Introduction
Gastrointestinal stromal tumors (GISTs) are rare
neoplasms with an estimated prevalence of 10–14 per 1,000,000.
GISTs are mesenchymal tumors of the gastrointestinal tract, which
occur most frequently in the stomach (60%) and small intestine
(30%), and are less frequently observed in the rectum (4%), colon
and appendix (1–2%), and duodenum (4–5%). In rare cases, GISTs may
occur outside of the gastrointestinal tract, including in the
greater omentum and mesentery (1,2). All GISTs
are currently regarded to be potentially malignant, with varying
degrees of malignancy. GISTs in the mesentery and the small
intestine are more aggressive than those at other sites, and have a
higher degree of malignancy and poorer prognosis than GISTs of the
stomach (3). A comprehensive
treatment strategy, including surgery, radiofrequency ablation
(RFA) and imatinib mesylate therapy, is effective in treating liver
metastases (4). RFA has also been
reported to be an effective treatment modality for
imatinib-resistant GIST with liver metastases (5). The present study describes a case of
mesenteric GIST with 27 liver metastases, which was successfully
treated by RFA combined with surgical resection and imatinib; this
is the greatest number of tumors treated with the most RFA sessions
for GISTs reported to date. Written informed consent was obtained
from the patient.
Case report
A 47-year-old female was admitted to Southwest
Hospital, Third Military Medical University (Chongqing, China) on
April 13, 2011, 1 year following surgical treatment for stromal
tumors of the small intestinal mesentery. Prior to this admission,
resection of small bowel mesenteric stromal tumors, and subtotal
resection of the jejunum and intestinal anastomosis had been
performed at the Department of Gastrointestinal Surgery, The
Affiliated Hospital of Zunyi Medical College (Zunyi, China) on 27th
April, 2010. The surgery had revealed a tumor of ~18×15
cm2 in size, located inside the mesentery in the upper
jejunal segment. Postoperative pathological examination confirmed a
diagnosis of stromal tumors of the small bowel mesentery. For
