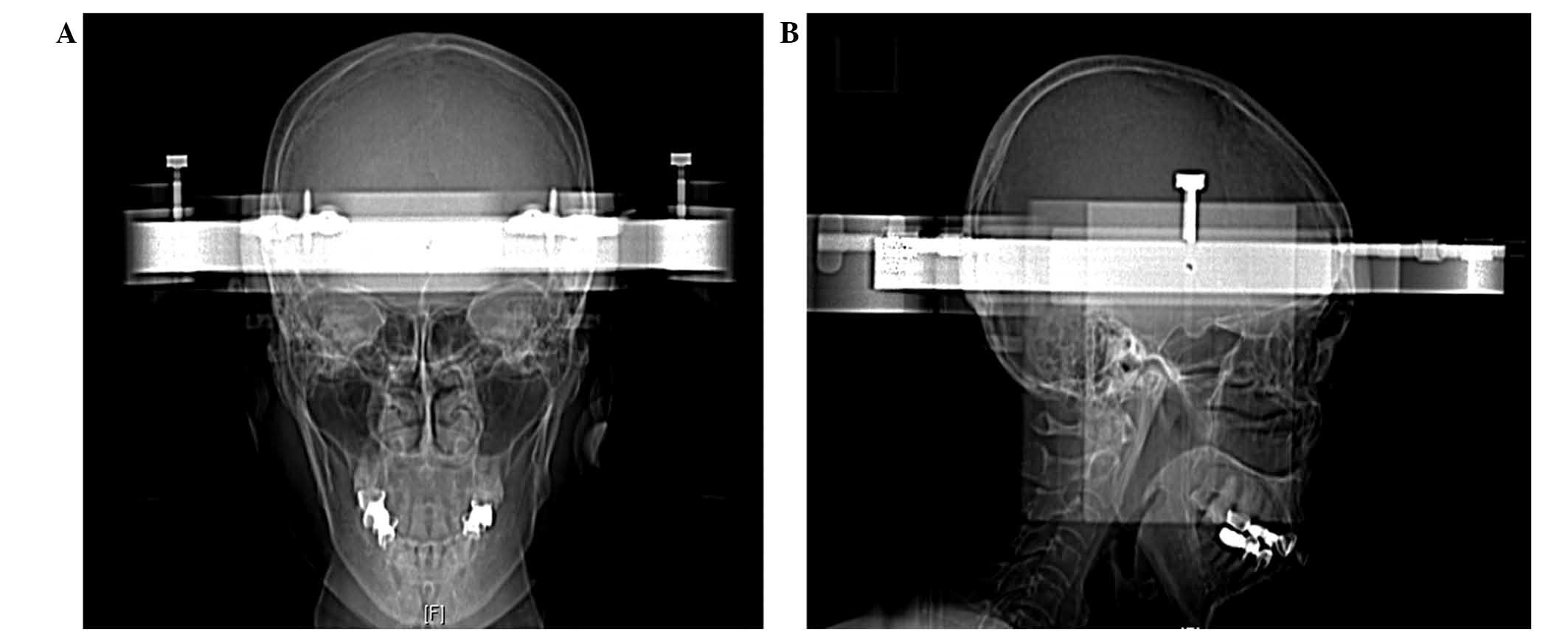
stereotactic biopsy and aspiration of the intratumoral cyst,
performed three months following the initial GKRS, yielded 2.0
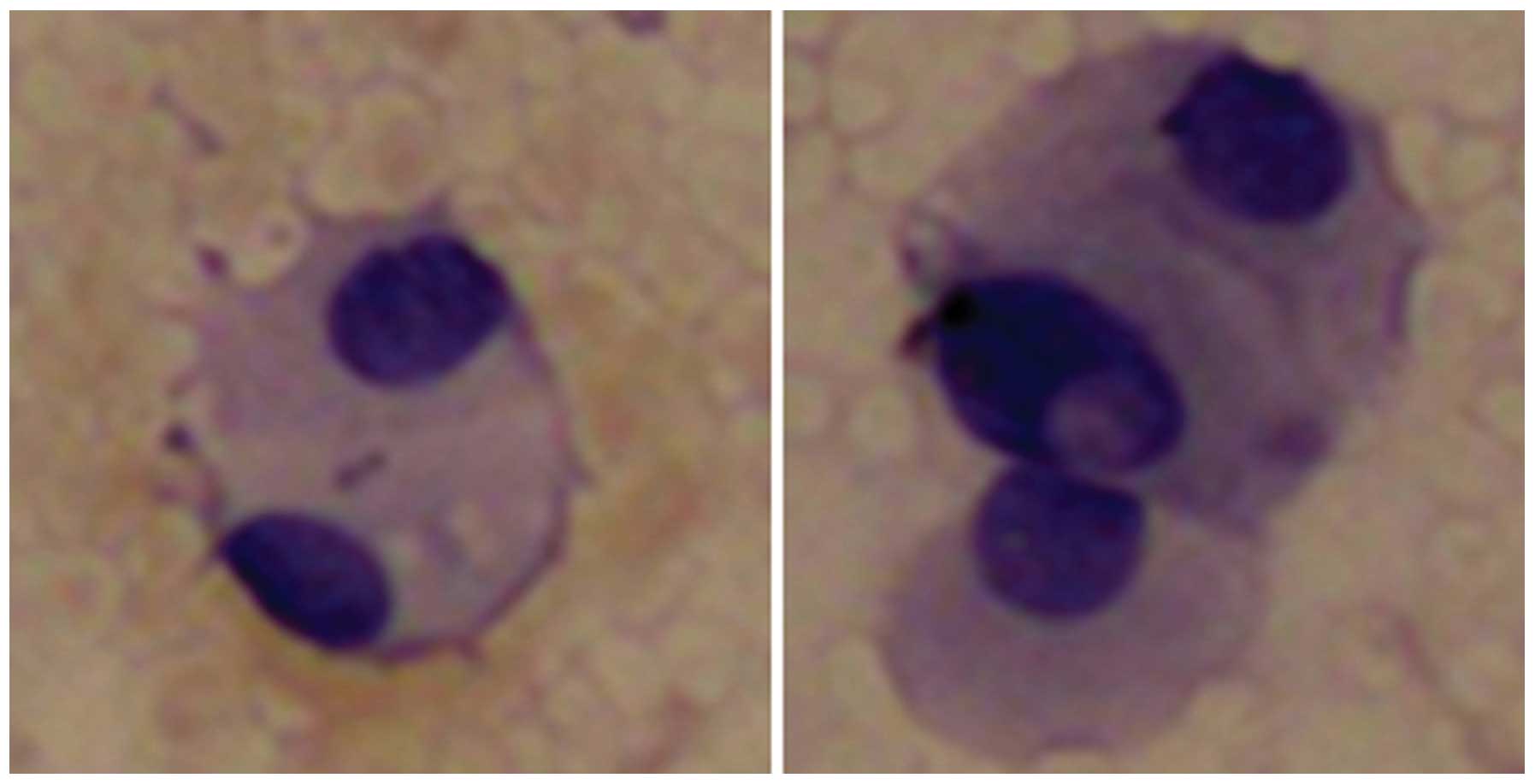
cm3 of yellow-white fluid (Fig. 4), and a smear of the hydatid fluid
showed atypical cells (Fig. 5).
Histopathology revealed the biopsy specimen to be a metastatic
adenosquamous carcinoma originating from the lung. The sample
exhibited similar hematoxylin and eosin morphology to lung
adenosquamous carcinoma with predominant well-differentiated
adenocarcinoma associated with heterologous elements of squamous
cell carcinoma. An MRI scan for gamma knife radiosurgery planning
conducted following stereotactic aspiration showed that the cystic
tumor in the pons had decreased in size to 18×15×14 mm (volume, 1.9
cm3; Figure 6). The
patient’s vertigo and gait instability improved within three days
following the aspiration, and a second GKRS was performed one week
later (dose, 12.0 Gy). Following discharge from hospital, the
patient was alert and the neurological symptoms had resolved. A
further MRI scan was performed five months subsequent to the repeat
GKRS, revealing that the brainstem metastasis had reduced to
12×13×14 mm (volume, 1.2 cm3), without severe
radiation-induced edema (Fig. 7).
MRI also indicated that the brainstem metastasis was well
controlled. The patient survived for 12 months following the repeat
GKRS, however, later succumbed to the disease after lapsing into a
two-week coma following the development and progression of new
brain metastases.
Discussion
A number of reports have described the treatment of
brainstem metastasis, including pontine metastasis (1–11). The
most common site of primary malignancy in patients with metastases
to the brainstem is the lungs; the majority of such malignancies
are adenocarcinomas (6,7,9,10) and,
less commonly, squamous cell carcinomas (8). SRS is the preferred treatment option
for brainstem metastases due to its provision of adequate local
control with low morbidity. Accurate targeting of the tumor may
limit damage to the surrounding healthy brain tissue, thereby
mitigating the neurological decline (3,6,15).
