Introduction
Neuroblastoma is an embryonal malignancy of the
sympathetic nervous system that is derived from primordial neural
crest cells. It is the most frequently occurring extracranial solid
tumor, accounting for 9–10% of all pediatric neoplasms, and heavily
contributes to childhood cancer mortality (1). The majority of cases are sporadic, and
may occur as a localized or disseminated disease. Spontaneous
regression may also be observed (2).
As the understanding of neuroblastoma tumors has
increased, it has become evident that these tumors behave
differently with regard to aggressiveness and response to
treatment. Multimodal therapies are necessary to improve the
prognosis of patients with progressive tumors, and aggressive
therapy must be avoided in patients with favorable tumor pathology
in order to reduce side effects and financial expenditure (3).
The Children's Oncology Group (COG) classifies
neuroblastoma patients into low, intermediate and high risk
categories based on certain characteristics including the age of
the patient, the stage of the disease upon initial diagnosis, the
histological appearance of the tumor, the quantitative DNA content
of the tumor (ploidy), and the presence or absence of amplification
of the MYCN oncogene (4).
The aim of the present study was to investigate the
clinico-epidemiological features of neuroblastoma in infants and
children in north east Egypt and to evaluate the association
between these clinico-epidemiological features and patient
outcome.
Materials and methods
The present retrospective study included 142
patients with neuroblastoma, who were diagnosed, treated and
followed-up at four main hospitals (Mansoura University Children's
Hospital and Mansoura Oncology Center, Mansoura; Zagazig University
Hospital, Zagazig; and Tanta University Hospital, Tanta, Egypt)
between January 2005 and January 2010. Of these cases, 10 were
omitted from the study due to defective data records. The remaining
132 cases were analyzed for demographic characteristics, and
factors impacting survival were determined. The clinical,
morphological and biological data obtained for each patient were
filed in a computerized database using SPSS software, version 14
(SPSS Inc., Chicago, IL, USA). A descriptive analysis was performed
for each variable, and the associations between variables, and
between each variable and outcome, were analyzed using the
appropriate statistical method (χ2, φ, Cramer's V,
Mann-Whitney, Kendall's τB and Median tests). The effect
sizes were estimated and used to evaluate the practical
significance of the results. Survival was measured from the date of
diagnosis to the date of death or of last follow-up. Overall
survivals (OAS) were estimated using Kaplan-Meier curves and
compared using a log-rank test and multivariate analysis using the
Cox regression method. P<0.05 was considered to indicate a
statistically significant difference.
The study was undertaken in accordance with ethical
standards and with the Helsinki Declaration of 1964 (as revised in
2000) and was approved by the ethical committees of Mansoura
University, Zagazig University and Tanta University. Written
informed consent was obtained from the patient's families.
Results
In total, 142 cases of neuroblastoma were identified
from the hospital records between January 2005 and January 2010,
and 10 cases were subsequently excluded due to defective data
records. Of the remaining 132 cases, 28 were diagnosed in 2005, 36
in 2006, 44 in 2007, 8 in 2008 and 16 in 2009. The cohort comprised
68 males and 64 females; 32 patients were aged <1 year, and 100
were aged ≥1 year. The median age at the time of diagnosis was 30
months (range, 2–96 months; Table
I).
 | Table I.Demographic characteristics of the
neuroblastoma patients included in the study. |
Table I.
Demographic characteristics of the
neuroblastoma patients included in the study.
| Demographic
characteristics | n | % |
|---|
| Year |
|
|
|
2005 | 28 | 21.2 |
|
2006 | 36 | 27.3 |
|
2007 | 44 | 33.3 |
|
2008 | 8 | 6.1 |
|
2009 | 16 | 12.1 |
| Age, years |
|
|
|
<1 | 32 | 24.2 |
| ≥1 | 100 | 75.8 |
| Gender |
|
|
|
Male | 68 | 51.5 |
|
Female | 64 | 48.5 |
Among the 32 patients aged <1 year, the primary
tumor site was suprarenal in 16 cases (50.0%), cervical in 4 cases
(12.5%), paraspinal in 4 cases (12.5%) and retroperitoneal in 8
cases (25.0%). Of the 96 cases of patients aged ≥1 year and with a
known primary tumor site, 80 (83.3%) were suprarenal, 4 (4.2%) were
paraspinal and 12 (12.5%) were retroperitoneal; a significantly
high proportion of patients aged ≥1 year had suprarenal tumor sites
(P=0.001, t=27.250, df=2, χ2 non-parametric test for
distribution within cases). No significant association was observed
between age at diagnosis and site of the primary tumor (P=0.161, φ
test) (Table II).
| Table II.Distribution of sites of the primary
tumor, INSS and pathology by age at presentation. |
Table II.
