Introduction
Glucagonoma is an uncommon neoplasm of the
pancreatic neuroendocrine islet α-cells, whereby the islet cells
secrete abundant glucagon (1). The
estimated annual incidence of glucagonoma is ~1 case per 20,000,000
individuals (2). Due to the rarity of
the disease, mortality rates remain unclear. In a study of 21
glucagonoma patients, Wermers et al (3) reported that nine patients succumbed to
the diease after a mean duration of 4.91 years following diagnosis
(3). Complete tumor resection may
cure glucagonoma, with a 10-year survival rate of 64.3% following
surgery, however, liver and lymph node metastasis are major risk
factors that contribute to tumor-associated mortality (4). For patients with unresectable advanced
disease, tumor debulking, chemotherapy or somatostatin may also be
considered to reduce the tumor-associated symptoms, however, the
survival benefit of such treatments is limited (2,3).
Glucagonoma induces various manifestations, which
are characterized by necrolytic migratory erythema (NME), diabetes
mellitus (DM), weight loss, anemia and neuropsychiatric
disturbances (1). NME represents the
most specific manifestation of glucagonoma syndrome and has
therefore provided the most valuable indications for diagnosis in
the majority of previous cases (5).
Early recognition of NME is likely to lead to a more rapid
diagnosis of glucagonoma, thereby allowing surgical resection and
achieving a promising therapeutic outcome. This study presents the
case of a glucagonoma patient who recovered following
spleen-preserving distal pancreatectomy.
Case report
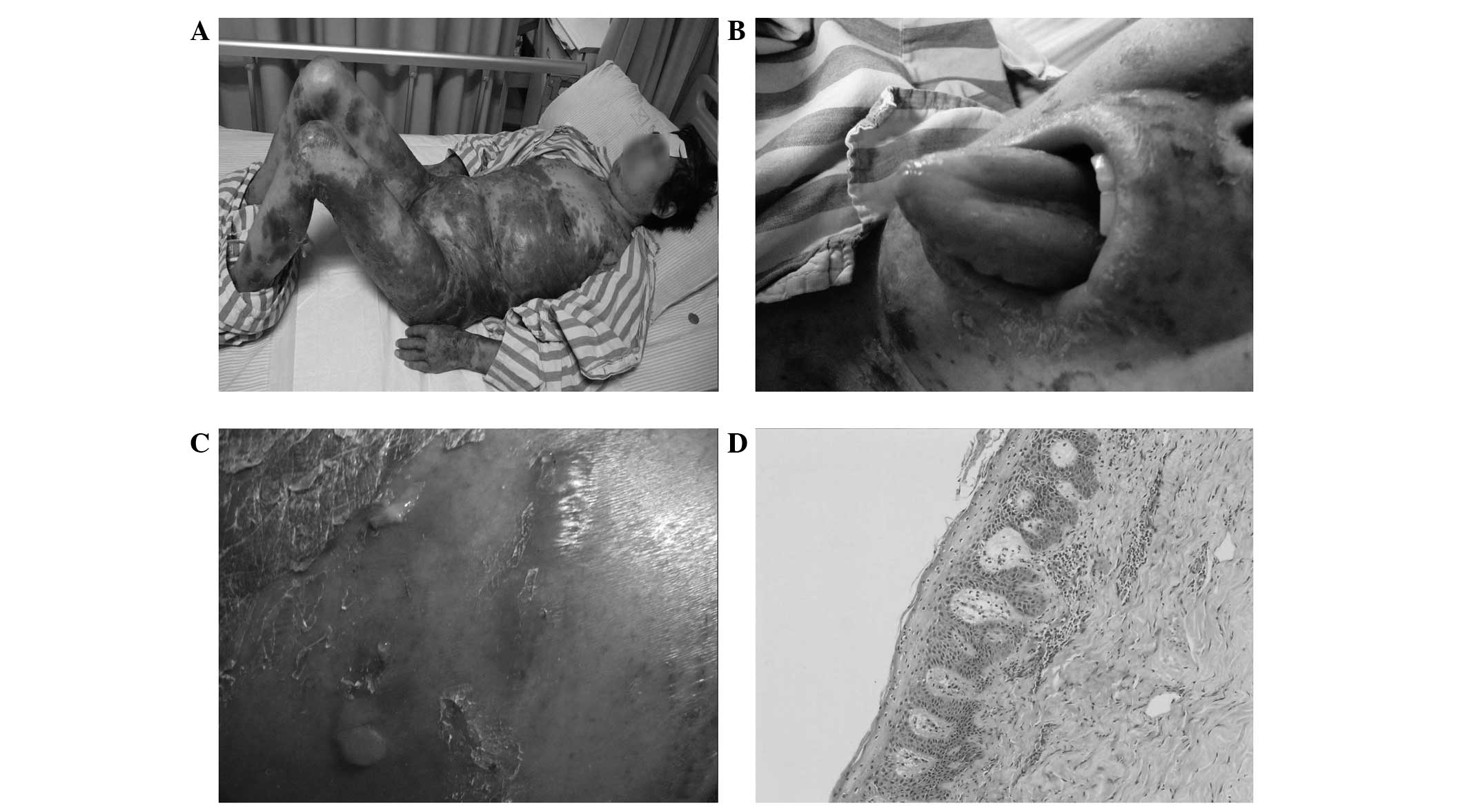
In November 2010, a 50-year-old female presented to
The Pancreas Center of Nanjing Medical University (Nanjing, China)
with a 2-year history of a pruritic and ulcerating skin rash, which
initially appeared at the waist and slowly progressed to the entire
body within three months (Fig. 1A).
Phacoscotasmus, cheilitis and glossitis were also present (Fig. 1B). The patient also complained of
blurred vision and weight loss of 5 kg. The patient was initially
diagnosed with pemphigus and treated with prednisone without relief
of the skin rash prior to her admission to our clinic. Physical
examination revealed that the skin lesions were erythematous
macules with erosions, serous exudate and crusting (Fig. 1C). A skin biopsy revealed that the
skin layers were arranged normally with mild skin keratosis, basal
pigmentation and perivascular infiltration of inflammatory cells in
the superficial skin (Fig. 1D).
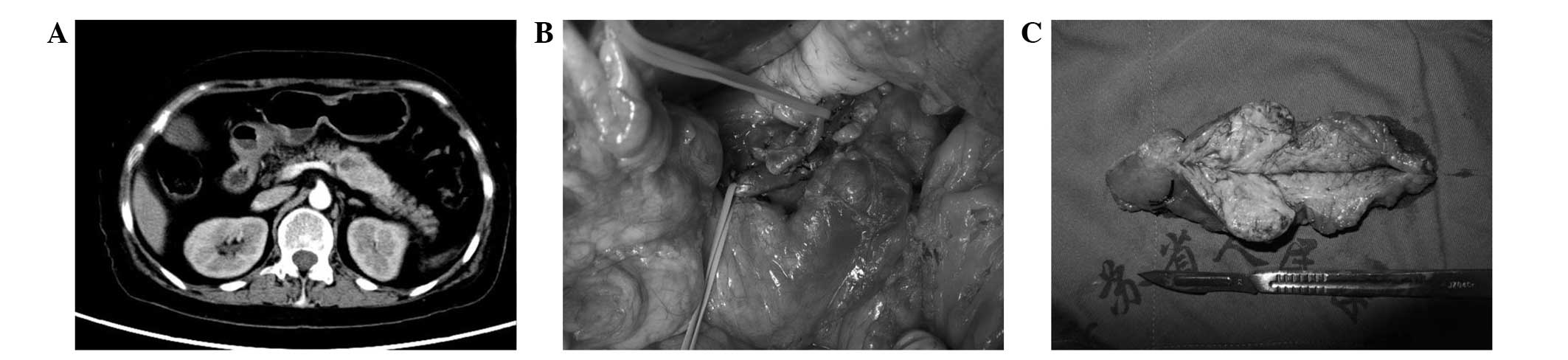
Laboratory tests indicated elevated blood glucose (maximum 18
mmol/l), anemia (87 g/l) and hypoproteinemia (24.6 g/l). Following
