Introduction
Lacrimal gland tumours are uncommon. The most common
type of malignant lacrimal gland tumour are epithelial tumours,
including adenoid cystic carcinoma, which are responsible for 58%
of all malignant tumours in the lacrimal gland (1). Metastases to the lacrimal gland are rare
(2) and only sporadic cases have
previously been reported. The gland may also be a site of direct
invasion from a neighbouring tumour (3).
Breast cancer is considered one of the most frequent
solid tumours to metastasize to the eye region (4,5). However,
only one previous report has described breast cancer metastasizing
to the lacrimal gland (2). Breast
cancer metastasis to the salivary gland, to which the lacrimal
gland is often compared, is considered markedly more common
(6).
The present study reports two cases of metastases to
the lacrimal gland from breast cancer, presenting with massive
proptosis and a poor prognosis. Written informed consent for the
publication of this report was obtained from each patient or their
family.
Case report
Case 1
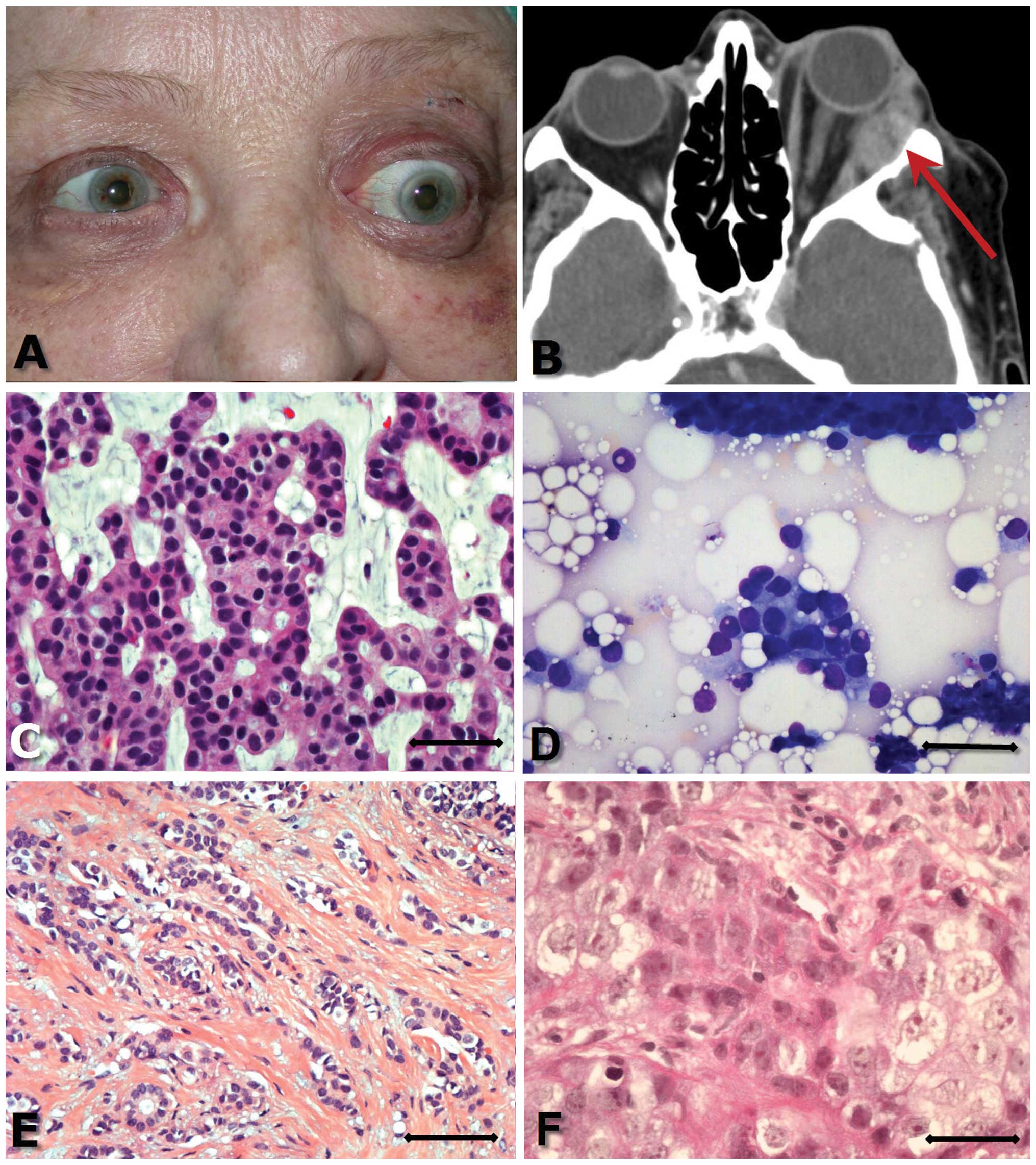
A 77-year-old female was referred to the
ophthalmological department with a suspected retrobulbar tumour,
due to a rapidly (2–3 months) progressing left-sided proptosis
(Fig. 1A).