financial reasons, the patient had declined imatinib mesylate or
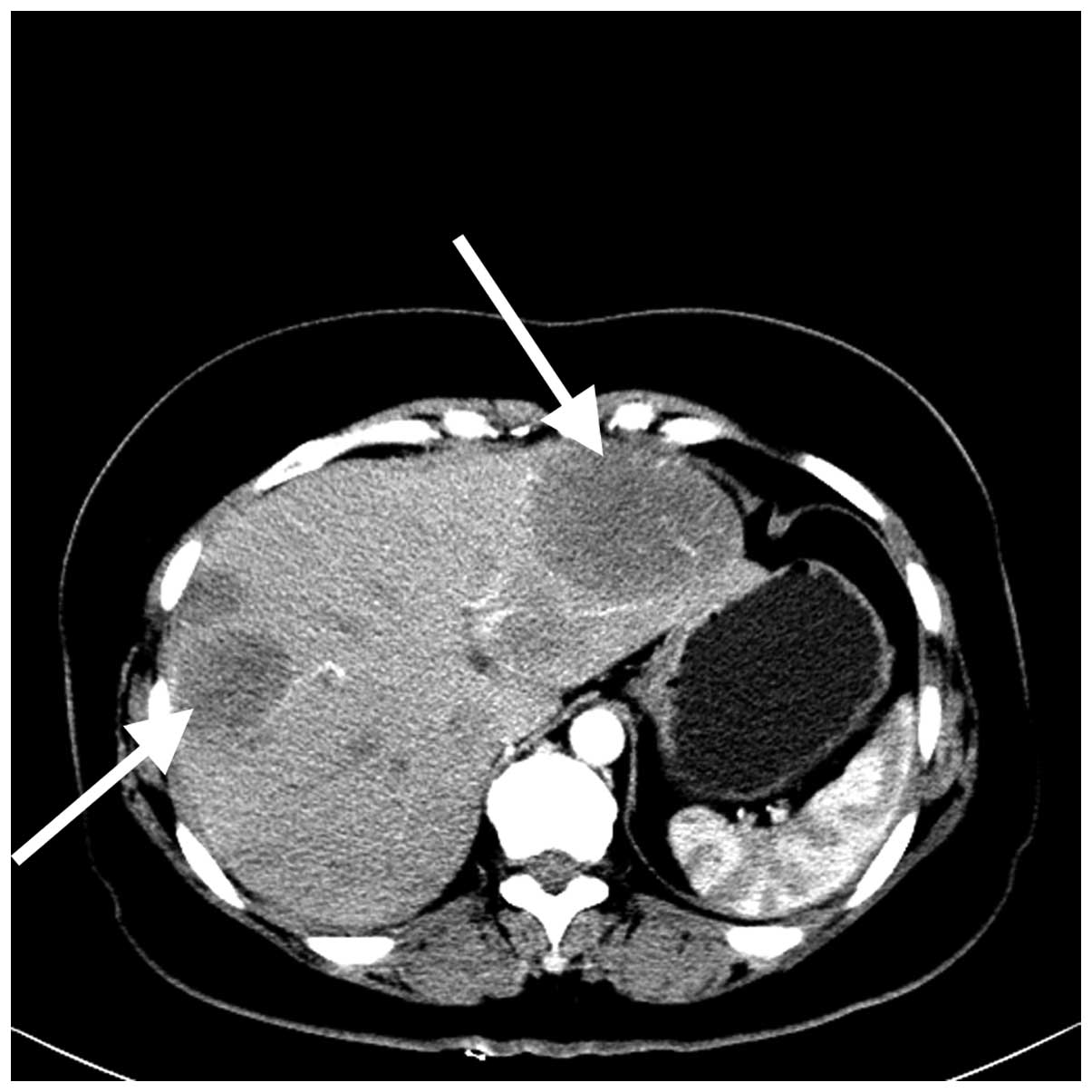
other molecular-targeted therapies following surgery. After 1 year,
color Doppler ultrasonography and enhanced computed-tomography (CT)
imaging revealed multiple solid, space-occupying lesions in the
liver as a result of routine follow-up (Fig. 1). These findings, in combination with
the patient's history of GIST, indicated a diagnosis of liver
metastases.
In May 2011, subtotal resection of the left liver
and intraoperative ultrasound-guided RFA of four metastases in the
right liver were conducted with the patient under general
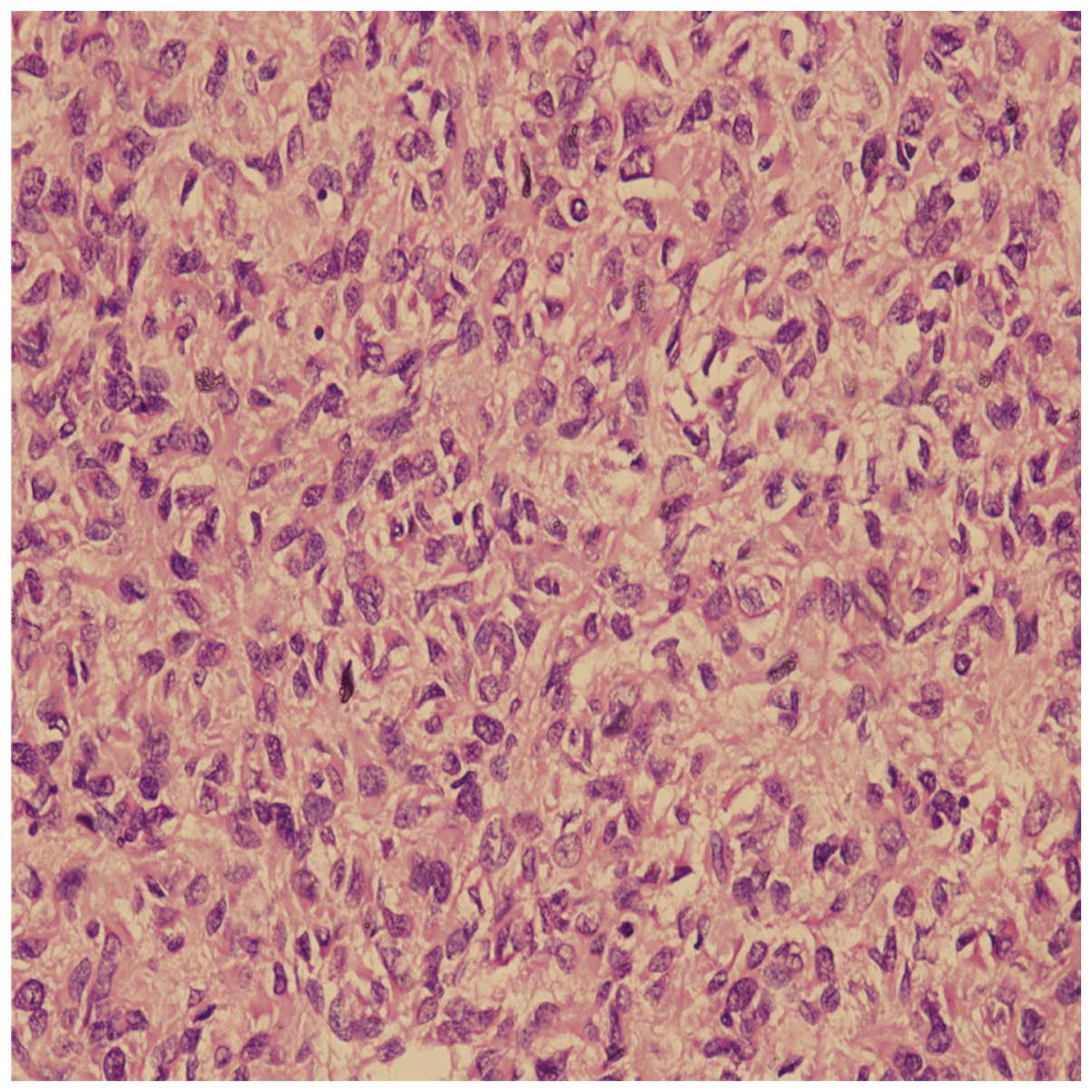
anesthesia. The postoperative pathological examination revealed
predominantly fusiform tumor cells (Fig.
2) and six mitoses per 50 high power fields, confirming a
diagnosis of malignant stromal tumors in the liver.
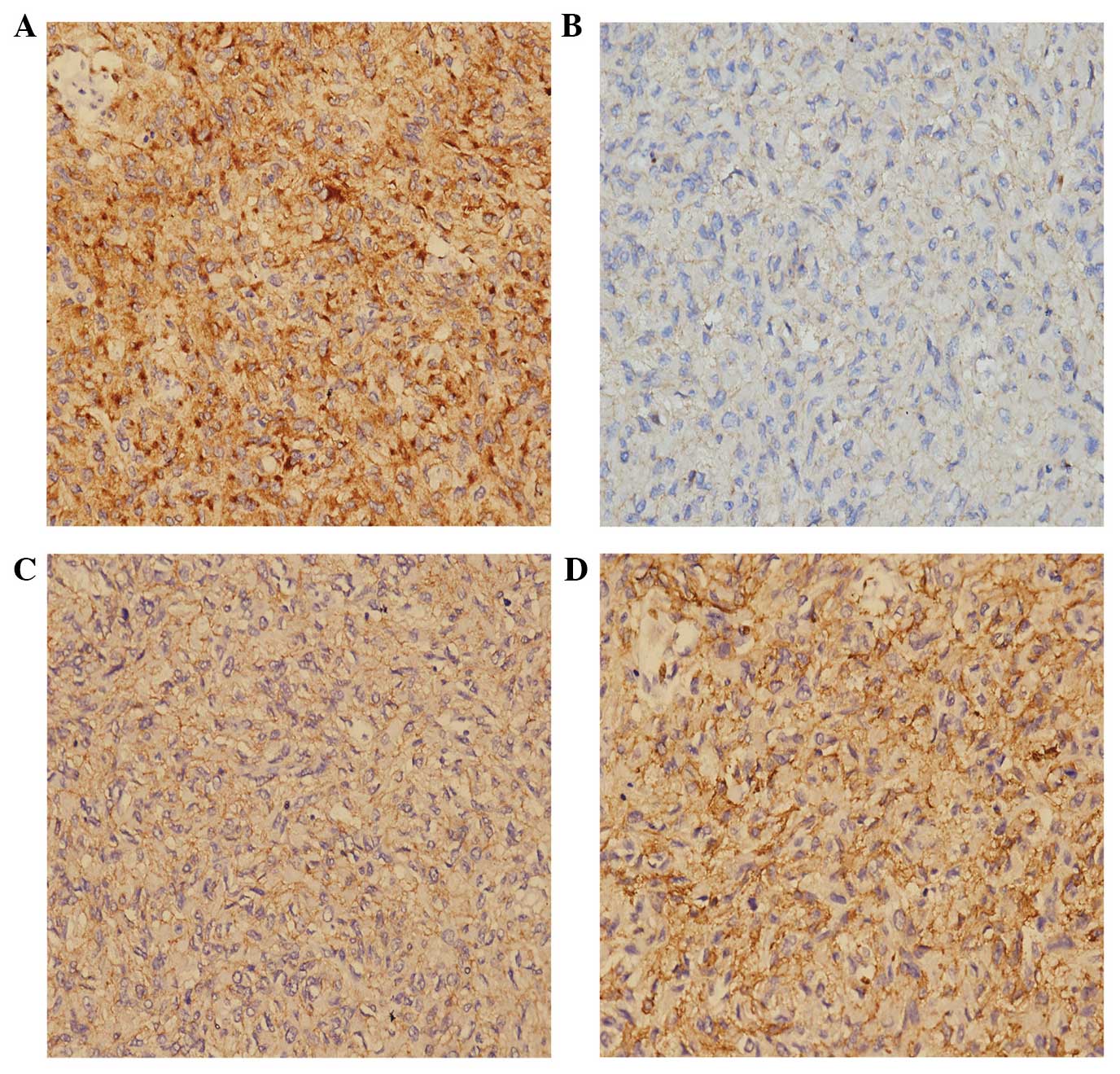
Immunohistochemical evaluation showed that the tumor cells were
