Introduction
Childhood pancreatic hemangioendothelioma (HE) is a
rare form of vascular anomaly that mainly occurs in infants
(1). Presenting signs and symptoms
include obstructive jaundice, hepatomegaly, palpable mass, duodenal
obstruction and intestinal bleeding (2). Ultrasound, computated tomography and
magnetic resonance imaging scanning, not only help in localising
the mass, but may also provide information on any associated
findings (2). Differential diagnosis
of pediatric pancreatic HE includes pseudopapillary tumor,
pancreatoblastoma, rhabdomyosarcoma and endocrine cell carcinoma.
The treatment of pancreatic HE is variable and dependent upon the
clinical presentation such as biliary obstruction and vascular
invasion (2). The present study
reports a case of pancreatic HE in terms of its clinical features,
treatment principles and prognosis through analysis of clinical
symptoms, pre-operational examinations, intraoperational findings
and pathological features. A literature review is also
presented.
Case report
Patient information
An 8-month-old female was admitted to the Department
of General Surgery in The Children's Hospital (Zhejiang University
School of Medicine, Hangzhou, Zhejiang, China) on January 3, 2011,
due to yellow skin and sclera that had been apparent for 1 week.
The patient presented with acute onset of the disease, and the
jaundice increased progressively. During the course of the disease,
the child exhibited anorexia, yellow urine and white stool, with no
abdominal pain, vomiting or fever. A physical examination upon
admission to the hospital found listlessness, mild malnutrition,
severe jaundice in the skin and sclera, and liver and spleen
enlargement.
Laboratory outcome
Liver function tests showed a total bilirubin level
of 270.3 µmol/l (1.71–17.1 µmol/l) and a direct bilirubin level of
248.6 µmol/l (0–3.4 µmol/l), suggesting obstructive jaundice.
Aspartate aminotransferase (254 U/l), alanine aminotransferase (242
U/l), pancreatic amylase and hepatitis-related tests all exhibited
normal results.
Imaging characteristics
Ultrasonography suggested a pancreatic head body
mass, distal common bile duct (CBD) obstruction and proximal CBD
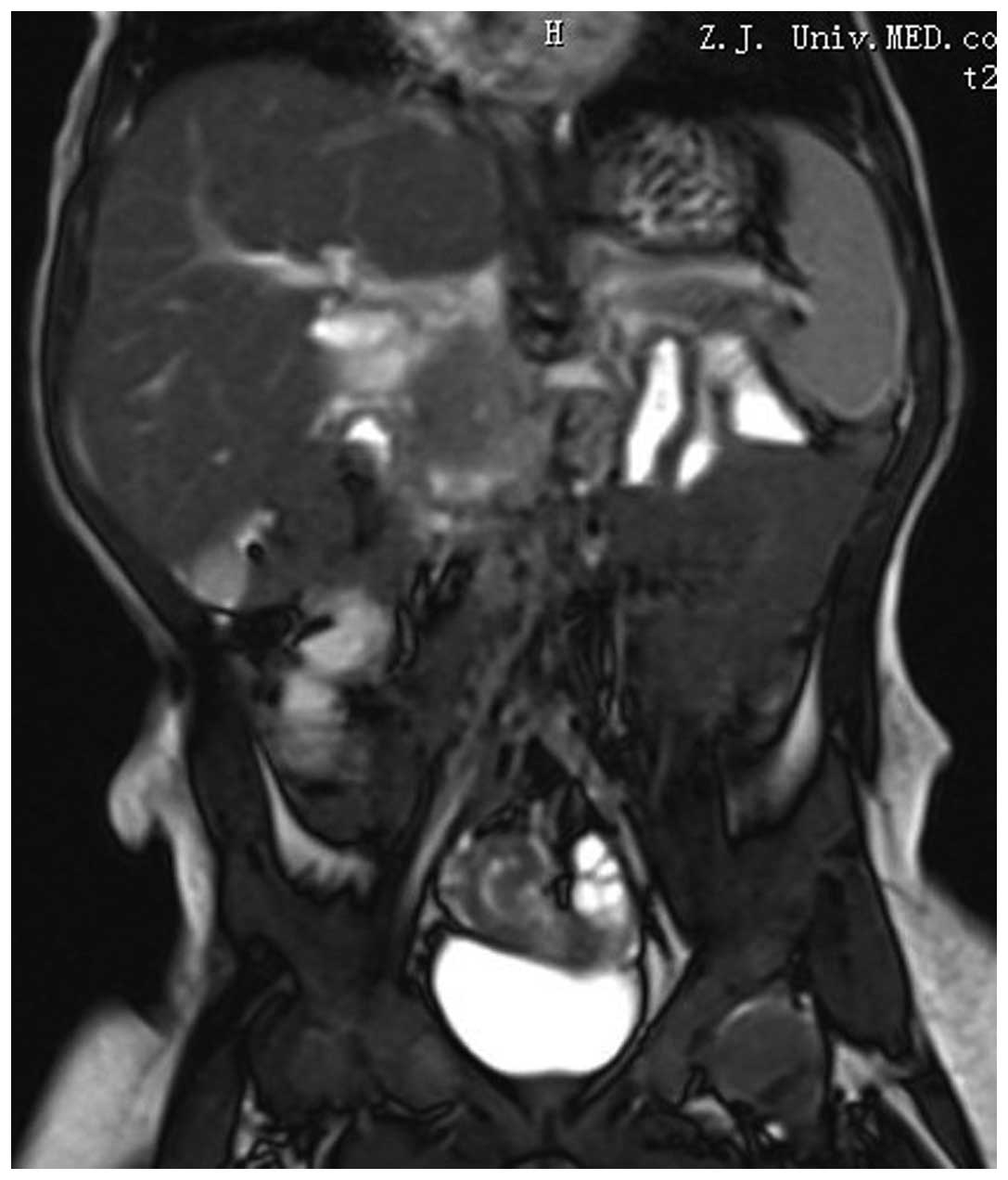
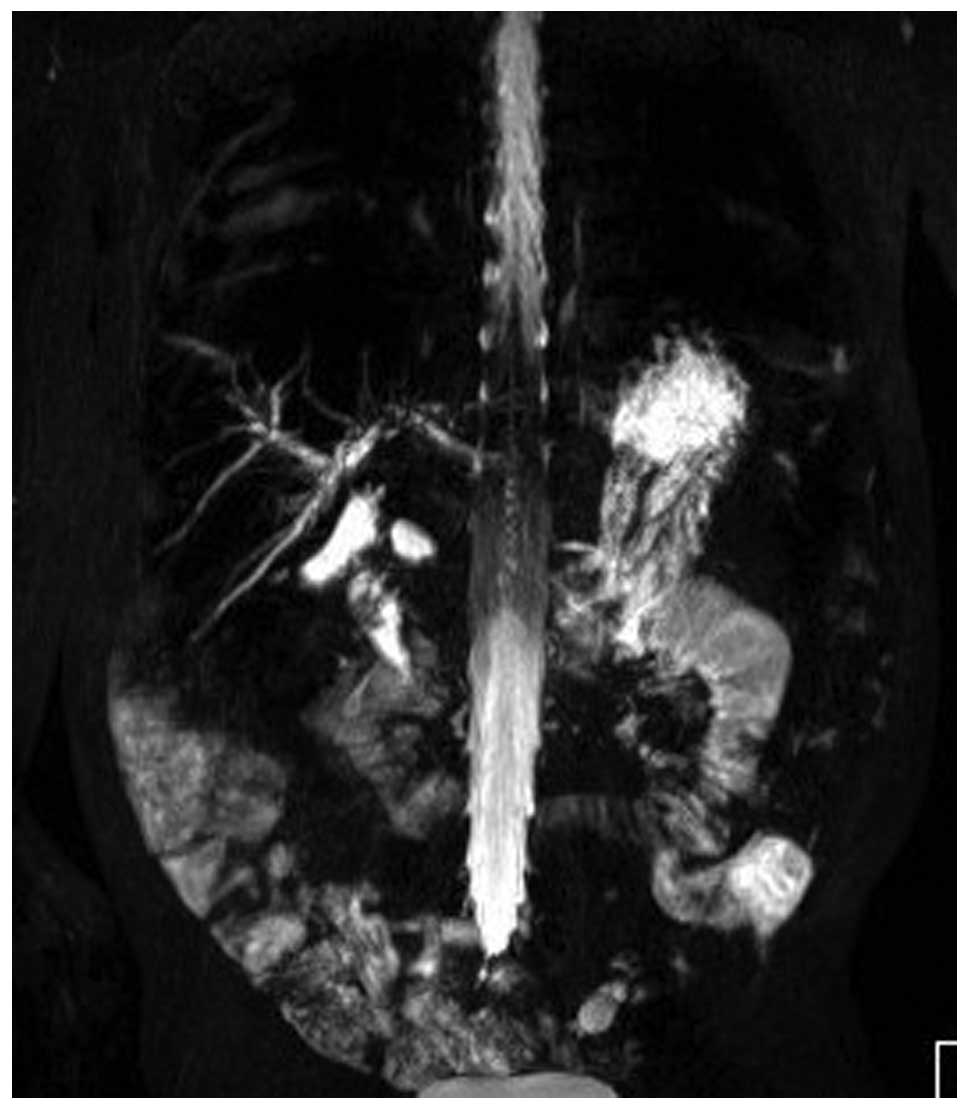
dilatation, with a diameter of ~1.5 cm. Magnetic resonance imaging
(MRI) showed dilatation in the left and right hepatic ducts, the
common hepatic duct and the CBD (Fig.