Examination revealed a proptosis of 11 mm,
accompanied by increased retrobulbar resistance. Eye motility was
reduced and when looking up and to the left the patient complained
of diplopia. The skin over the temporal orbital border was
thickened but without palpable tumour. Visual acuity was 6/60 in
the right eye and 1/60 in the left eye. The intraocular pressure
was 20 mmHg in the right eye and 29 mmHg in the left eye. A
computed tomography (CT) scan revealed a 4-cm tumour located
laterally and superiorly to the left eyeball. The tumour
infiltrated the lateral and superior rectus muscle, and eroded the
lateral orbital wall and roof (Fig.
1B). The tumour had spread intracranially to the frontal region
of the brain and had a 1 cm bone metastasis in the frontal region
of the cranium. A bone scintigraphy revealed multiple pathological
areas of increased activity, which explained the skeletal pain the
patient had experienced.
An incisional biopsy of the lacrimal gland tumour
was performed.
Eleven years previously a mammography had identified
a dense area with microcalcifications in the upper lateral quadrant
of the patient's left breast. There was no palpable process. The
patient refused treatment. A further mammography conducted three
months later demonstrated growth of the tumour and fine needle
aspiration revealed malignant tumour cells. Growth of the tumour
was monitored during the next five years by control mammographies
and ultrasound. During these years a fine needle aspiration
revealed an invasive ductal carcinoma. The patient still refused
treatment and no further mammographies or clinical control measures
were performed.
Following diagnosis of the orbital metastasis the
patient received palliative radiotherapy ten times towards the left
eye resulting in a cumulative subdosis of 29 Gy. The patient died
nine months following first contact with the ophthalmological
department.
Case 2
A 69-year-old female was referred due to proptosis
of the right eye, which had developed over three weeks. Clinical
examination revealed proptosis of 5 mm, oedema of the right upper
eyelid and ptosis. Movement capabilities of the right eye were
significantly reduced when the patient looked up, and slightly
reduced abduction and adduction were observed. A tumour could be
palpated supero-temporally in the right orbit at the site of the
lacrimal gland and extending laterally. The tumour was adherent to
the neighbouring structures. Visual acuity was 0.8 in the right eye
and 1.0 in the left eye. A magnetic resonance imaging scan revealed
a 1×2×3 cm tumour proximal to the lacrimal gland. A biopsy of the
lacrimal gland tumour was performed.
A bone scintigraphy demonstrated multiple areas of
increased activity and an abdominal ultrasound identified a focal
process in the liver. A liver biopsy revealed breast cancer
metastasis.
One year previously, the patient had been diagnosed
with a tumour in the left breast. The tumour was 0.5 cm in diameter
and localised proximal to the areola. An ultrasound guided biopsy
(including fine needle aspiration as well as core biopsy) was
conducted and microscopy revealed an invasive ductal carcinoma. A
mastectomy was performed and ten axillary lymph nodes were removed.
Histological examination demonstrated the carcinoma to be oestrogen
receptor positive.
Following diagnosis of the orbital tumour the
patient received radiotherapy (3 Gy x10), and a cycle of
cyclofosfamid 1200 mg, Methotrexat 95 mg and 5-fluoracil 1200 mg
was administered. The radiation therapy reduced the swelling around
the eye, proptosis was reduced to 2 mm and normal movement of the
eye was regained. However, the patient was not well enough to
receive the second series of chemotherapy. Shortly prior to death,
the patient commenced treatment with Tamoxifen based on an estrogen
receptor-positive breast cancer. The patient died three months
following referral to the eye department.