admission, the patient underwent abdominal computed tomography (CT)
scanning, which disclosed a pancreatic body mass with low density
(Fig. 2A). Given her history of the
skin rash, DM and the pancreatic mass, the patient's blood glucagon
concentration was measured, and her fasting glucagon level was
noted to be elevated, at 1132.20 pg/ml (normal, 0–80 pg/ml). The
patient was first treated with octreotide and intravenous amino
acid infusion. After the patient's nutrition was improved,
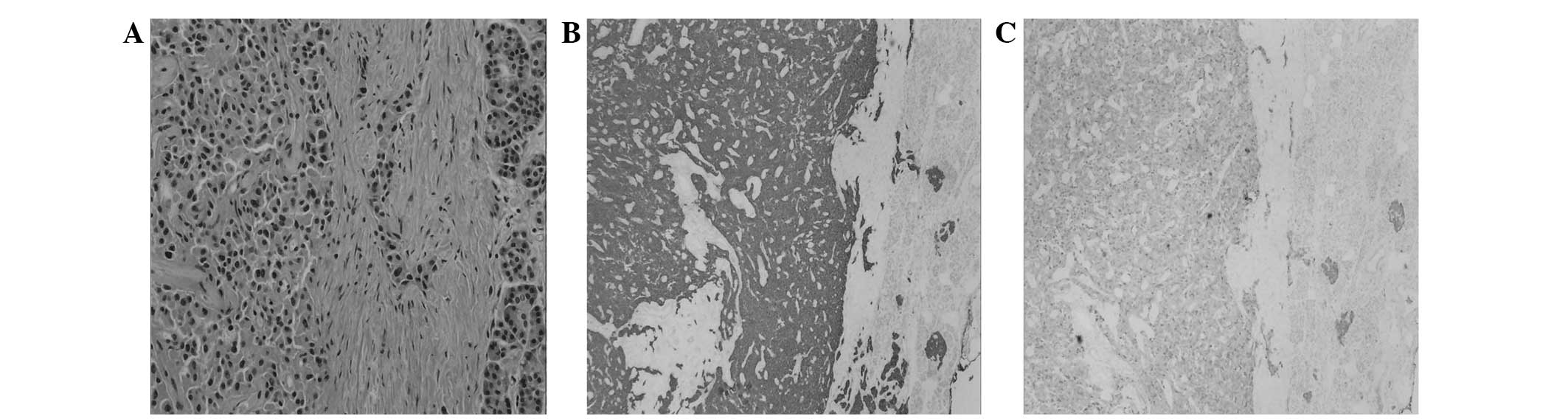
spleen-preserving distal pancreatectomy was performed (Fig. 2B and C). The skin lesions were
partially relieved following treatment with octreotide and
intravenous amino acid infusion, and gradually recovered following
surgery (Fig. 3A–C). Pathological
examination confirmed the diagnosis of glucagonoma (Fig. 4A) and immunohistochemical staining
revealed the positive staining of chromogranin and synaptophysin
(Fig. 4B and C). Four weeks
subsequent to discharge, the skin lesions were completely resolved
and blood glucose returned to normal. At 3-year follow-up, the
patient remained asymptomatic and no signs of recurrence were
detected. The patient provided written informed consent prior to
the publication of the study, and the study was approved by the
research ethics committee of The First Affiliated Hospital of
Nanjing Medical University (Nanjing, China).