1), and a pancreatic head and body mass of ~4.7×5.2 cm, with a
strong signal. The portal vein and mesenteric vessels were closely
linked to the tumor (Fig. 2). Chest
computed tomography (CT) did not show any abnormalities.
Surgical procedure and treatment
Laparotomy was performed on January 11, 2011. During
the surgery, the mass was found to be solid and tough, located in
the head and body of the pancreas, and oppressing the CBD and
duodenum. The mass surrounded the portal vein, superior mesenteric
artery and vein, midcolic artery and vein, and was closely
associated with the inferior vena cava. Consequently, the mass
could not be removed. Examination of the spleen and adjacent
retroperitoneal lymph nodes did not show any abnormalities. An
intraoperative tumor frozen biopsy was performed. Tumor tissues,
and a small piece of liver tissue and hepatic lymph node were fixed
with formalin for inspection. The frozen specimen showed small
round cells, which were possibly benign.
Palliative surgery was decided upon. The gallbladder
was removed, the common hepatic duct was transected, and distal
closure was performed for the common hepatic duct. The proximal and
distal jejunum, which were already transected, were stitched with
an end-to-side anastomosis. Disarticulation of the gastric antrum,
removal of the pylorus and closure of the proximal duodenum were
performed. Following formation of the antrum, the antrum and liver
branch jejunum were stitched with an end-to-side anastomosis. The
transected proximal jejunum and the liver branch jejunum 40 cm from
the cholangio-intestinal anastomosis were stitched with an
end-to-side anastomosis.
Due to the benign nature of this tumor, chemotherapy
was not prescribed. The patient was treated by fasting,
