Introduction
Gastrointestinal stromal tumors (GISTs) are the most
prevalent mesenchymal tumors of the gastrointestinal tract
(1). GISTs are considered to
originate from the interstitial cells of Cajal (ICC), which are the
pacemakers of the peristaltic activity of the gastrointestinal
tract. GISTs mainly emerge in the stomach (60%), jejunum and ileum
(30%), colorectum, duodenum, esophagus and appendix (10%). However,
they may also be encountered in locations outside the
gastrointestinal tract, such as the omentum, mesentery and
retroperitoneum, in which case they are referred to extra-GISTs
(EGISTs) (2). More than 95% of GISTs
express KIT protein and discovered on GIST-1 (DOG-1), which are
considered to be the most specific and sensitive diagnostic markers
for GISTs. Approximately 80% of GISTs harbor a KIT mutation and
8–10% express mutations in the platelet-derived growth factor
receptor, α polypeptide (PDGFRα). Imatinib, a selective inhibitor
of KIT and PDGFRα, is a treatment agent effective against EGISTs
(1,2).
Case report
A 53-year-old male patient with severe dyspnea was
admitted to the Acibadem Adana Hospital (Adana, Turkey). A chest
computed tomography (CT) scan revealed a massive pericardial
effusion and pericardiocentesis was performed. A positron emission
tomography (PET)/CT scan performed following recurrence of
pericardial effusion revealed right pericardial hypermetabolic mass
lesions [maximum standardized uptake value (SUV), 12.1],
pericardial effusion, right hilar lymphadenopathy (maximum SUV,
4.9) and multiple metastatic nodules in both lungs. There was no
evidence of a primary malignancy originating from the
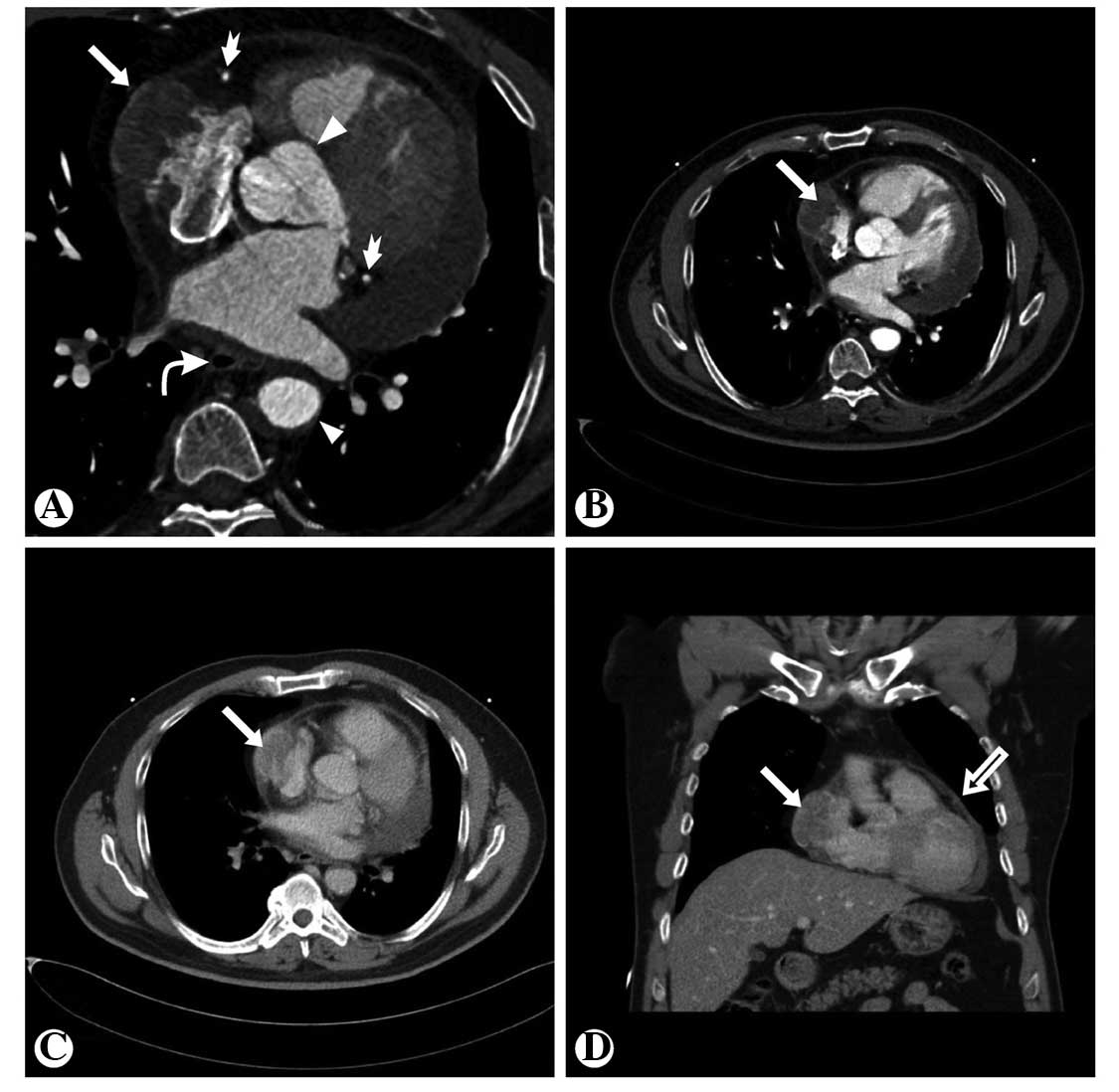
abdominopelvic cavity. The chest CT and coronary CT angiography
revealed that the pericardial mass involved the right atrium and
exhibited peripheral contrast enhancement. There was no association
between the pericardial mass and esophagus (Fig. 1). The lesion was considered to be