Discussion
Glucagonoma, which accounts for 2% of islet cell
carcinomas, is a rare neuroendocrine pancreatic tumor with an
estimated incidence of one in 20 million (6). Although the diagnostic criteria for
glucagonoma has already been established by Stacpoole (7), its rare incidence has hampered prompt
diagnosis when the glucagonoma syndrome appears. To date, there are
fewer than 300 cases reported in the literature and the largest
case cohort included only 21 patients. Delayed diagnosis remains a
major issue in the treatment of glucagonoma. The median time
between the onset of glucagonoma syndrome and diagnosis is 3–4
years (3,5).
Oversecretion of glucagon by islet α-cells in tumors
contributes to the paraneoplastic phenomenon, namely glucagonoma
syndrome (5). Glucagon exhibits its
physiological functions by increasing the hepatic glucose output
and maintaining the blood glucose level (8). Glucagon also exerts a catabolic role by
attenuating protein synthesis (9).
The elevated glucagon secreted by glucagonoma results in amino acid
catabolism and serum glucose elevation, which are considered to be
responsible for skin lesions and DM (10). Glucagonoma syndrome consists of a
triad comprising glucagon-secreting tumors, DM and NME (11).
NME is considered to be the hallmark of glucagonoma
syndrome and is characterized by an annular pattern of erythema
with centrally formed fragile vesicles, bullae and crusts (2). It is present in ~65–70% of glucagonoma
cases at the point of diagnosis (12). Although a skin biopsy of NME offers
limited indications for the pathological diagnosis of glucagonoma,
its early recognition may lead to further CT scanning and establish
the diagnosis (13). It is worthy to
note that celiac disease, malabsorption, cirrhosis, malignancy and
pancreatitis may also present NME-like skin lesions, known as
pseudoglucagonoma syndrome (14). In
the present case, the NME had been misdiagnosed as immune pemphigus
and treated with corticosteroids for two years. Although the
corticosteroids treatments occasionally relieved the NME,
persistent elevated glucagon inevitably induced its recurrence. In
clinical practice, glucagonoma induced by NME should be considered
if the skin lesions remain following conventional treatments.
DM is a further clinical hallmark of glucagonoma.
Elevated glucagon levels promote the glucose output and antagonize
the effect of insulin. Although only 40% of glucagonoma patients
presented DM at the onset of symptoms, ~90% went on to develop it
(2). The severity of the diabetes
remains controversial in the literature, and NME usually occurs
prior to the emergence of the diabetes. In the present case, the
patient exhibited intermittent glucose elevation one and a half
years after the initiation of the skin rash, and the diabetes
resulted in the rapid damage of her lens.
Glucagonoma is a slow-growing and relatively
low-malignancy tumor. Although numerous glucagonoma patients suffer
due to a delayed diagnosis, the majority still benefit from tumor
resection. Metastasis represents the main prognostic factor for
glucagonoma. Half of all glucagonomas are metastatic at the time of
diagnosis (15). Patients without
metastasis achieve a 10-year survival rate of almost 100%, compared
with 51.6% of patients with metastasis (4). Synchronous resection of liver metastasis
or liver transplantation provides a favorable outcome (16,17).
Whether patients would benefit from tumor debulking or chemotherapy
remains to be elucidated (5,17). For localized glucagonoma, removal of
the tumor led to a notable improvement of the glucagonoma syndrome
within several days of surgery (18).
In the case of malnutrition, total parenteral nutrition with amino
acid and caloric supplementation may be used to counteract the
catabolic effects of high glucagon and reduce perioperative
complications (2). Moreover,
somatostatin analog may be useful in relieving glucagonoma syndrome
by inhibiting glucagon secretion or counteracting its effect
(19).
Although serum glucagon measurement and CT scanning
are capable of establishing diagnosis in most cases, the bridge
from glucagonoma syndrome to serum glucagon measurement and CT
scanning remains a major obstacle to early diagnosis. Few
clinicians suspect glucagonoma in its early stages due to its rare
incidence. Numerous patients suffer due to the delayed diagnosis
and may even miss out on the opportunity of curable resection. For
this rare tumor, optimization of the diagnostic procedure based on
glucagonoma syndrome is urgently needed.