gastrointestinal decompression, administration of antibiotics
(piperacillin sodium 100 mg/day for 7 days) and supportive
treatment (total parenteral nutrition, 75 Kcal/day for 7 days)
following the surgery.
Clinical presentation
The post-operative jaundice disappeared rapidly. The
patient started eating 1 week after the surgery and was discharged
1 week later. Liver function, pancreatic amylase level and other
measures were all normal prior to discharge. Ultrasonography showed
that the pancreatic mass had not increased in size, while a small
amount of intraperitoneal effusion was observed.
Pathological results
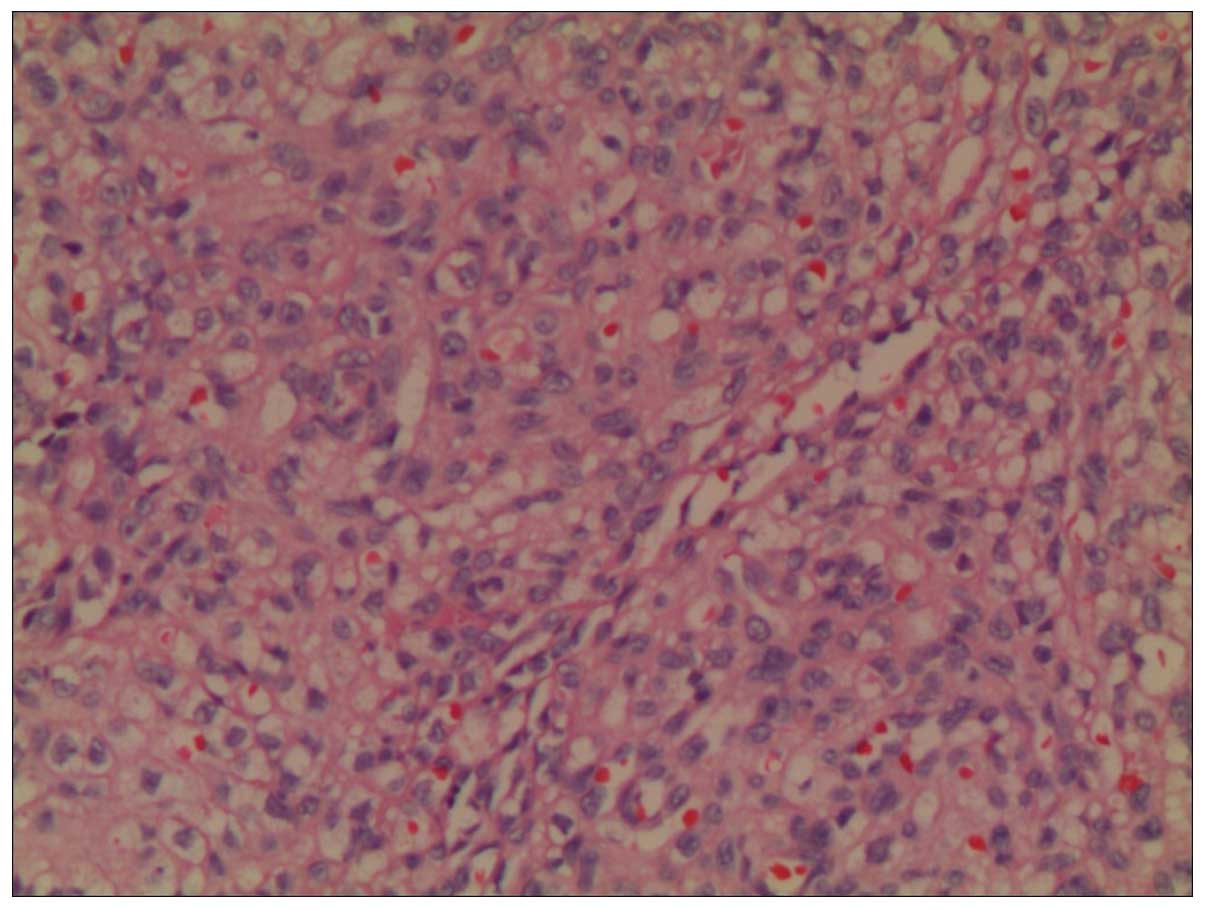
Vascular endothelial cell proliferation was
observed. A number of the cells formed a capillary with a small
cavity, and there was less cellular atypia and collagen fiber
hyperplasia between the tumor cells (Fig.
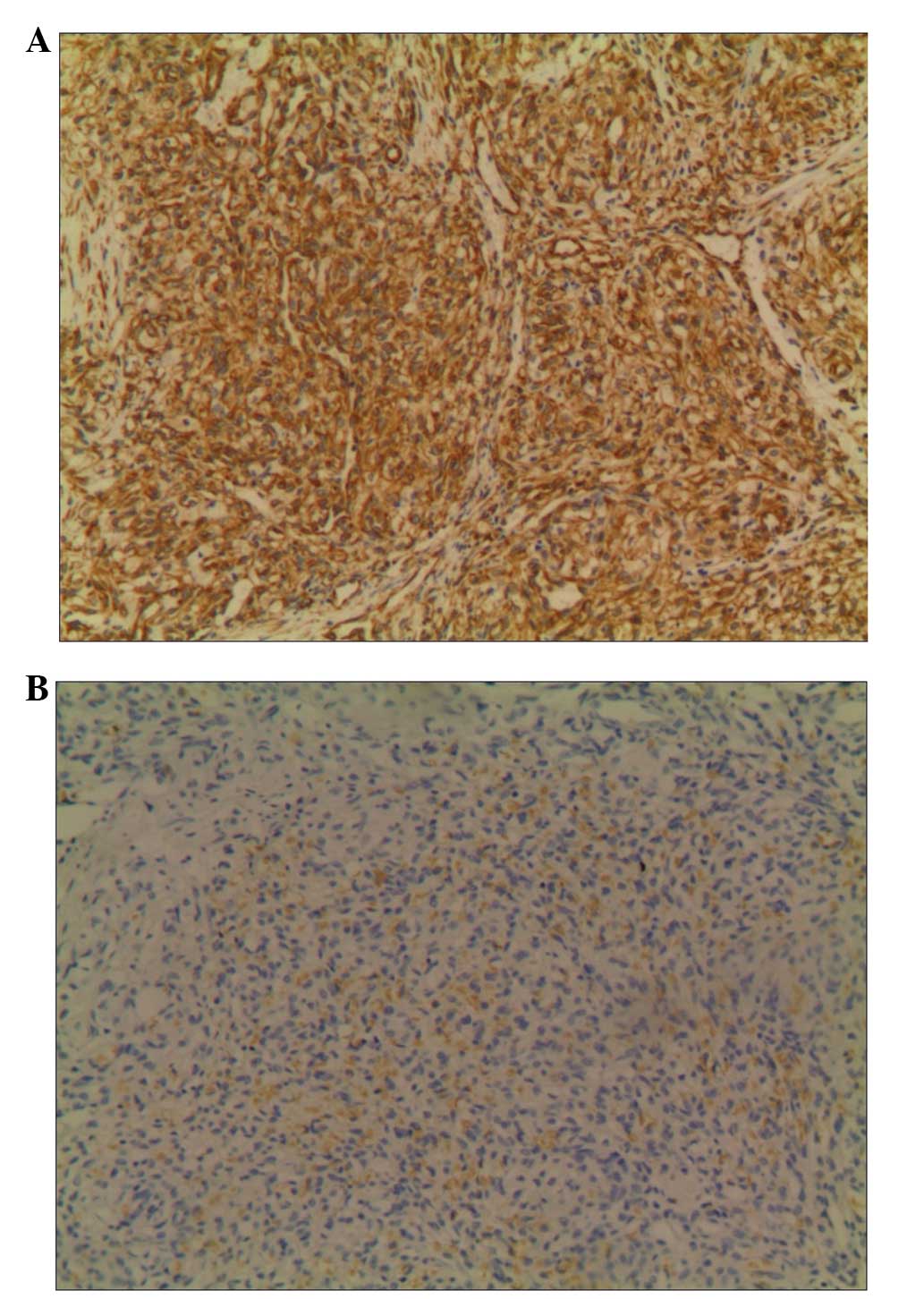
3). The immunohistochemical analysis showed that the tumor was
cluster of differentiation 34+, vimentin+,
S100−, glucose transporter 1−,
neuron-specific enolase−, chromogranin A+ and
epithelial membrane antigen+ (Fig. 4). The liver biopsy results showed
cholestatic liver cell swelling, mild portal area dilatation, small
bile duct hyperplasia, bile plug formation and infiltration of a
few inflammatory cells. A hepatic lymph node structure existed, but
no tumor invasion was found. The consequent diagnosis was of
pancreatic HE, with cholestatic hepatitis.
Follow-up
During the follow-up 3 months after the surgery, the
patient showed an increase in body weight, no abdominal pain or
jaundice, and urination and defecation were of a normal color.
Liver function and pancreatic amylase levels were normal.
Ultrasonography showed the size of the pancreatic head mass to be