inoperable; a right thoracotomy and wedge resection were performed
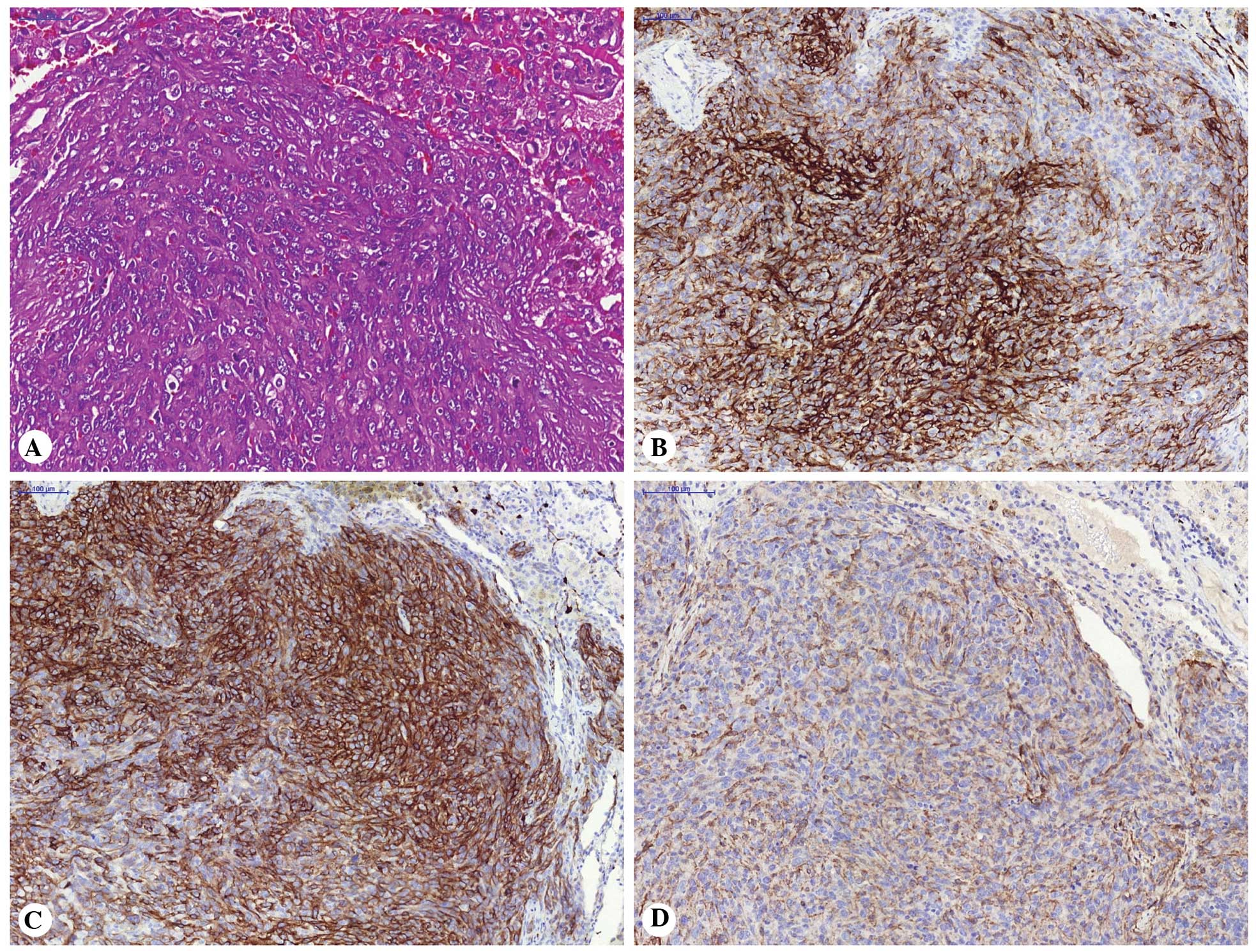
and a small number of lung nodules were resected. Microscopically,
the tumor was composed of spindle or ovoid cells with eosinophilic
cytoplasm and pleomorphic nuclei with conspicuous nucleoli. Mitotic
figures were frequently observed. Immunohistochemically, the tumor
cells were strongly positive for cluster of differentiation 117
(CD117; c-Kit) and CD34 and exhibited heterogeneous moderate
positivity for DOG-1 (Fig. 2). The
Ki-67 labeling index was 61%. The pathological diagnosis was
malignant EGIST. Therapy with adjuvant imatinib (400 mg/day) was
recommended. At the beginning of treatment, the patient responded
well, however, after a further 6 months the disease progressed and
the patient succumbed to the disease 18 months later. To the best
of our knowledge, this is the third reported case of EGIST
occurring above the diaphragm without being associated with the
esophageal wall. Two cases of primary EGIST originating from the
pleura were reported previously (1,2). In
addition, this is the first reported case of an EGIST originating
from the pericardium.
Discussion
EGISTs are considered to originate from the common
precursor cells that differentiate into this ICC-derived neoplasm
during development outside of the gastrointestinal tract. Another
theory is that this tumor may originate from the pluripotent
mesenchymal stem cells located outside of the gastrointestinal
tract (3). Contrary to GISTs, the
clinical findings of EGISTs are not comprehensively known and are
often associated with adverse prognostic factors, such as high
proliferative index, large size, lymph node involvement and distant
metastasis. The emergence of EGIST outside the gastrointestinal
tract may lead to a delay in the occurrence of clinical symptoms. A
number of these cases are diagnosed at a late stage, making
surgical resection difficult (1,2). A
mutational study on EGISTs demonstrated that this type of neoplasm
