Introduction
Liposarcoma is the most common type of soft-tissue
sarcoma, typically occurring in the lower extremities and
retroperitoneum and accounts for 10–16% of all sarcomas (1). Its diagnosis depends mainly on
histopathological characteristics such as typical lipoblasts, and
immunohistochemical features, namely MDM2, CDK4 and S-100 were
positive (2). By contrast,
mediastinal liposarcomas are rare and constitute <1% of all
mediastinal tumors worldwide (3). Few
cases have been described in the English literature (4–6).
Furthermore, the majority of cases were of giant liposarcomas
(5,6).
In addition, Boland et al (4)
considered that the majority of patients with
well-differentiated/undifferentiated liposarcoma had a protracted
clinical progression, in contrast to the more rapid disease
progression observed in patients with myxoid and plemorphic
liposarcoma. Liposarcomas originate from primitive mesenchymal
cells rather than mature fat cells (7). Thus, it may differentiate towards
various mesenchymal tissues. The current study presents a rare case
of a giant liposarcoma with smooth muscle and neural
differentiation in the mediastinum. Written informed consent was
obtained from the family of the patient.
Case report
A 27-year-old male was referred to the Thoracic
Surgical Hospital, (Weinan, China) in June 2012 due to a one-month
history of chest tightness and shortness of breath at rest. Chest
computed tomography revealed a bulky, well-defined mass in the
posterior mediastinum, which was subsequently resected by
thoracotomy and diagnosed as a fibrolipoma. Following the discharge
of the patient, no therapy was received. The patient was admitted
to Tangdu Hospital (Xi'an, China) in September 2013 with the
complaint of increasing chest tightness and shortness of breath 12
months after the initial thoracotomy had been performed. Imaging
features revealed a large mass extending from the posterior
mediastinum to the neck, indicating tumor recurrence. The patient
consequently underwent surgery to excise the mass. During the
surgical procedure the tumor was identified to have adhered to the
lower thyroid gland, compressing the superior vena cava and the
right wall of the trachea. Following complete excision of the mass,
the tumor was found to be 23×15×10 cm in size, with a yellow cut
surface. Its circumsciption was clear, with no conglutination with
the surrounding tissues, furthermore, the texture was soft.
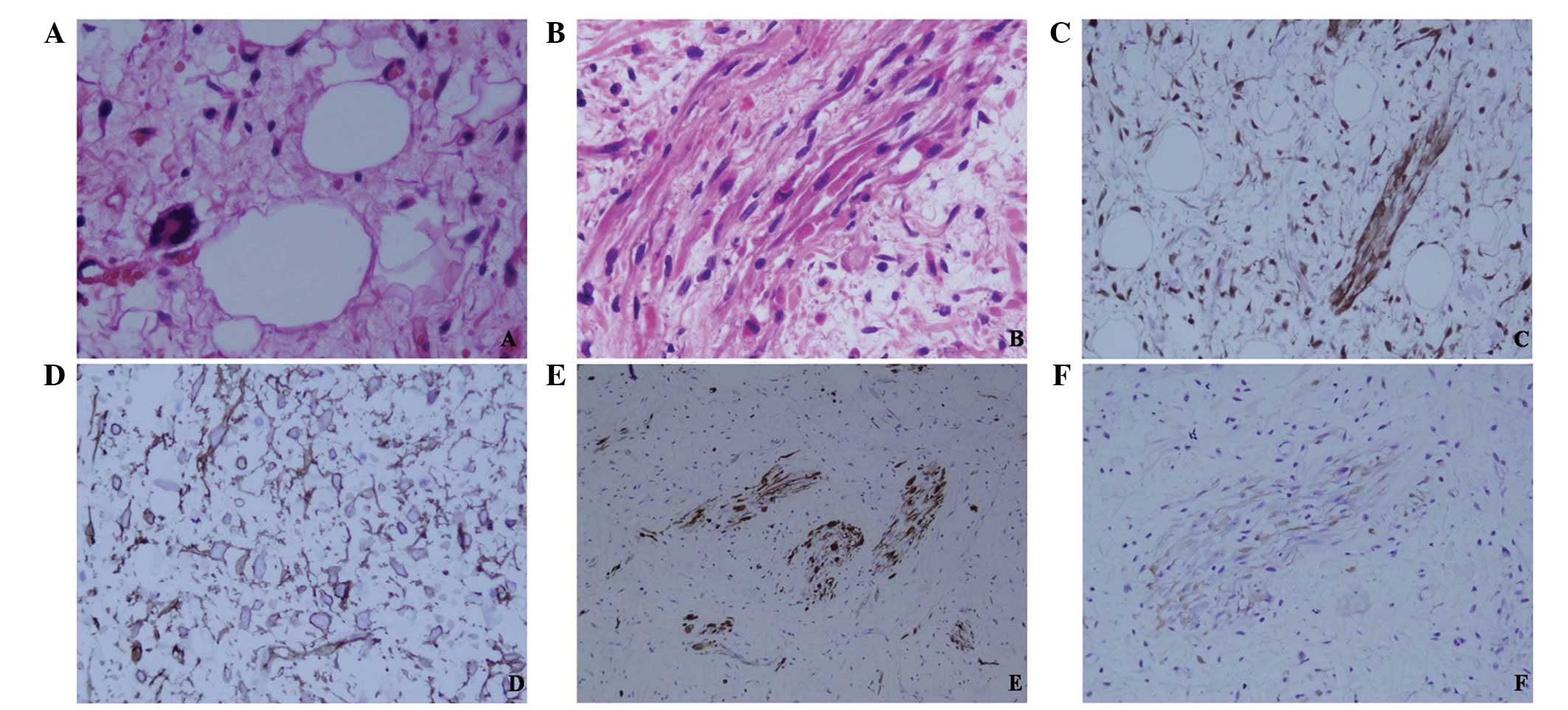
Microscopically, the tumor was composed of spindle cells organized
in a fascicular pattern and fat cells (Fig. 1A and B). Lipoblast cells were
identified, however, they were not abundant, and mitotic figures
were absent. Immunohistochemically, the spindle cells were positive
for vimentin, cyclin-dependent kinase (CDK)-4 (Fig. 1C), cluster of differentiation (CD) 34
(Fig. 1D), desmin (Fig. 1E), smooth muscle actin (SMA), myogenin
and neurofilament (NF; Fig. 1F), and
negative for glial fibrillary acidic protein, myoglobin, S-100,
epithelial membrane antigen, leukocyte common antigen, B-cell
lymphoma-2, CD99 and CD117. Thus, the tumor was diagnosed as a
well-differentiated liposarcoma with smooth muscle and neural
differentiation. A histological comparison between the initial
tumor slides obtained from the local hospital and the reoccurring
tumor tissue demonstrated evident differences. The initial tumor
was composed of fiber and fat tissues and no lipoblast cells were
identified; thus, there was no evidence of a well-differentiated