~4.3×3.6×2.3 cm, which was slightly reduced compared with the
pre-operative size. During the follow-up at 28 months post-surgery,
the child showed good growth and development, no abdominal pain, a
good appetite, and normal urination and defecation. Upon
examination, no jaundice was observed in the skin and sclera, and
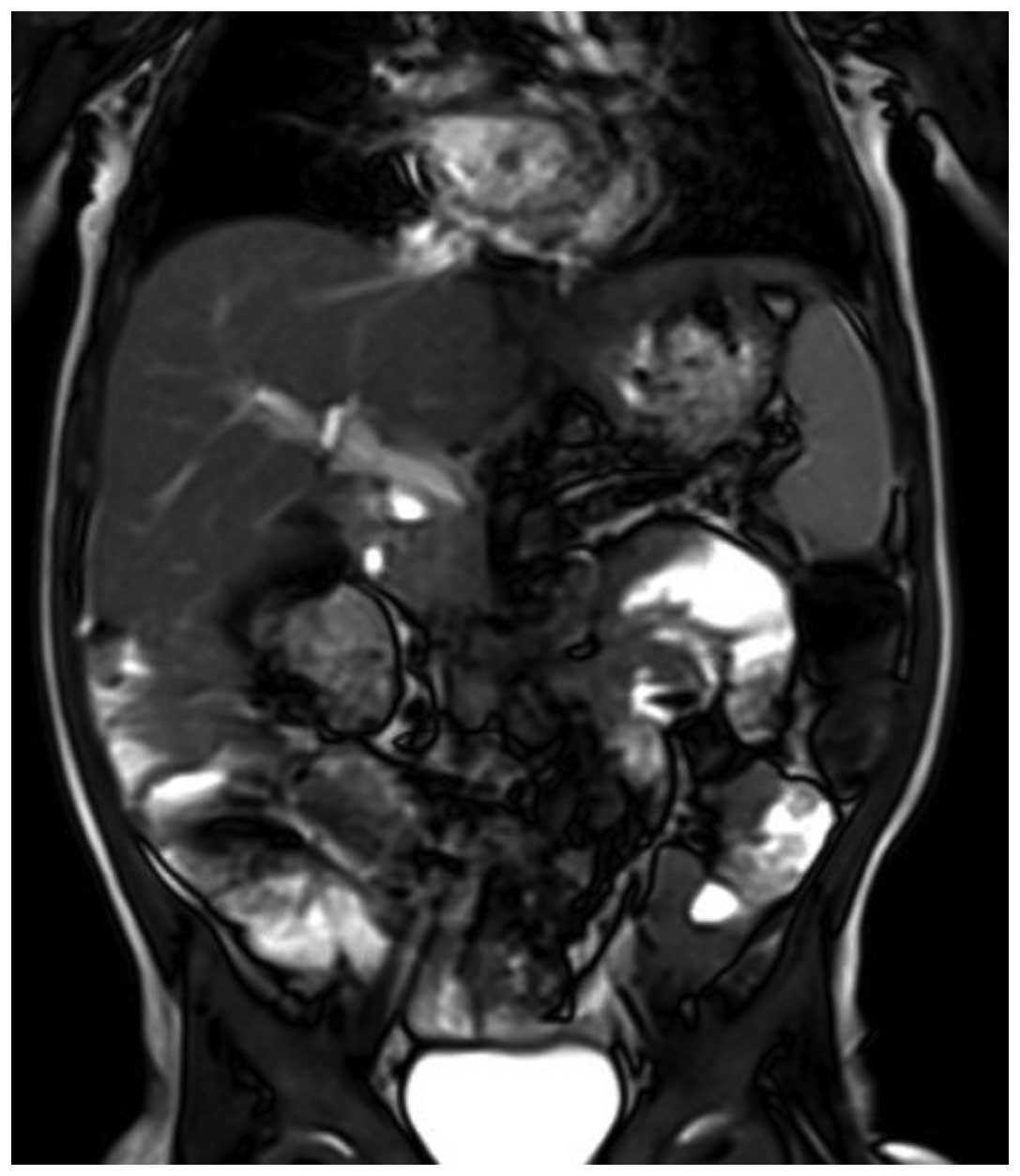
the abdomen was flat and soft. MRI showed the mass to be
~2.4×2.0×1.5 cm, which was a significantly reduced, but it was
still closely linked to the mesenteric vessels and portal vein. No
pancreatic duct dilatation and slight intrahepatic bile duct
dilatation were observed, and there were no abnormal signals in the
liver parenchyma (Figs. 5 and
6). Chest radiograph did not show any
abnormalities.
Discussion
Pediatric congenital vascular abnormalities are
extremely common, mostly occurring in the skin and soft tissues,
with fewer observed in the organs, whether single or multiple in
nature (3,4). The liver is the most commonly involved
organ (5). The most common
histological type of this disease is HE, which rarely occurs in the
pancreas (6).
PubMed was searched using the key words ‘pancreas
hemangioendothelioma infantile’, ‘pancreas kaposiform
hemangioendothelioma’, ‘juvenile hemangioendothelioma’ and ‘spindle
cell hemangioendothelioma’. The results showed that from 1973 to
the present date, only 9 studies on children with HE of the
pancreas have been published (7).
The case of a 3-year-old male with benign HE of the
pancreas was reported by Horie et al in 1985 (8). Obstructive jaundice was the presenting
symptom. The patient was treated with a temporary choledochojejunal
bypass, with no additional treatment. In the 16-month follow-up
period, the child remained well and asymptomatic. Laboratory data