exhibits a lower frequency (41.4%) of KIT mutation at exon 11,
which may be the reason underlying the good response to imatinib
(4). Radiologically, these tumors are
often identified in the bowel wall, involving either the mucosal or
serosal surface. The tumor size ranges between 1 and 35 cm, with a
median size of 5 cm. In approximately two-thirds of the cases the
tumor margins are well-defined. Large tumors, in particular, may
display areas of hemorrhage and necrosis, leading to a
heterogeneous appearance on imaging. The enhancement pattern may be
homogeneous or heterogeneous (5–7).
References
|
1
|
Yi JH, Sim J, Park BB, et al: The primary
extra-gastrointestinal stromal tumor of pleura: a case report and a
literature review. Jpn J Clin Oncol. 43:1269–1272. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Long KB, Butrynski JE, Blank SD, et al:
Primary extragastrointestinal stromal tumor of the pleura: report
of a unique case with genetic confirmation. Am J Surg Pathol.
34:907–912. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: pathology and prognosis at different sites. Semin
Diagn Pathol. 23:70–83. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yamamoto H, Oda Y, Kawaguchi K, et al:
c-Kit and PDGFRA mutations in extragastrointestinal stromal tumor
(gastrointestinal stromal tumor of the soft tissue). Am J Surg
Pathol. 28:479–488. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee CM, Chen HC, Leung TK and Chen YY:
Gastrointestinal stromal tumor: computed tomographic features.
World J Gastroenterol. 10:2417–2418. 2004.PubMed/NCBI
|
|
6
|
Levy AD, Remotti HE, Thompson WM, Sobin LH
and Miettinen M: Gastrointestinal stromal tumors: radiologic
features with pathologic correlation. Radiographics. 23:283–304,
456, quiz 532. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ulusan S, Koc Z and Kayaselcuk F:
Gastrointestinal stromal tumours: CT findings. Br J Radiol.
81:618–623. 2008. View Article : Google Scholar : PubMed/NCBI
|