liposarcoma. Following surgery, the patient underwent radiation
treatment, a dose of 2 Gy was given five times a week, for 4–5
weeks.. The patient remains alive with no evidence of disease
recurrence at two months post-surgery.
Discussion
Liposarcoma arises from primitive mesenchymal cells
and commonly occurs in the lower extremities (75% of cases), with a
less frequent rate of occurrence in the retroperitoneum (20% of
cases) (8–10). Alternative sites of liposarcoma, such
as the abdomen, vulva and buttocks, have also been reported
(11); however, primary liposarcoma
of the mediastinum is rare, comprising <1% of all mediastinal
tumor cases (only 130 cases have been described in the Western
literature thus far) (3). The
majority of cases occur in patients aged >40 years, with a mean
age range of 43–58 years (total age range, 3–72 years).
Furthermore, there is no apparent difference in the incidence rate
between genders (12,13). Mediastinal liposarcomas may grow to a
large size (mean tumor size, 15.7 cm; range, 2.2–61 cm),
compressing the surrounding organs and causing symptoms such as
shortness of breath, chest pain, dyspnea and tachypnea (14,15). The
patient in the present study was young (age, 27 years) and
exhibited a tumor with a large diameter (23 cm), which caused it to
compress the trachea.
Liposarcoma is histologically classified into the
following five subtypes, according to the most recent World Health
Organization Classification of Soft Tissue Tumors: i)
Well-differentiated, ii) myxoid, iii) round cell, iv)
dedifferentiated and v) pleomorphic (2). These histological subtypes correlate
with the clinical behavior and prognosis; for example, the
excessive size of mediastinal liposarcomas may result in invasion
of the surrounding structures, such as the pericardium, superior
vena cava, heart, trachea, bronchi and esophagus, causing symptoms
such as shortness of breath, dyspnea and pain. Additionally, the
prognosis of patients with dedifferentiated or pleomorphic
liposarcomas is poor compared with patients with
well-differentiated liposarcomas (12). Despite its rapid recurrence, the case
presented in the current study may be histologically classified as
a well-differentiated liposarcoma, according to its histological
features. However, its immunohistochemical features, including
spindle cells positive for CD34, CDK4, NF, desmin and SMA, indicate
a diagnosis of well-differentiated liposarcoma with smooth muscle
and neural differentiation. To the best of our knowledge, the
present study is the first to report this specific subtype of
liposarcoma.
The recurrence of established liposarcoma is common,
with the majority of cases reoccurring within the first six months,
although recurrence may be delayed for up to 5–10 years following
the initial excision (16). In the
present case, the patient exhibited tumor recurrence 12 months
after discharge from the local hospital. Despite an initial
diagnosis of a benign fibrolipoma, the second resected tumor
indicated a low-grade malignant liposarcoma. One possible
explanation of these different diagnoses is that the primitive
tumor became malignant one year after the surgery. An alternative
explanation is that the true malignant lesion was not identified as
only a limited sample was resected. Overall, the present study
indicates a requirement for long-term and careful follow-up for
tumors in the mediastinum, regardless of whether the tumor was
initially diagnosed as benign.