showed no abnormalities. A biopsy specimen of the pancreatic head
showed a hemangiomatous pattern histologically. A positive reaction
to factor VIII-related antigen and endothelial cell marker was
noted on immunohistochemical study of the biopsy, supporting an
endothelial origin. It was concluded that the prognosis of HE is
favorable and that spontaneous regression can be expected,
therefore, the initial tumor treatment should be conservative.
In 1987, Sauer et al reported the case of a
5-month-old female with jaundice and dilatation of the hepatic bile
ducts (1). The pancreatic head and
hepatic portal vein had a 3-cm mass that completely blocked the
gallbladder and CBD. Cholecystectomy surgery was performed, and a
biopsy was performed of the tumor and regional lymph nodes. The
pathological diagnosis was HE without lymph node invasion.
Following the clear diagnosis, percutaneous biliary decompression
was performed. Drainage continued for 22 months until the
regression of the tumor. The study stated that this patient was the
youngest case of percutaneous biliary drainage that has been
reported.
In 1989, Villegas-Alvarez and Léon-Bojorge reported
the case of a 6-month-old male with a pancreatic head vascular
endothelial tumor, with Kasabach-Merritt syndrome (KMS) (9). The patient presented with
thrombocytopenia and gastrointestinal bleeding. The authors
believed that the vascular malformations and location of this
disease gave this case great clinical significance. This disease
commonly leads to neonatal obstructive jaundice and severe liver
disease, eventually resulting in mortality. Paradoxically, the
neoplasm is not considered malignant and the liver lesions that
were produced secondarily could have been prevented if the patient
was diagnosed correctly and at an earlier stage.