positive for CD117, CD34, smooth muscle actin and Discovered on
GIST-1 (Fig. 3). The patient was
discharged on postoperative day 13. On June 20, 2011, a follow-up
examination was conducted using color Doppler ultrasonography and
enhanced CT imaging. Ultrasonography revealed 10 liver metastases
in right liver, with a tumor size ranging from 7–22 mm, and the
patient was readmitted for RFA treatment. All tumors were ablated
percutaneously under local or general anesthesia. Ultrasound or
contrast-enhanced ultrasound was used for tumor visualization. No
liver metastases were observed on postoperative CT imaging. On
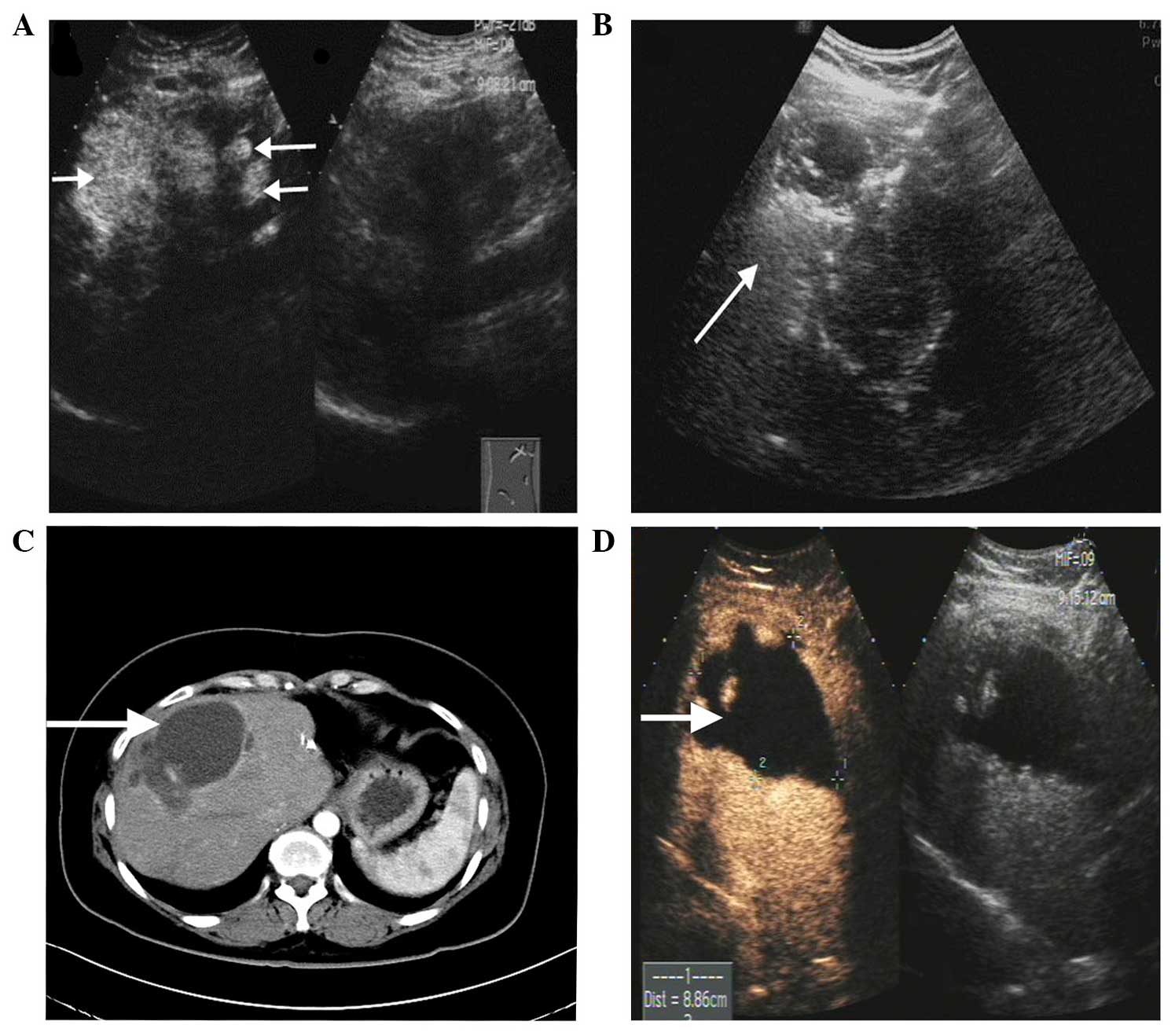
September 5, 2011, a follow-up examination revealed seven liver
metastases, the largest measuring 7.8 cm in diameter (Fig. 4A). The patient was readmitted for
further RFA, and postoperative ultrasonography revealed the lesion
to be hyperechoic (Fig. 4B). The
patient subsequently commenced therapy with oral imatinib (400
mg/day; Gleevec, Novartis, Switzerland); this regimen has been
continued to the present day.
During follow-up examinations in January and May
2012, color Doppler ultrasonography revealed five liver metastases,
and CT imaging revealed one liver metastasis. The patient
subsequently underwent further RFA. In total, two surgeries were
required to treat all tumors; three tumors were ablated for the
first time, and the remaining nodules were completely destroyed for
the second time. An abdominal CT scan (Fig. 4C) conducted on May 30, 2013, and
contrast-enhanced ultrasonography on February 25, 2014, (Fig. 4D) revealed that the metastatic liver
lesions had disappeared following RFA treatment and no new lesions
were observed. At present, the patient has undergone 36 months of
follow-up since the initial treatment with RFA, and has been
hospitalized five times for the further RFA treatment of a total of
27 metastases, which ranged in diameter from 7–78 mm. The patient
is currently stable and in good health. The most recent
contrast-enhanced ultrasonography of the liver and abdominal CT
imaging indicate no new or recurrent lesions.