Between 1999 and 2014, >20 studies reported the clinical
characteristics, radiation doses and outcomes of brainstem
metastases following SRS treatment (Table I). In these reports, the median
survival time of patients with brainstem metastases ranged from
4–16.8 months (2–21).
 | Table IPreviously published studies of
stereotactic radiosurgery for brainstem metastases. |
Table I
Previously published studies of
stereotactic radiosurgery for brainstem metastases.
| Author (ref) | Year | Patients, n | Lesions, n | Patients with WBRT,
n | SRS modality | Median age,
years | Median tumor volume,
cm3 | Median tumor margin
dose, Gy | Median follow-up,
months | Median survival,
months | Local control
rate,% |
|---|
| Huang et al
(2) | 1999 | 26 | 27 | 24 | GKRS | 62 | 1.1 | 16 | 9.4 | 9 | 95 |
| Shuto et al
(3) | 2003 | 25 | 31 | 9 | GKRS | 54 | 2.1 | 13 | 5.2 | 4.9 | 77.4 |
| Fuentes et al
(4) | 2006 | 28 | 28 | 6 | GKRS | 57.5 | 2.1 | 19 | 11 | 12 | 92 |
| Yen et al
(5) | 2006 | 53 | 53 | 21 | GKRS | 57.3 | 2.8 | 18 | 9.8 | 11 | 86.5 |
| Hussain et
al (6) | 2007 | 22 | 25 | 3 | GKRS | 60 | 0.9 | 16 | 8.5 | 8.5 | 100 |
| Kased et al
(7) | 2008 | 42 | 44 | 24 | GKRS | 55 | 0.26 | 16 | 6.9 | 9 | 77 |
| Lorenzoni et
al (8) | 2009 | 25 | 27 | 17 | GKRS | 53 | 0.6 | 20 | 10.5 | 11.1 | 95 |
| Samblas et
al (9) | 2009 | 28 | 30 | 27 | LINAC | 52.3 | 1.86 | 11.1 | NA | 16.8 | NA |
| Koyfman et
al (10) | 2010 | 43 | 43 | 34 | GKRS | 59 | 0.37 | 15 | 5.3 | 5.8 | 85 |
| Yoo et al
(11) | 2011 | 32 | NA | NA | GKRS | 50 | 1.5 | 15.9 | 12 | 7.7 | 87.5 |
| Hatiboglu et
al (12) | 2011 | 60 | 60 | 9 | LINAC | 61 | 1 | 15 | 5.3 | 4 | 76 |
| Valery et al
(13) | 2011 | 30 | 43 | 4 | LINAC | 57 | 2.82 | 13.4 | 10.4 | 10 | 90 |
| Kelly et al
(14) | 2011 | 24 | 24 | 23 | LINAC | 57 | 0.2 | 13 | 6.6 | 5.3 | 78.6 |
| Li et al
(15) | 2012 | 28 | 32 | 0 | GKRS | 61 | 0.78 | 16 | NA | 9 | 90.6 |
| Kawabe et al
(16) | 2012 | 200 | 222 | 13 | GKRS | 64 | 0.2 | 18 | NA | 6 | 81.8 |
| Lin et al
(17) | 2012 | 45 | 48 | 17 | LINAC | 59.9 | 0.4 | 14 | NA | 11.6 | 88 |
| Sengaez et
al (18) | 2013 | 44 | 46 | 29 | GKRS | 57 | 0.6 | 16 | NA | 8 | 96 |
| Jung et al
(19) | 2013 | 32 | 32 | 19 | GKRS | 50 | 0.711 | 13 | 6 | 5.2 | 87.5 |
| Kilburn et
al (20) | 2014 | 44 | 52 | 25 | GKRS | 57 | 0.134 | 18 | 10 | 6 | 88 |
| Peterson et
al (21) | 2014 | 41 | NA | 19 | GKRS | 59 | 0.66 | 17 | NA | 4.40 | 91 |
In the present case, the patient was initially
diagnosed based on clinical and neuroimaging assessments performed
at the Department of Neurosurgery, The Affiliated Hospital of
Beihua University. Consistent with the standard treatment of
irradiation of brain metastases, the patient underwent GKRS of the
brainstem metastasis over 40 days with a total dose of 54.0 Gy.