Histopathology
The applied antibodies are listed in Table I. The breast tumour smear from patient
one was only stained with haematoxylin and eosin and an antibody
against oestrogen receptors due to the small specimen sample
available.
 | Table I.Immunohistochemical analysis of
lacrimal gland tumours and ductal breast carcinomas of patients 1
and 2. |
Table I.
Immunohistochemical analysis of
lacrimal gland tumours and ductal breast carcinomas of patients 1
and 2.
|
| Patient 1 | Patient 2 |
|
|---|
|
|
|
|
|
|---|
| Immunohistochemical
marker | Lacrimal gland
tumour | Ductal breast
carcinoma | Lacrimal gland
tumour | Ductal breast
carcinoma | Breast carcinoma
staining pattern in literature, (ref) |
|---|
| Pan-CK
1–8,10,14–16,18,19 | + | | + | + | Positive (7,8) |
| CEA | + | | (+) | (+) | 45–58% (9) |
| EMA | + | | + | + | 93% (10) |
| ER | + | – | (+) | + | 70–80% (7,11,12) |
| GCDFP-15 | + | | – | (+) | 50–74% (7,12) |
| GFA | (+) | | – | – | 7% (13) |
| HER-2 | – | | – | – | 15–20% (14) |
| Mammaglobin A | – | | – | – | 23–47% (15) |
| PR | – | | – | – | 54–70% (7,11,12) |
| S100 | – | | – | – | 10–45% (7,8,12,14) |
| SMA | – | | – | – | Negative (7) |
| Vimentin | – | | – | – | 64% (16) |
Microscopy
Case 1
Biopsy from the lacrimal gland revealed an
epithelial tumour tissue with a cribriform growth pattern
containing ductal elements (Fig. 1C).
There were scattered lumina in the epithelial clusters. The
epithelial cells appeared well differentiated and there was no
invasion into the surrounding stromal tissue. Few mitoses were
observed. The background was mucinous and stained positive with
Alcian blue. Immunohistochemistry indicated a positive reaction for
pan-cytokeratin (CK), estrogen receptor, epithelial membrane
antigen (EMA), carcinoembryonic antigen (CEA) and gross cystic
disease fluid protein 15 (GCDFP-15). There was variable staining
for glial fibrillary acidic protein but the tumour cells were
negative for progesterone, human epidermal growth factor receptor 2
(HER-2) and mammaglobin.
Fine needle aspiration from the tumour in the left
breast revealed epithelial cells with slight pleomorphism, arranged
in groups or as single cells. There were no myoepithelial cells,
but in certain areas mucoid material was identified (Fig. 1D).
The cytology of the breast tumour and the histology
of the lesion in the lacrimal gland were consistent with a
diagnosis of an invasive ductal, partly mucinous, breast carcinoma
with metastasis to the lacrimal gland.
Case 2
The lacrimal gland tumour consisted of closely
arranged areas of glandular epithelial tumour islands of varying
size, surrounded by sparse collagenous stroma containing a
proportion of inflammatory cells. The tumour cells were pleomorphic
with a lightly eosinophilic cytoplasm and nuclei with prominent
nucleoli (Fig. 1F). There were small
necroses, and mitotic figures were identifiable.
Immunohistochemistry revealed a positive reaction for pan-CK, EMA
and oestrogen receptor, variable positivity for CEA and a negative
reaction for GCDFP-15, progesterone, HER-2 and mammaglobin.
The breast tumour was an invasive ductal carcinoma,
comprised of cells with moderate pleomorphism, arranged in small,
solid clusters or trabeculi (Fig.
1E). The eosinophilic or clear cytoplasm was moderate to
abundant. Focally, an in situ component was demonstrated.
Immunohistochemically, the tumour was found to be positive for EMA
and estrogen receptor, with variable positivity for pan-CK, CEA and
GCDFP-15 and negative reaction for progesterone, HER-2 and
mammaglobin.
Due to the similar morphology and
immunohistochemical profile, the tumour in the lacrimal gland was
regarded as a metastasis from the ductal carcinoma of the
breast.