Surgical removal with a wide margin is the optimal
treatment strategy for mediastinal liposarcoma, with chemotherapy
and radiotherapy appearing ineffective as adjuncts to surgical
excision in unresectable or incompletely resected tumors (17,18). The
prognosis is dependent on the histological subtype and the
completion of surgical resection, with myxoid or pleomorphic
subtype patients exhibiting a poorer prognosis compared with
well-differentiated tumors (12).
Furthermore, a number of previous studies have reported a five-year
survival rate of 34.9% for the well-differentiated subtype and
21.0% for the pleomorphic subtype (8,10,19).
In conclusion, to the best of our knowledge, the
current study is the first to report a case of well-differentiated
liposarcoma with smooth muscle and neural differentiation in the
mediastinum. Furthermore, the study indicates the requirement for a
long-term follow-up period for patients with mediastinal tumors,
even after a diagnosis of a benign tumor arising from the
mesenchymal tissue. Multiple tissues should be sampled and
histologically investigated to achieve an accurate diagnosis.
References
|
1
|
Conesa X, Seijas R, Ares O, et al:
Multicentric liposarcoma. Acta Orthop Belg. 77:9–14.
2011.PubMed/NCBI
|
|
2
|
Fletcher CDM, Unni KK and Mertens F:
Pathology and genetics of tumours of soft tissue and boneIn: World
Health Organization Classification of Tumours. IARC Press; Lyon,
France: pp. 35–44. 2002
|
|
3
|
Kashu Y, Yukumi S, Tsunooka N, Tanigawa K,
Arakane M, Nakagawa H and Kawachi K: Successful resection of a
massive mediastinal liposarcoma that rapidly extended into the
entire left thoracic cavity: report of a case. Surg Today.
42:68–71. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Boland JM, Colby TV and Folpe AL:
Liposarcomas of the mediastinum and thorax: a clinicopathologic and
molecular cytogenetic study of 24 cases, emphasizing unusual and
diverse histologic features. Am J Surg Pathol. 36:1395–1403. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Matsuo T, Takamori S, Hayabuchi N, et al:
Giant liposarcoma occupying most of the hemi-thorax and resected in
the supine position: report of a rare case. Kurume Med J. 58:63–65.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Németh T, Géczi T, Tiszlavicz L, Wolfárd
A, Lázár G and Furák J: Giant fibrolipoma of the mediastinum. Magy
Seb. 64:235–238. 2011.[(In Hungarian)]. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sung MS, Kang HS, Suh JS, et al: Myxoid
liposarcoma: appearance at MR imaging with histologic correlation.
Radiographics. 20:1007–1019. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ohta Y, Murata T, Tamura M, Sato H,
Kurumaya H and Katayanagi K: Surgical resection of recurrent
bilateral mediastinal liposarcoma through the clamshell approach.
Ann Thorac Surg. 77:1837–1839. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Caraglia M, Montella L, Addeo R, et al:
Conditions suggesting lymphoma: case 2. Mediastinal liposarcoma in
a patient with previous testicular cancer. J Clin Oncol.
23:3844–3846. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Noji T, Morikawa T, Kaji M, Ohtake S and
Katoh H: Successful resection of a recurrent mediastinal
liposarcoma invading the pericardium: report of a case. Surg Today.
34:450–452. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Raghavan R, Raghuram P, Parekh PV and
Kurien JM: Posterior mediastinal liposarcoma simulating a lung
mass: an unusual case report. Cancer Imaging. 7:141–144. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Klimstra DS, Moran CA, Perino G, Koss MN
and Rosai J: Liposarcoma of the anterior mediastinum and thymus. A
clinicopathologic study of 28 cases. Am J Surg Pathol. 19:782–791.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hahn HP and Fletcher CD: Primary
mediastinal liposarcoma: clinicopathologic analysis of 24 cases. Am
J Surg Pathol. 31:1868–1874. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gaerte SC, Meyer CA, Winer-Muram HT,
Tarver RD and Conces DJ: Fat-containing lesions of the chest.
Radiographics. 22:S61–S78. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Attal H, Jensen J and Reyes CV: Myxoid
liposarcoma of the anterior mediastinum. Diagnosis by fine needle
aspiration biopsy. Acta Cytol. 39:511–513. 1995.PubMed/NCBI
|
|
16
|
Barbetakis N, Samanidis G, Paliouras D,
Boukovinas I, Kiziridou A and Tsilikas C: A rare cause of
mediastinal mass: Primary liposarcoma. J BUON. 13:429–431.
2008.PubMed/NCBI
|
|
17
|
Farah M, Abou-Sleiman P and Bahous J:
Primary mediastinal liposarcoma: a case report and review of the
literature. J Med Liban. 49:165–169. 2001.PubMed/NCBI
|
|
18
|
Enzinger FM and Weiss SW: LiposarcomaIn:
Soft Tissue Tumors. 3rd. Mosby; St. Louis, MO: pp. D431–D466.
1995
|
|
19
|
Kara M, Ozkan M, Dizbay Sak S and Kavukçu
ST: Successful removal of a giant recurrent mediastinal liposarcoma
involving both hemithoraces. Eur J Cardiothorac Surg. 20:647–649.
2001. View Article : Google Scholar : PubMed/NCBI
|