Distribution of sites of the primary
tumor, INSS and pathology by age at presentation.
|
| Age, years |
|
|
|
|---|
|
|
|
|
|
|
|---|
|
| <1 | ≥1 | Test | Statistic | P-value |
|---|
| Site of primary
tumor, n (%) |
|
| φ test | 0.401 | 0.161 |
| Supra
renal | 16 (50.0) | 80 (83.3) |
|
|
|
|
Neck | 4 (12.5) | 0
(0.0) |
|
|
|
|
Paraspinal | 4 (12.5) | 4
(4.2) |
|
|
|
|
Retroperitoneal | 8 (25.0) | 12 (12.5) |
|
|
|
| INSS, n (%) |
|
| Kendall's
τB | 0.359 | 0.026 |
|
IIB | 4 (16.7) | 4
(4.3) |
|
|
|
|
III | 8 (33.3) | 8
(8.7) |
|
|
|
| IV | 12 (50.0) | 80 (87.0) |
|
|
|
| Pathology (Shimada
classification), n (%) |
|
| Kendall's
τB | 0.618 | 0.008a |
|
Favorable | 20 (83.0) | 8
(20.0) |
|
|
|
|
Unfavorable | 4 (17.0) | 32 (80.0) |
|
|
|
As International Neuroblastoma Staging System (INSS)
stage IVS disease is defined by the age of the patient, cases of
this stage were excluded from the statistical assessment of the
association between age and tumor stage, in order to avoid bias.
The correlation between age in months and disease stage was
determined to be positive and significant [r=0.265, P=0.045
(one-tailed), Kendall's τB test]. In addition, a
significant association between age (ranked into <1 year and ≥1
year) and stage was identified [r=0.356; P=0.026 (one-tailed),
Kendall's τB test; Table
II].
A significant positive correlation was identified
between age in months and Shimada pathological status [r=0.364,
P=0.050 (one-tailed), Kendall's τB test]; with an age
cutoff of 1 year, a stronger correlation was identified, which was
significant at the 0.01 level [r=0.618, P=0.008 (one-tailed),
Kendall's τB test; Table
II].
Among the 28 patients with favorable pathology, 4
(14.3%) had stage II disease, 8 (28.6%) had stage III and 16
(57.1%) had stage IV. Of the 36 patients with unfavorable
pathology, 8 patients (22.2%) had stage III disease, 24 (66.7%) had
stage IV and 4 (11.1%) had stage IVS. Progression in stage was
associated with a higher proportion of unfavorable pathology cases,
which reached 60.0% in stage IV tumors (Table III).
| Table III.Relationship between Shimada
pathological status and stage according to INSS of the studied
neuroblastoma cases. Valid cases, n=64 (48.5%). |
Table III.
Relationship between Shimada
pathological status and stage according to INSS of the studied
neuroblastoma cases. Valid cases, n=64 (48.5%).
|
| INSS |
|
|
|
|---|
|
|
|
|
|
|
|---|
| Pathology (Shimada
classification), n (%) | IVS | IIB | III | IV | Total |
Statistica | P-value |
|---|
| Favorable | 0 (0.0) | 4 (14.3) | 8 (28.6) | 16 (57.1) | 28 (100) | 0.369 | 0.535 |
| Unfavorable | 4 (11.1) | 0 (0.0) | 8 (22.2) | 24 (66.7) | 36 (100) |
|
|
| Total | 4 (6.3) | 4 (6.3) | 16 (25.0) | 40 (62.5) | 64 (100) |
|
|
No significant association was found between
pathological status and stage (P=0.535). The correlation between
Shimada pathological status and stage according to INSS (by ranking
them into non-distant metastatic stages (I, II, III) and metastatic
stages (IV, IVS) was positive (r=0.221), but showed no statistical
significance (P=0.196; Tables III
and IV). Notably, a higher
percentage of patients in the unfavorable pathology group exhibited
evidence of central nervous system metastasis (85.7%) when compared
with the favorable pathology group (55.6%).
| Table IV.Association between Shimada
pathological status and metastasis in the studied neuroblastoma
cases. Valid cases, 64 (48.5%). |
Table IV.