This dose was deemed appropriate based on the study by Maranzano
et al (22), who reported
that the brain tolerated a single course of radiotherapy of 50–60
Gy in 2 Gy daily fractions. However, in the current case, MRI
performed three months following GKRS showed an increase in the
size of the cystic mass. The patient was therefore referred to the
China-Japan Union Hospital of Jilin University for further
treatment.
As part of the clinical evaluation, it was critical
to determine whether the mass was a metastatic growth or a
high-grade glioma. Server et al (23) reported that MRS may be utilized to
differentiate high-grade glioma from metastases, particularly when
the performed in conjunction with measurement of the peritumoral
Cho/NAA ratio, which has a high sensitivity (100%). In the current
case, the results of these tests indicated the presence of a
metastatic carcinoma.
Stereotactic aspiration is a minimally invasive
technique. It is widely used to treat brain abscesses (24), and is an important component of the
multimodal treatment of cystic craniopharyngiomas (25). Several studies have also applied
stereotactic aspiration for the treatment of glial and metastatic
brain tumors (26–28). Higuchi et al (26) used a procedure in which stereotactic
aspiration followed by GKRS on the same day provided good tumor
control in 25 patients with cystic metastases. Park et al
(27) performed stereotactic
aspiration, which was followed by GKRS, in 24 patients with cystic
metastatic brain tumors. Following treatment, 13 patients (54.2%)
had good tumor control, five patients (20.8%) exhibited local tumor
progression, and six patients (25.0%) had remote progression. The
overall median survival time was 17.8 months, and no cases of
brainstem metastasis were identified. To the best of our knowledge,
Aung et al (29) were the
first to report a patient with adenocarcinoma of the right main
bronchus that disseminated to the pons, left cerebral peduncle, and
liver. In this case, CT-guided stereotactic aspiration of the
cystic pontine lesion was performed and a catheter inserted in the
cyst cavity was connected to a subgaleal Ommaya reservoir for
further aspiration and decompression. Although these procedures
alleviated the patient’s clinical symptoms, the patient succumbed
to the disease three weeks following the stereotactic surgery,
after becoming comatose, with jaundice and ascites. Matsumoto et
al (30) reported a patient
with a cystic metastasis in the midbrain that was successfully
treated by brachytherapy following stereotactic biopsy and
aspiration of the intratumoral cyst. The authors reported that
stereotactic aspiration of cystic lesions provides clinical
improvement, and brachytherapy prevents cyst recurrence. In our
previous report (31), we treated a
brainstem cystic glioma by combining stereotactic aspiration with
GKRS, with a favorable outcome. Therefore, we speculated that
stereotactic aspiration surgery may improve the effect of GKRS
treatment of cystic brainstem glioma.
In the present case, however, the cystic mass
progressed and disease control was lost following the initial GKRS.
As the results from prior reports and our previous case indicated
that stereotactic aspiration of the cystic mass may be an effective
treatment, the patient underwent CT-guided stereotactic biopsy,
which yielded 2.0 cm3 of cystic fluid. Histopathological
analysis of the exudate confirmed the origin as primary
adenosquamous carcinoma of the lung. Following stereotactic
aspiration, GKRS was repeated, reducing the volume of the mass to
1.9 cm3. An MRI scan performed five months following the
repeat GKRS revealed a controlled mass of 1.2 cm3
without substantial radiotherapy-induced edema. However, a second
metastatic lesion was detected in the cerebellum of this patient
following the second GKRS. The patient survived for 17 months
following the first MRI (12 months after the repeat GKRS).
Adenosquamous carcinoma is an uncommon lung cancer,
accounting for 0.4–4% of all primary lung cancers, in which ≥10% of
the tumor volume contains adenocarcinoma and squamous cell
carcinoma components. Adenosquamous carcinomas have a significantly
poorer prognosis compared with adenocarcinomas and squamous cell
carcinomas. Brain metastasis is common in patients with
adenosquamous carcinoma of the lung, however, metastasis to the
brainstem from this carcinoma is extremely uncommon (32–35),
and the present case is the first in which adenosquamous carcinoma
of the lung with metastasis to the brainstem has been reported.
Furthermore, the current case is the first to report stereotactic
aspiration and GKRS for the treatment of a cystic brainstem
metastasis. This treatment provided good local tumor control and
the patient survived for 12 months following the procedure. The
patient’s survival time of 17 months from initial diagnosis is
longer than that of patients reported elsewhere. This indicates
that the use of multiple treatment modalities, including
stereotactic aspiration combined with GKRS, may extend the survival
time of patients with cystic brainstem metastases.