Acknowledgements
This study was supported by the Research Special
Fund for Public Welfare of Health of China (201202007) and NSFC
(81272239).
References
|
1
|
Tseng HC, Liu CT, Ho JC and Lin SH:
Necrolytic migratory erythema and glucagonoma rising from
pancreatic head. Pancreatology. 13:455–457. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chastain MA: The glucagonoma syndrome: a
review of its features and discussion of new perspectives. Am J Med
Sci. 321:306–320. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wermers RA, Fatourechi V, Wynne AG, Kvols
LK and Lloyd RV: The glucagonoma syndrome. Clinical and pathologic
features in 21 patients. Medicine (Baltimore). 75:53–63. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Soga J and Yakuwa Y:
Glucagonomas/diabetico-dermatogenic syndrome (DDS): a statistical
evaluation of 407 reported cases. J Hepatobiliary Pancreat Surg.
5:312–319. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Eldor R, Glaser B, Fraenkel M, Doviner V,
Salmon A and Gross DJ: Glucagonoma and the glucagonoma syndrome -
cumulative experience with an elusive endocrine tumour. Clin
Endocrinol (Oxf). 74:593–598. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lo CH, Ho CL and Shih YL: Glucagonoma with
necrolytic migratory erythema exhibiting responsiveness to
subcutaneous octreotide injections. QJM. 107:157–158. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stacpoole PW: The glucagonoma syndrome:
clinical features, diagnosis and treatment. Endocr Rev. 2:347–361.
1981. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lefèbvre PJ: Glucagon and its family
revisited. Diabetes Care. 18:715–730. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Charlton MR, Adey DB and Nair KS: Evidence
for a catabolic role of glucagon during an amino acid load. J Clin
Invest. 98:90–99. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
van Beek AP, de Haas ER, van Vloten WA,
Lips CJ, Roijers JF and Canninga-van Dijk MR: The glucagonoma
syndrome and necrolytic migratory erythema: a clinical review. Eur
J Endocrinol. 151:531–537. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shi W, Liao W, Mei X, Xiao Q, Zeng Y and
Zhou Q: Necrolytic migratory erythema associated with glucagonoma
syndrome. J Clin Oncol. 28:e329–e331. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Remes-Troche JM, Garcia-de-Acevedo B,
Zuniga-Varga J, Avila-Funes A and Orozco-Topete R: Necrolytic
migratory erythema: a cutaneous clue to glucagonoma syndrome. J Eur
Acad Dermatol Venereol. 18:591–595. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kheir SM, Omura EF, Grizzle WE, Herrera GA
and Lee I: Histologic variation in the skin lesions of the
glucagonoma syndrome. Am J Surg Pathol. 10:445–453. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mullans EA and Cohen PR: Iatrogenic
necrolytic migratory erythema: a case report and review of
nonglucagonoma-associated necrolytic migratory erythema. J Am Acad
Dermatol. 38:866–873. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yao JC, Eisner MP, Leary C, Dagohoy C,
Phan A, Rashid A, Hassan M and Evans DB: Population-based study of
islet cell carcinoma. Ann Surg Oncol. 14:3492–3500. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Radny P, Eigentler TK, Soennichsen K,
Overkamp D, Raab HR, Viebahn R, Mueller-Horvart C, Sotlar K and
Rassner G: Metastatic glucagonoma: treatment with liver
transplantation. J Am Acad Dermatol. 54:344–347. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Poggi G, Villani L and Bernardo G:
Multimodality treatment of unresectable hepatic metastases from
pancreatic glucagonoma. Rare Tumors. 1:e62009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Smith AP, Doolas A and Staren ED: Rapid
resolution of necrolytic migratory erythema after glucagonoma
resection. J Surg Oncol. 61:306–309. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Elsborg L and Glenthoj A: Effect of
somatostatin in necrolytic migratory erythema of glucagonoma. Acta
Med Scand. 218:245–249. 1985. View Article : Google Scholar : PubMed/NCBI
|