Discussion
Liver metastasis is one major cause of mortality
among GIST patients. Following total resection of the original
tumor, liver metastases typically occur in 55% of patients
(6). The majority of GIST liver
metastases have complete capsules, with clear boundaries between
tumor and healthy liver tissues. Surgical resection is the primary
treatment for liver metastasis, and resection of the GIST itself
may be curative. Surgical resection has a 5-year survival rate of
34%, and a median survival time of 36 months (7). However, the rate of tumor recurrence
following liver resection may exceed 70% (7,8). As only a
small minority of patients are able to undergo repeated liver
resection, satisfactory outcomes are difficult to achieve with
surgical treatment alone.
RFA has been widely used for the treatment of liver
tumors; it has the advantage of easy administration that can be
repeated with minimal trauma and a low rate of complication
(9). However, few reports of RFA
treatment for GIST liver metastases have been published. Yamanaka
et al (10) reported the
successful treatment of a total of 21 liver metastases (maximum
diameter, 2.2±1.1 cm; range, 1.2–4.2 cm) from seven cases of GIST
using CT-guided RFA, with a GIST-related 5-year survival rate of
100%. Jones et al (11)
reported 13 cases of RFA treatment of GIST liver metastases, and a
post-RFA 2-year survival rate of 77%. This indicates that repeated
RFA may slow the rate of liver metastasis. In the present case, a
small number of asymptomatic pleural effusions in the right chest
were observed following two RFA sessions, and disappeared without
treatment, suggesting that RFA is an effective and safe way to
treat liver metastases from GIST.
Since 2000, the development and use of the tyrosine
kinase inhibitor, imatinib mesylate has greatly improved
molecular-targeted therapy for GIST. The c-kit expressed by the
majority of GISTs is the protein product of the c-kit
proto-oncogene; imatinib inhibits the enzymatic activity of c-kit,
suppresses cell proliferation and restores apoptosis. It has been
used successfully to treat unresectable and metastatic GIST, and
oral administration of imatinib produces satisfactory outcomes in
the majority of c-kit-positive patients (12,13). The
adverse effects of imatinib are mild and generally tolerable, and
include skin rash, edema, periorbital edema, diarrhea, nausea,
vomiting and bleeding sclera. Few patients experience complications
severe enough to merit the discontinuation of treatment. The
National Comprehensive Cancer Network recommends imatinib as a
first-line treatment for unresectable and metastatic GIST, and
patients with a medium to high risk of metastasis are advised to
receive at least 1 year of imatinib treatment following surgery
(14).
A number of studies indicate good efficacy of
combined RFA and imatinib therapy for GIST liver metastases. Pawlik
et al (15) reported 36 cases
of GIST liver metastases, in which the majority of patients who had
received RFA combined with imatinib therapy had a significantly
longer median survival compared with the patients who only received
RFA. A further case of combined RFA and imatinib treatment for
liver metastases was reported by Ishikawa et al (4); in this study, the patient experienced
>28 months of progression-free survival. The use of imatinib in
the absence of RFA has limited efficacy with regard to the
elimination of tumors and sustained tumor-free survival. Although
the tumor recurrence rate following RFA is high, it is valuable in
reducing the tumor load, delaying local tumor growth and
controlling development of the disease. This allows the opportunity
for patients to maintain tumor-free survival with oral imatinib
therapy.
In the present case, RFA combined with imatinib was
used to treat the largest number of liver metastases observed in a
single GIST patient to date. At 2 years following the most recent
RFA treatment, the patient continues to take imatinib orally,
exhibiting long-term tumor-free survival with satisfactory
therapeutic efficacy.
In conclusion, RFA combined with imatinib may be an
effective therapy in cases of multiple liver metastases arising
from GISTs. However, a large-sample study with appropriate
inclusion criteria is required to verify and further optimize this
treatment strategy. This study was approved by the Research Ethics
Committee of the Southwest Hospital, which is affiliated with The
Third Military Medical University. Written informed consent was
obtained from the patient.