Discussion
The two patients in the present study presented with
ptosis, increased retrobulbar resistance, diplopia, reduced eye
movement and proptosis. All of these findings are typical of
primary, as well as secondary, lacrimal gland tumours (23). Malignant lacrimal gland tumours
typically induce symptoms six months following development
(24), although this was even more
rapid in the present cases of metastasis.
In addition to histology, histochemistry and
immunohistochemistry are able to aid clarification of the diagnosis
of breast cancer metastasis. However, there is no single specific
marker that may reliably diagnose a breast cancer metastasis. The
importance of establishing the correct diagnosis is important due
to the varying treatment modalities of breast cancer metastases
(25).
GCDFP-15 and mammaglobin have been considered to be
specific markers of breast carcinomas. GCDFP-15 is regarded to have
high specificity, whereas mammaglobin has a high sensitivity
(26). A combination of GCDFP-15 and
mammaglobin staining is recommended for the diagnosis of metastatic
breast cancer (14,27). When possible, it is also preferable to
compare the primary breast tumour to the suspected metastasis. In
the two present cases, GCDFP-15 was variably positive and the
metastases were mammaglobin negative.
The CK panel used in the present study consisted of
CK 1–8, 10, 14–16, 18 and 19. In normal breast tissue the luminal
cells express CK 7, 8, 18 and 19 and the basal cells express CK
5/6, 14 and 17 (7,14). In lacrimal glands the secretory and
basal ductal cells have also been found to be CK 7, 8, 18 and 19
positive (28). Therefore, it is not
possible to differentiate between a primary epithelial lacrimal
gland tumour and a metastasis from a ductal breast carcinoma using
CKs.
The lacrimal gland is often compared to the salivary
gland due to their shared embryonic origins. In the salivary gland
1–8% of all malignancies are found to be metastatic tumours
(29,30). Tumours in the salivary glands are
markedly more common than those in the lacrimal gland, and there
are more metastases to the salivary glands than to the lacrimal
glands (31). A plausible explanation
for this phenomenon is the presence of lymph nodes in the salivary
glands, in contrast to the lacrimal gland. The spread of breast
cancer to the salivary glands may therefore occur by haematogenous
or lymphatic spread. Metastases to the sublingual gland, which is
also without lymph nodes, has never been reported (31).
Consideration should also be given to
metastasis-associated genes, where a specific genetic profile may
increase the risk of organ-specific metastasis (32).
The general treatment of breast cancer and breast
cancer metastases is individualised and may consist of surgery,
radiation and systemic therapy (33,34).
Depending on the initial stage, tumour biology and primary
treatment strategy, 20–85% of patients diagnosed with early breast
cancer will later develop recurrent and/or metastatic breast cancer
(33). The two patients in the
present study received radiotherapy and patient two also received
chemotherapy and, shortly prior to mortality, began treatment with
Tamoxifen.
Metastases to the lacrimal gland are rare (Table II). The present cases demonstrate
that the clinician should consider breast cancer metastasis in the
differential diagnosis of lacrimal gland tumours, particularly if
symptoms develop rapidly. Such lacrimal gland metastases may be
histologically difficult to differentiate from other epithelial
lacrimal gland tumours. The results of the present study draw
attention to breast cancer being one of the most frequent causes of
metastasis to the lacrimal gland.
| Table II.Previously reported metastases to the
lacrimal gland. |
Table II.
Previously reported metastases to the
lacrimal gland.
| Tumour type | Gender | Age, years | Treatment | Reference | Publication |
|---|
| Breast
carcinoma | – | – | – | (2) | 1998 A |
| Breast
carcinoma | – | – | – | (2) | 1998 B |
| Breast
carcinomaa | Female | 77 | Radiotherapy | Present case 1 |
|
| Breast
carcinomaa | Female | 69 | Radiotherapy,
Tamoxifen | Present case 2 |
|
| Carcinoid | – | – | – | (17) | 1982 |
| Carcinoid,
ileum | Male | 51 | Resection | (18) | 1956 |
| Carcinoid,
mediastinum | Male | 82 | Surgery | (19) | 1989 |
| Renal cell
carcinoma | Male | 59 | Surgery | (20) | 1999 |
| Renal cell
carcinoma | Male | 65 | Surgery | (21) | 1986 |
| Thyroid
carcinoma | Female | 56 |
| (22) | 1990 |
| Unknown | – | – | – | (2) | 1998 |
Acknowledgements
The authors would like to thank Søren Daugaard
(Department of Pathology, Rigshospitalet, University of Copenhagen,
Denmark) for his valuable comments. The present study was supported
by The Danish Eye Research Foundation, The Danish Eye Health
Society, Synoptik-Fonden, Købmand Kristjan Kjær and wife Magrethe
Kjær's Foundation, Kleinsmed Svend Helge Arvid Schrøder and wife
Ketty Lydia Larsen Schrøder's Foundation, DMSc Alfred Helsted and
wife DMSc Eli Møller's Foundation and Engineer August Fredrik
Wedell Erichsen's Foundation.