Association between Shimada
pathological status and metastasis in the studied neuroblastoma
cases. Valid cases, 64 (48.5%).
|
| Metastasis |
|
|
|
|---|
|
|
|
|
|
|
|---|
| Pathology (Shimada
classification), n (%) | Non-metastatic
stages (I, II, III) | Metastatic stages
(IV, IVS) | Total |
Statistica | P-value |
|---|
| Favorable | 12 (42.9) | 16 (57.1) | 28 (100) | 0.221 | 0.196 |
| Unfavorable | 8
(22.2) | 28 (77.8) | 36 (100) |
|
|
| Total | 20 (31.3) | 44 (68.8) | 64 (100) |
|
|
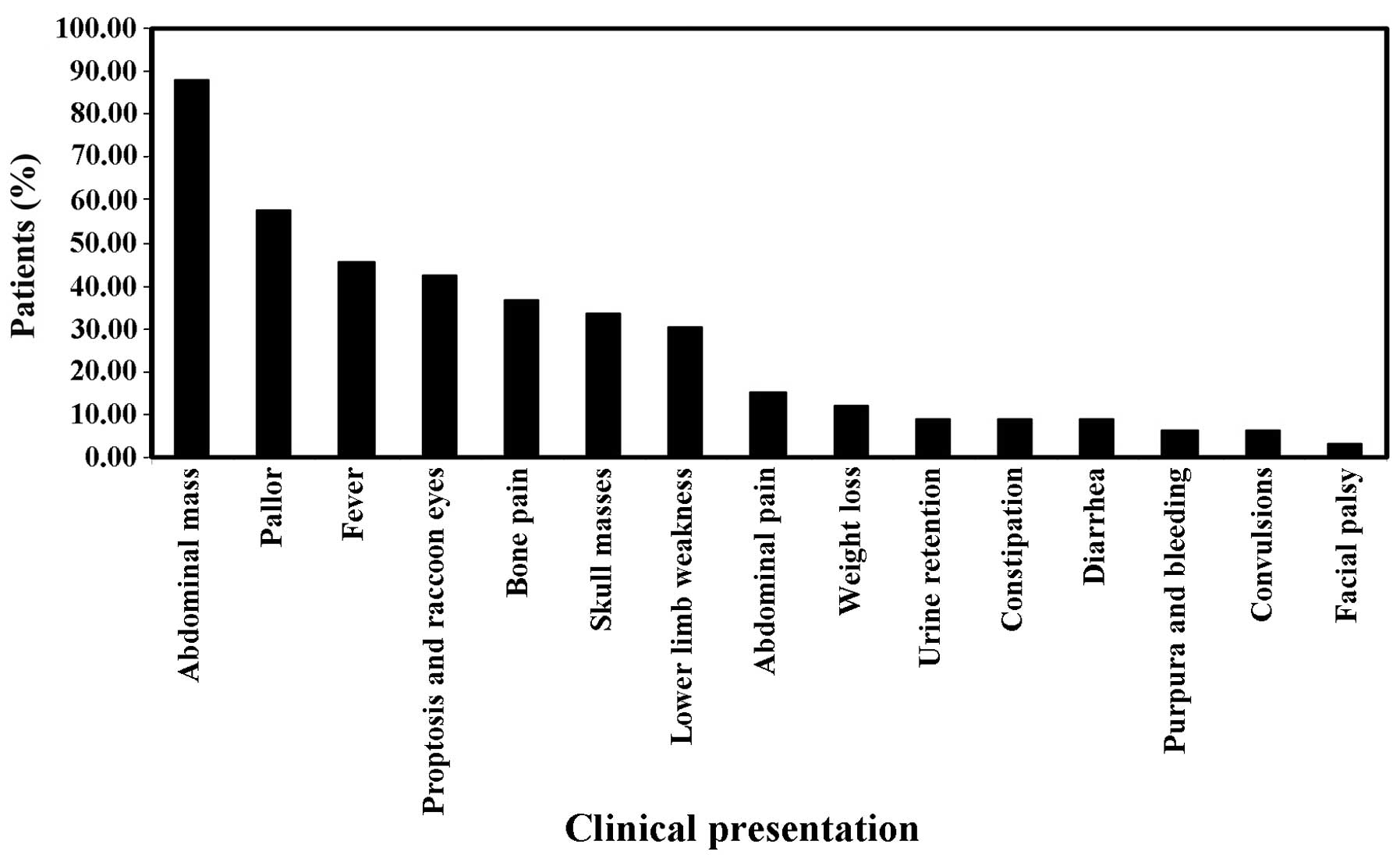
Clinical presentations were variable, with abdominal
mass being the most common (87.9%; 116 cases), followed by pallor
(57.6%; 76 cases), fever (45.5%; 60 cases), proptosis and/or
raccoon eye (42.4%; 56 cases), bone pain (36.4%; 48 cases), skull
masses (33.3%; 44 cases), lower limb weakness (30.3%; 40 cases),
abdominal pain (15.2%; 20 cases), weight loss (12.1%; 16 cases),
urine retention (9.1%; 12 cases), constipation (9.1%; 12 cases),
diarrhea (9.1%; 12 cases), purpura and/or bleeding (6.1%; 8 cases),
convulsions (6.1%; 8 cases) and facial palsy (3%; 4 cases)
(Fig. 1).