Acknowledgements
The authors would like to thank the Southwest
Hospital Department of Information.
References
|
1
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: pathology and prognosis at different sites. Semin
Diagn Pathol. 23:70–83. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: review on morphology, molecular pathology,
prognosis, and differential diagnosis. Arch Pathol Lab Med.
130:1466–1478. 2006.PubMed/NCBI
|
|
3
|
Reith JD, Goldblum JR, Lyles RH and Weiss
SW: Extragastrointestinal (soft tissue) stromal tumors: an analysis
of 48 cases with emphasis on histologic predictors of outcome. Mod
Pathol. 13:577–585. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ishikawa A, Teratani T, Ono S, et al: A
case of gastrointestinal stromal tumor with liver and bone
metastases effectively treated with radiofrequency ablation and
imatinib mesylate. Nihon Shokakibyo Gakkai Zasshi. 103:1274–1279.
2006.(In Japanese). PubMed/NCBI
|
|
5
|
Minami T, Sato S, Watanabe Y, et al:
Successful treatment of a gastrointestinal stromal tumor with liver
metastases in a case that tolerated imatinib administration, by
radiofrequency ablation using contrast-enhanced ultrasonography.
Nihon Shokakibyo Gakkai Zasshi. 107:442–448. 2010.(In Japanese).
PubMed/NCBI
|
|
6
|
DeMatteo RP, Lewis JJ, Leung D, Mudan SS,
Woodruff JM and Brennan MF: Two hundred gastrointestinal stromal
tumors: recurrence patterns and prognostic factors for survival.
Ann Surg. 231:51–58. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nunobe S, Sano T, Shimada K, Sakamoto Y
and Kosuge T: Surgery including liver resection for metastatic
gastrointestinal stromal tumors or gastrointestinal
leiomyosarcomas. Jpn J Clin Oncol. 35:338–341. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gomez D, Al-Mukthar A, Menon KV, Toogood
GJ, Lodge JP and Prasad KR: Aggressive surgical resection for the
management of hepatic metastases from gastrointestinal stromal
tumours: a single centre experience. HPB (Oxford). 9:64–70. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li L, Zhang J, Liu X, Li X, Jiao B and
Kang T: Clinical outcomes of radiofrequency ablation and surgical
resection for small hepatocellular carcinoma: a meta-analysis. J
Gastroenterol Hepatol. 1:51–58. 2012. View Article : Google Scholar
|
|
10
|
Yamanaka T, Takaki H, Nakatsuka A, et al:
Radiofrequency ablation for liver metastasis from gastrointestinal
stromal tumor. J Vasc Interv Radiol. 24:341–346. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jones RL, McCall J, Adam A, et al:
Radiofrequency ablation is a feasible therapeutic option in the
multi modality management of sarcoma. Eur J Surg Oncol. 36:477–482.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gastrointestinal Stromal Tumor
Meta-Analysis Group (MetaGIST), . Comparison of two doses of
imatinib for the treatment of unresectable or metastatic
gastrointestinal stromal tumors: a meta-analysis of 1,640 patients.
J Clin Oncol. 28:1247–1253. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Blanke CD, Demetri GD, von Mehren M, et
al: Long-term results from a randomized phase II trial of standard-
versus higher-dose imatinib mesylate for patients with unresectable
or metastatic gastrointestinal stromal tumors expressing KIT. J
Clin Oncol. 26:620–625. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Demetri GD, von Mehren M, Antonescu CR, et
al: NCCN Task Force report: update on the management of patients
with gastrointestinal stromal tumors. J Natl Compr Canc Netw.
8:S1–S41. 2010.PubMed/NCBI
|
|
15
|
Pawlik TM, Vauthey JN, Abdalla EK, Pollock
RE, Ellis LM and Curley SA: Results of a single-center experience
with resection and ablation for sarcoma metastatic to the liver.
Arch Surg. 141:537–543. 2006. View Article : Google Scholar : PubMed/NCBI
|