References
|
1
|
von Holstein SL, Therkildsen MH, Prause
JU, Stenman G, Siersma VD and Heegaard S: Lacrimal gland lesions in
Denmark between 1974 and 2007. Acta Ophthalmol. 91:349–354. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Font RL, Smith SL and Bryan RG: Malignant
epithelial tumors of the lacrimal gland: A clinicopathologic study
of 21 cases. Arch Ophthalmol. 116:613–616. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Font RL, Croxatto JO and Rao NA: Tumors of
the lacrimal glandTumors of the Eye and Ocular Adnexa. 4th.
American Registry of Pathology/Armed Forces Institute of Pathology;
Washington: pp. 223–246. 2006
|
|
4
|
Mejía-Novelo A, Alvarado-Miranda A,
Morales-Vázquez F, Gamboa-Vignole C, Núñez-Gómez R, Castañeda-Soto
N, Dueñas-González A, Candelaria-Hernández M and Lara-Medina F:
Ocular metastases from breast carcinoma. Med Oncol. 21:217–221.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mennel RG: Ocular metastases from breast
cancer. Clin Breast Cancer. 1:318–319. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Löning T and Jäkel KT: Tumours of the
salivary glands - secondary tumoursWorld Health Organization
Classification of Tumours: Pathology and Genetics, Head and Neck
Tumours. Barnes L, Eveson JW, Reichart P and Sidransky D: IARC
Press; Lyon: pp. 2812005
|
|
7
|
Yeh IT and Mies C: Application of
immunohistochemistry to breast lesions. Arch Pathol Lab Med.
132:349–358. 2008.PubMed/NCBI
|
|
8
|
Hicks DG: Immunohistochemistry in the
diagnostic evaluation of breast lesions. Appl Immunohistochem Mol
Morphol. 19:501–505. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mauri FA, Caffo O, Veronese S, Verderio P,
Boracchi P, Bonzanini M, Rossi N, Perrone G, Dalla Palma P and
Barbareschi M: Tissue carcinoembryonic antigen and oestrogen
receptor status in breast carcinoma: An immunohistochemical study
of clinical outcome in a series of 252 patients with long-term
follow-up. Br J Cancer. 77:1661–1668. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
van der Vegt B, de Roos MA, Peterse JL,
Patriarca C, Hilkens J, de Bock GH and Wesseling J: The expression
pattern of MUC1 (EMA) is related to tumour characteristics and
clinical outcome of invasive ductal breast carcinoma.
Histopathology. 51:322–335. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ellis IO, Schnitt SJ, Sastre-Garau X,
Bussolati G, Tavassoli FA, Eusebi V, et al: Tumours of the
breastTumours of the Breast and Female Genital Organs. Tavassol FA
and Devilee P: IARC Press; Lyon: pp. 9–112. 2003
|
|
12
|
Lee AH: Use of immunohistochemistry in the
diagnosis of problematic breast lesions. J Clin Pathol. 66:471–477.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gould VE, Koukoulis GK, Jansson DS, Nagle
RB, Franke WW and Moll R: Coexpression patterns of vimentin and
glial filament protein with cytokeratins in the normal,
hyperplastic, and neoplastic breast. Am J Pathol. 137:1143–1155.
1990.PubMed/NCBI
|
|
14
|
Bhargava R, Esposito N and Dabbs DJ:
Immunohistology of the breastDiagnostic Immunohistochemistry
Theranostic and Genomic Applications. 3rd. Dabbs DJ: Elsevier
Saunders; Philadelphia: pp. 763–819. 2010
|
|
15
|
Watson MA and Fleming TP: Mammaglobin, a
mammary-specific member of the uteroglobin gene family, is
overexpressed in human breast cancer. Cancer Res. 56:860–865.