In 1993, Goldszmidt et al reported the case
of a 2.5-month-old male admitted to hospital due to an abdominal
mass (10). A routine blood test
showed that the patient presented with severe anemia, with a
hemoglobin level of 68 g/l and a reduced blood platelet count of
50,000/mm3. Ultrasonography showed that the mass was
retroperitoneal and heterogeneous. X-rays delineated the mass,
which distorted the duodenal loop and pressed forward against the
stomach. Surgery showed that the mass included the pancreas, the
root of mesentery and the extrahepatic bile duct. This mass was
biopsied and histological examination showed infantile-type HE.
Abdominal angiography showed that the mass was not particularly
hypervascularized, and there were no dilated supplying blood
vessels. The patient was administered methylprednisolone, but the
volume of the mass remained unchanged, while hepatosplenomegaly and
jaundice developed, and ultrasound showed dilated extra- and
intrahepatic biliary ducts. The patient was then administered
interferon-α2b for 1 month. Embolization of the small supplying
arteries was performed due to a lack of improvement after 1 week of
treatment. This procedure was followed by rapid disappearance of
the signs of consumption coagulopathy, a progressive improvement in
cholestasis and a decrease in the size of the mass (10).
In 2002, Lazure et al reported two cases of
pancreatic vascular tumor, one of which was kaposiform HE and
received tumor nourishing vascular embolization treatment with good
effects (4). The study suggested that
kaposiform HE has benign biological behaviors with a good
prognosis.
Wang et al reported the case of a 9-month old
infant with spindle cell HE of the pancreas in 2004 (10). Rapid intraoperative biopsy failed to
confirm the diagnosis and the surgeons failed to remove the tumor,
only employing interferon treatment after the pathological
diagnosis. The tumor size was reduced, the jaundice disappeared and
the follow-up visit showed good growth and development.
In 2006, Vogel et al collected 5,051 cases of
children with vascular abnormalities (including vascular tumor and
vascular malformations) who were treated at Boston Children's
Hospital (Boston, MA, USA) between 1994 and 2004. Of these cases, 6
involved the pancreas and only 1 case was of kaposiform HE
(2). The single case was in a male
patient with tumor invasion of the porta hepatis, gallbladder,
spleen, colon, omentum, mesentery and abdominal vascular
structures, including the superior mesenteric artery, renal artery
and celiac axis. The patient also presented with skin bruising and
severe thrombocytopenia, fitting KMS. MRI, CT, angiography,
colonoscopy and esophagogastroduodenoscopy (EGD) were used for the
pre-operative examination and diagnosis of the patient. Next,
systematic treatment was performed using corticosteroids and
vincristine. It was suggested that palliative procedures, such as
percutaneous drainage, stenting, and temporary or permanent bypass,
should be performed for biliary obstruction and jaundice, and
temporary or permanent bypass for intestinal obstruction.
Pancreatectomy, in a variety of forms, can be used for the
treatment of symptomatic lesions refractory to medical management
and following the inability to exclude malignancy.
In a retrospective study, Park et al reviewed
the clinical features and outcomes of all patients who were <18
years old with pancreatic neoplasms, and who were treated at Asan
Medical Center (Seoul, South Korea) between December 1994 and March
2010 (11). A total of 32 patients
were identified, but only 1 case of HE was found.
In the literature, only 9 patients have exhibited
pancreatic HE, with ages all but one under 1 year old, including 2
patients with KMS. The youngest was 2.5 months old, and the oldest
was 3 years old. In 1940, Kasabach and Merritt reported the case of
a newborn who exhibited rapidly increased hemangioma associated
with thrombocytopenic purpura. Successive associated cases have
been reported since that time. Researchers termed the systemic
features of the syndrome with giant hemangioma associated with
thrombocytopenia purpura as KMS (or hemangioma thrombocytopenia
syndrome). KMS includes the severe consumption of platelets, a
systemic bleeding tendency, an often acute onset and symptoms that
worsen progressively during the short term. Generally, KMS occurs
in children with giant hemangioma, while HE of the pancreas has a
small volume; the reason for the associated KMS is unknown. The 2
infant patient cases recorded in the literature exhibited rapidly
improved symptoms after the treatment, with hemorrhagic purpura
disappearing and platelet counts returning to normal.