In conclusion, this case suggests that cyst drainage
by stereotactic aspiration improves the effects of GKRS in the
treatment of cystic brainstem metastasis, by reducing the tumor
burden and enhancing local tumor control. To date, there are no
evident-based guidelines for the treatment of brainstem metastasis;
for the brainstem metastasis with cystic components, multimodality
strategy combing stereotactic aspiration with GKRS may be
considered. Furthermore, large series of patients with cystic
brainstem metastasis should be studied to make the final
disgnosis.
Abbreviations:
|
SRS
|
stereotactic radiosurgery
|
|
GKRS
|
gamma knife radiosurgery
|
|
MRI
|
magnetic resonance imaging
|
|
CT
|
computed tomography
|
|
MRS
|
magnetic resonance spectroscopy
|
References
|
1
|
Lamm AF, Elaimy AL, Lamoreaux WT, et al: A
review of the clinical outcomes for patients diagnosed with
brainstem metastasis and treated with stereotactic radiosurgery.
ISRN Surg. 2013:6528952013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Huang CF, Kondziolka D, Flickinger JC and
Lunsford LD: Stereotactic radiosurgery for brain stem metastases. J
Neurosurg. 91:563–568. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shuto T, Fujino H, Asada H, et al: Gamma
knife radiosurgery for metastatic tumours in the brain stem. Acta
Neurochir (Wien). 145:755–760. 2003. View Article : Google Scholar
|
|
4
|
Fuentes S, Delsanti C, Metellus P, et al:
Brain stem metastases: management using gamma knife radiosurgery.
Neurosurgery. 58:37–42. 2006. View Article : Google Scholar
|
|
5
|
Yen CP, Sheehan J, Patterson G and Steiner
L: Gamma knife surgery for metastatic brain stem tumors. J
Neurosurg. 105:213–219. 2006. View Article : Google Scholar
|
|
6
|
Hussain A, Brown PD, Stafford SL and
Pollock BE: Stereotactic radiosurgery for brain stem metastases:
Survival, tumor control, and patient outcomes. Int J Radiat Oncol
Bio Phys. 67:521–524. 2007. View Article : Google Scholar
|
|
7
|
Kased N, Huang K, Nakamura JL, et al:
Gamma knife radiosurgery for brainstem metastases: the UCSF
experience. J Neurooncol. 86:195–205. 2008. View Article : Google Scholar
|
|
8
|
Lorenzoni JG, Devriendt D, Massager N, et
al: Brain stem metastases treated with radiosurgery: prognostic
factors of survival and life expectancy estimation. Surg Neurol.
71:188–196. 2009. View Article : Google Scholar
|
|
9
|
Samblás JM, Sallabanda K, Bustos JC, et
al: Radiosurgery and whole brain therapy in the treatment of
brainstem metastases. Clinical Transl Oncol. 11:677–680. 2009.
View Article : Google Scholar
|
|
10
|
Koyfman SA, Tendulkar RD, Chao ST, et al:
Stereotactic radiosurgery for single brainstem metastases: the
cleveland clinic experience. Int J Radiat Oncol Bio Phys.
78:409–414. 2010. View Article : Google Scholar
|
|
11
|
Yoo TW, Park ES, Kwon do H and Kim CJ:
Gamma knife radiosurgery for brainstem metastases. J Korean
Neurosurg Soc. 50:299–303. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hatiboglu MA, Chang EL, Suki D, et al:
Outcomes and prognostic factors for patients with brainstem
metastases undergoing stereotactic radiosurgery. Neurosurgery.
69:796–806. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Valery CA, Boskos C, Boisserie G, et al:
Minimized doses for linear accelerator radiosurgery of brainstem
metastasis. Int J Radiat Oncol Biol Phys. 80:362–368. 2011.
View Article : Google Scholar
|
|
14
|
Kelly PJ, Lin YB, Yu AY, et al: Linear
accelerator-based stereotactic radiosurgery for brainstem
metastases: the Dana-Farber/Brigham and Women’s Cancer Center
experience. J Neurooncol. 104:553–557. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li Y, Xu D, Zhang Z, et al: Gamma knife
surgery for brainstem metastases. J Neurosurg. 117:13–16.
2012.PubMed/NCBI
|
|
16
|
Kawabe T, Yamamoto M, Sato Y, et al: Gamma
Knife surgery for patients with brainstem metastases. J Neurosurg.