1996.PubMed/NCBI
|
|
16
|
Raymond WA and Leong AS: Co-expression of
cytokeratin and vimentin intermediate filament proteins in benign
and neoplastic breast epithelium. J Pathol. 157:299–306. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Divine RD, Anderson RL and Ossoinig KC:
Metastatic carcinoid unresponsive to radiation therapy presenting
as a lacrimal fossa mass. Ophthalmology. 89:516–520. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Font RL and Ferry AP: Carcinoma metastatic
to the eye and orbit III. A clinicopathologic study of 28 cases
metastatic to the orbit. Cancer. 38:1326–1335. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Harris DC, Clark CV and Bartholomew RS:
Carcinoid tumour in the lacrimal gland. Doc Ophthalmol. 73:43–51.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shields JA, Shields CL, Eagle RC Jr, Singh
AD and Armstrong T: Metastatic renal cell carcinoma to the
palpebral lobe of the lacrimal gland. Ophthal Plast Reconstr Surg.
17:191–194. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Denby P, Harvey L and English MG: Solitary
metastasis from an occult renal cell carcinoma presenting as a
primary lacrimal gland tumour. Orbit. 5:21–24. 1986. View Article : Google Scholar
|
|
22
|
Bernstein-Lipschitz L, Lahav M, Chen V,
Gutman I, Gal R and Lipschitz M: Metastatic thyroid carcinoma
masquerading as lacrimal gland tumor. Graefes Arch Clin Exp
Ophthalmol. 228:112–115. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ni C, Cheng SC, Dryja TP and Cheng TY:
Lacrimal gland tumors: A clinicopathological analysis of 160 cases.
Int Ophthalmol Clin. 22:99–120. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lee DA, Campbell RJ, Waller RR and Ilstrup
DM: A clinicopathologic study of primary adenoid cystic carcinoma
of the lacrimal gland. Ophthalmology. 92:128–134. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lewis JE, McKinney BC, Weiland LH,
Ferreiro JA and Olsen KD: Salivary duct carcinoma.
Clinicopathologic and immunohistochemical review of 26 cases.
Cancer. 77:223–230. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chia SY, Thike AA, Cheok PY and Tan PH:
Utility of mammaglobin and gross cystic disease fluid protein-15
(GCDFP-15) in confirming a breast origin for recurrent tumors.
Breast. 19:355–359. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bhargava R and Dabbs DJ: Use of
immunohistochemistry in diagnosis of breast epithelial lesions. Adv
Anat Pathol. 14:93–107. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kivelä T: Antigenic profile of the human
lacrimal gland. J Histochem Cytochem. 40:629–642. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lussier C, Klijanienko J and Vielh P:
Fine-needle aspiration of metastatic nonlymphomatous tumors to the
major salivary glands: A clinicopathologic study of 40 cases
cytologically diagnosed and histologically correlated. Cancer.
90:350–356. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Seifert G, Hennings K and Caselitz J:
Metastatic tumors to the parotid and submandibular glands -
analysis and differential diagnosis of 108 cases. Pathol Res Pract.
181:684–692. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Eveson JW, Auclair P, Gnepp DR and
El-Naggar AK: Tumours of the salivary glands: IntroductionWorld
Health Organization Classification of Tumours: Pathology and
Genetics, Head and Neck Tumours. Barnes L, Eveson JW, Reichart P
and Sidransky D: IARC Press; Lyon: pp. 212–215. 2005
|
|
32
|
Minn AJ, Gupta GP, Siegel PM, Bos PD, Shu
W, Giri DD, Viale A, Olshen AB, Gerald WL and Massagué J: Genes
that mediate breast cancer metastasis to lung. Nature. 436:518–524.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bernard-Marty C, Cardoso F and Piccart MJ:
Facts and controversies in systemic treatment of metastatic breast
cancer. Oncologist. 9:617–632. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Roché H and Vahdat LT: Treatment of
metastatic breast cancer: Second line and beyond. Ann Oncol.
22:1000–1010. 2011. View Article : Google Scholar : PubMed/NCBI
|