As the patient in the present study did not have
symptoms such as skin vascular lesions or thrombocytopenia, it was
difficult to diagnose the disease based only on pre-operative MRI
and CT. Performing only percutaneous biliary drainage and drug
treatment could lead to a risk of misdiagnosis. Therefore, although
imaging results suggested that it would be hard to remove the
tumor, surgical exploration was chosen for the sake of a clear
diagnosis. As the tumor volume was large, severe oppression of the
CBD and duodenum were observed, causing complete biliary
obstruction and incomplete obstruction of the duodenum. Although
the intraoperative frozen biopsy suggested a benign tumor, the
tumor exhibited malignant biological behavior. As it surrounded the
root of the mesenteric vessels and portal vein, and was hard to
remove, only palliative surgery was considered. If only biliary
drainage was performed, the problem of incomplete duodenal
obstruction would not be solved. Thus, the final decision was made
to perform Whipple surgery (biliary-enteric reconstruction) and
retain the tumor. No post-operative medication, including hormones
or interferon, was used. Good growth and development of the patient
were observed for 6 months and the tumor exhibited a shrinking
tendency. However, the long-term outcome remains to be observed.
The prognosis may be good, but if the tumor grows gradually after
surgery and leads to biliary or intestine obstruction again,
certain medications such as corticosteroids or interferon may be
prescribed‥
In conclusion, childhood pancreas HE is extremely
rare and is a benign vascular tumor that mostly occurs in infants.
The tumor is likely to occur in the pancreatic head with oppression
of the extrahepatic bile duct, leading to extrahepatic bile duct
and duodenal obstruction. Formation of a clear diagnosis is
difficult by pre-operative examinations, such as MRI, CT and
angiography. Early surgical exploration and rapid frozen biopsy are
recommended. If the intraoperative diagnosis of HE is confirmed,
palliative surgery (biliary drainage) can relieve biliary
obstruction. Medications such as corticosteroids and interferon are
prescribed after the surgery; if the tumor is large with oppression
of the duodenum and invasion of retroperitoneal vessels, Whipple
surgery retaining the tumor can be performed.
References
|
1
|
Sauer L, Harrison MR, Bond SJ, Flake AW,
Heyman MB and Ring EJ: Long-term percutaneous biliary drainage in
an infant with hemangioendothelioma. J Pediatr Surg. 22:606–608.
1987. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vogel AM, Alesbury JM, Fox VL and Fishman
SJ: Complex pancreatic vascular anomalies in children. J Pediatr
Surg. 41:473–478. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mulliken JB, Fishman SJ and Burrows PE:
Vascular anomalies. Curr Probl Surg. 37:517–584. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lazure T, Tebboune N, Ben Lagha N, Triller
MF, Pariente D and Fabre M: Pancreatic vascular tumours of
childhood: A heterogeneous nosologic spectrum. Ann Pathol.
22:226–229. 2002.(In French). PubMed/NCBI
|
|
5
|
Villegas-Alvarez F and de Léon-Bojorge BY:
Hemangioendothelioma of the pancreas and choledochus, as a cause of
cholestatic neonatal and Kasabach-Merrit syndromes. Bol Med Hosp
Infant Mex. 46:672–675. 1989.(In Spanish). PubMed/NCBI
|
|
6
|
Villegas-Alvarez F and de Léon-Bojorge BY:
Hemangioendothelioma of the pancreas and choledochus, as a cause of
cholestatic neonatal and Kasabach-Merrit syndromes. Bol Med Hosp
Infant Mex. 46:672–675. 1989.(In Spanish). PubMed/NCBI
|
|
7
|
Chappell JS: Case reports. Benign
hemangioendothelioma of the head of the pancreas treated by
pancreaticoduodenectomy. J Pediatr Surg. 8:431–432. 1973.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Horie H, Iwasaki I, Iida H, Takizawa J,
Itoh F and Kohda S: Benign hemangioendothelioma of the pancreas
with obstructive jaundice. Acta Pathol Jpn. 35:975–979.
1985.PubMed/NCBI
|
|
9
|
Goldszmidt D, Pariente D, Yandza T,
Dubousset AM and Valayer J: Kasabach-Merritt syndrome with
pancreatic hemangioma in an infant. Arch Fr Pediatr. 50:593–597.
1993.(In French). PubMed/NCBI
|
|
10
|
Wang HP, Ge L and Yu SY: The treatment of
5 cases with pancreas tumors in children. Academic journal of
Shanghai Second Medical University. 24:691–692. 2004.(In
Chinese).
|
|
11
|
Park M, Koh KN, Kim BE, Im HJ, Kim DY and
Seo JJ: Pancreatic neoplasms in childhood and adolescence. J
Pediatr Hematol Oncol. 33:295–300. 2011. View Article : Google Scholar : PubMed/NCBI
|