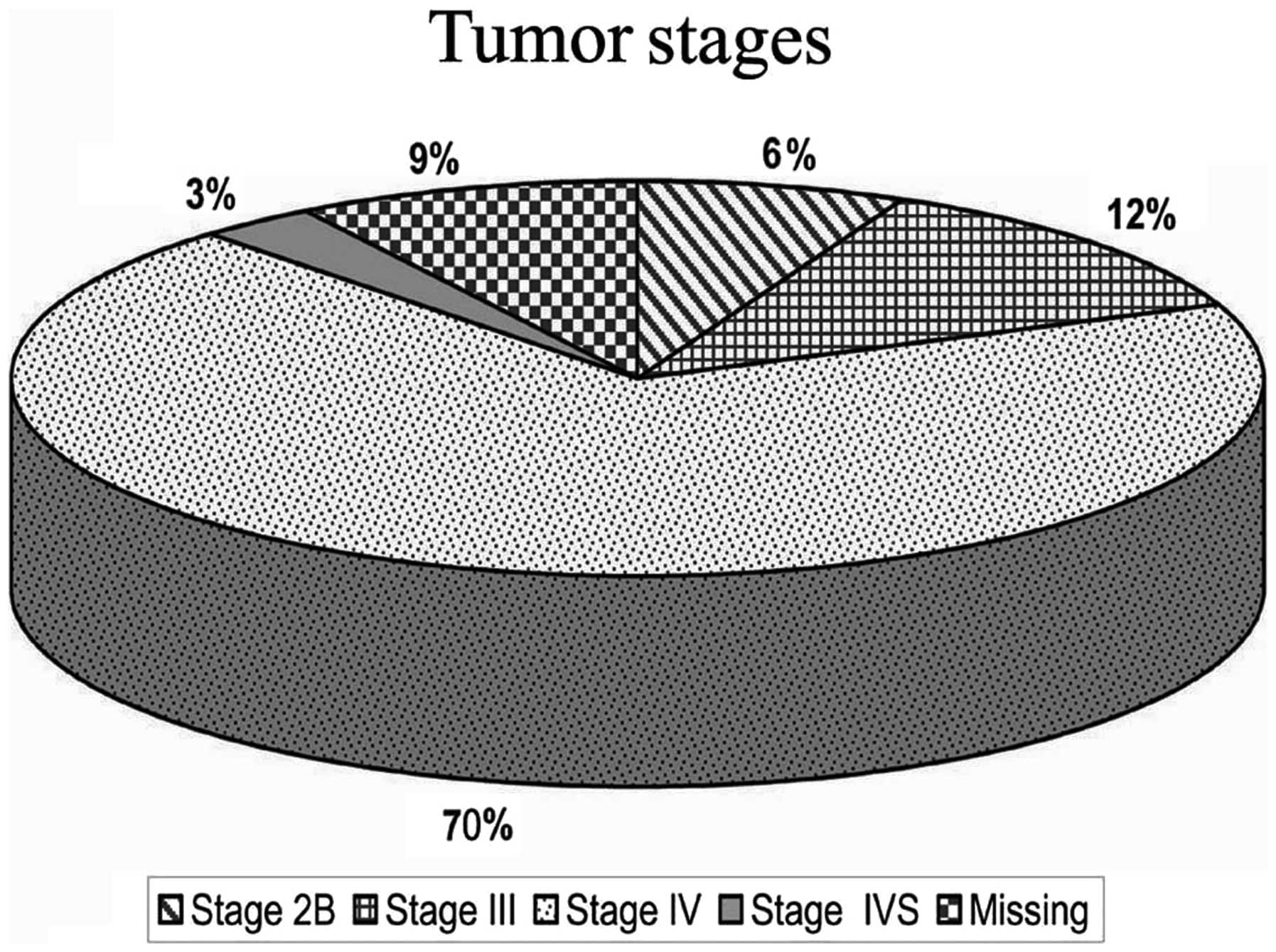
Of the 120 patients with known stage according to
INSS, 8 cases (6.1%) were stage IIB, 16 cases (12.1%) stage III, 92
cases (69.7%) stage IV and 4 cases (3%) were stage IVS (Fig. 2).