117:23–30. 2012.PubMed/NCBI
|
|
17
|
Lin CS, Selch MT, Lee SP, et al:
Accelerator-based stereotactic radiosurgery for brainstem
metastases. Neurosurgery. 70:953–958. 2012. View Article : Google Scholar
|
|
18
|
Sengöz M, Kabalay IA, Tezcanlı E, Peker S
and Pamir N: Treatment of brainstem metastases with gamma-knife
radiosurgery. J Neurooncol. 113:33–38. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jung EW, Rakowski JT, Delly F, et al:
Gamma Knife radiosurgery in the management of brainstem metastases.
Clin Neurol Neurosurg. 115:2023–2028. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kilburn JM, Ellis TL, Lovato JF, et al:
Local control and toxicity outcomes in brainstem metastases treated
with single fraction radiosurgery: is there a volume threshold for
toxicity? J Neurooncol. 117:167–174. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Peterson HE, Larson EW, Fairbanks RK, et
al: Gamma knife treatment of brainstem metastases. Int J Mol Sci.
15:9748–9761. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Maranzano E, Trippa F, Pacchiarini D, et
al: Re-irradiation of brain metastases and metastatic spinal cord
compression: clinical practice suggestions. Tumori. 91:325–330.
2005.PubMed/NCBI
|
|
23
|
Server A, Josefsen R, Kulle B, et al:
Proton magnetic resonance spectroscopy in the distinction of
high-grade cerebral gliomas from single metastatic brain tumors.
Acta Radiol. 51:316–325. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lü Y, Li C, Liu M, et al: MRI-guided
stereotactic aspiration of brain abscesses by use of an optical
tracking navigation system. Acta Radiol. 55:121–128. 2014.
View Article : Google Scholar
|
|
25
|
Hofmann BM, Höllig A, Strauss C, Buslei R,
Buchfelder M and Fahlbusch R: Results after treatment of
craniopharyngiomas: further experiences with 73 patients since
1997. J Neurosurg. 116:373–384. 2012. View Article : Google Scholar
|
|
26
|
Higuchi F, Kawamoto S, Abe Y, Kim P and
Ueki K: Effectiveness of a 1-day aspiration plus Gamma Knife
surgery procedure for metastatic brain tumor with a cystic
component. J Neurosurg. 117:17–22. 2012.PubMed/NCBI
|
|
27
|
Kim IY, Yun SJ, Lee JS, et al: Brain
metastasis from extramammary Paget’s disease of the scrotum. J Clin
Neurosci. 21:694–696. 2014. View Article : Google Scholar
|
|
28
|
Park WH, Jang IS, Kim CJ and Kwon do H:
Gamma knife radiosurgery after stereotactic aspiration for large
cystic brain metastases. J Korean Neurosurg Soc. 46:360–364. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Aung TH, Kwok CK, Mark YF and Mark EG:
Computed tomography-guided stereotactic aspiration and biopsy of a
cystic metastatic adenocarcinoma of the pons. Hong Kong Med J.
3:232–235. 1997.PubMed/NCBI
|
|
30
|
Matsumoto K, Tada E, Tamesa N, Tomita S
and Ohmoto T: Stereotactic brachytherapy for a cystic metastatic
brain tumor in the midbrain. Case report. J Neurosurg. 88:141–144.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhao X, Du C and Tian Y: Results Of Repeat
Gamma Knife Treatment: Stereotactic Aspiration Surgery Can Improve
the Effect of Gamma Knife Treatment for Cystic Small Brainstem
Glioma: Case Report. Neurosurgery Quarterly. 22:22–25. 2012.
View Article : Google Scholar
|
|
32
|
Nakagawa K, Yasumitu T, Fukuhara K, Shiono
H and Kikui M: Poor prognosis after lung resection for patients
with adenosquamous carcinoma of the lung. Ann Thorac Surg.
75:1740–1744. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gawrychowski J, Bruliński K, Malinowski E
and Papla B: Prognosis and survival after radical resection of
primary adenosquamous lung carcinoma. Eur J Cardiothorac Surg.
27:686–692. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cooke DT, Nguyen DV, Yang Y, et al:
Survival comparison of adenosquamous, squamous cell and
adenocarcinoma of the lung after lobectomy. Ann Thorac Surg.
90:943–948. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Filosso PL, Ruffini E, Asioli S, et al:
Adenosquamous lung carcinomas: a histologic subtype with poor
prognosis. Lung Cancer. 74:25–29. 2011. View Article : Google Scholar : PubMed/NCBI
|