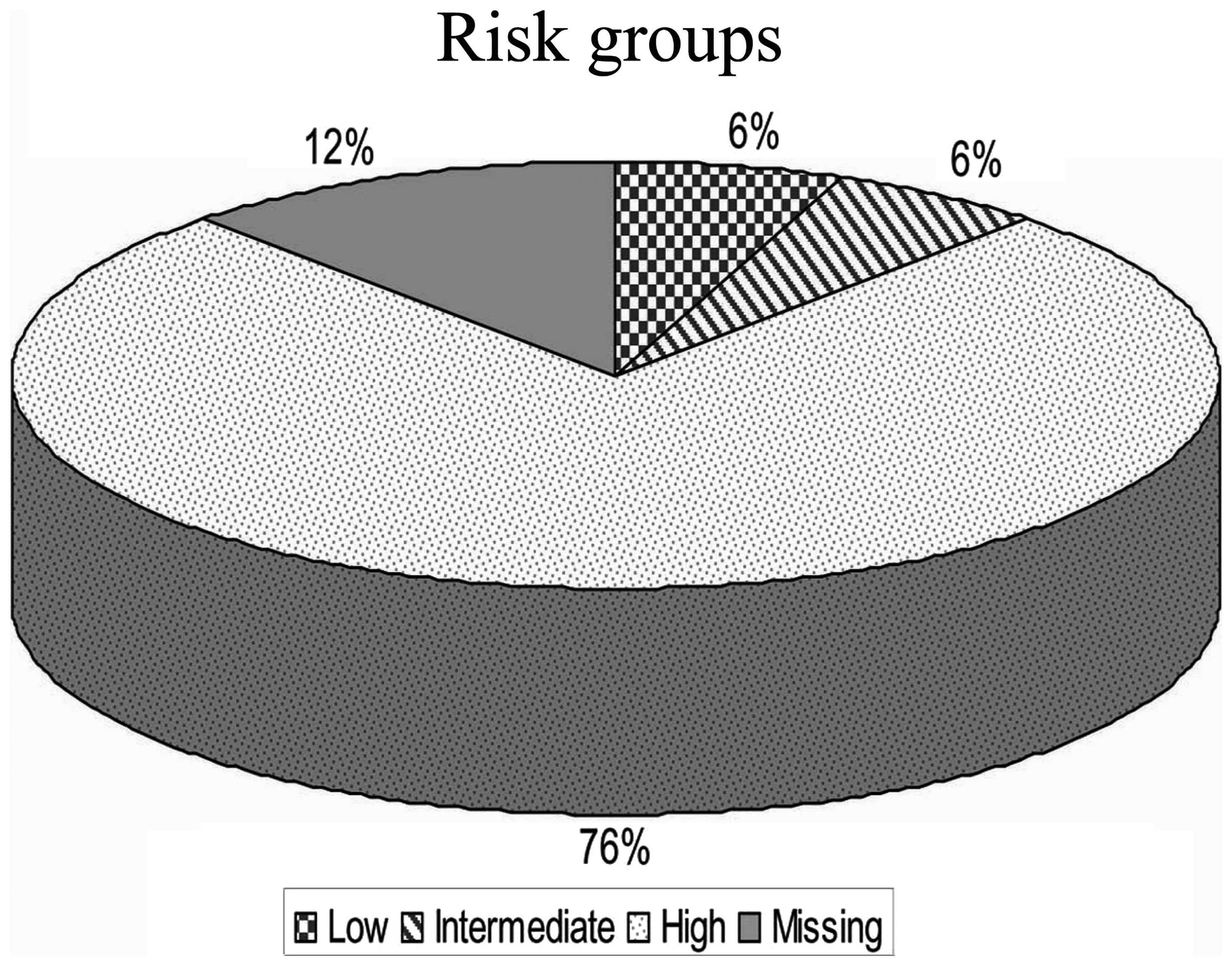
Among the 116 patients with known risk according to
COG risk group assignment for neuroblastoma, 8 cases (6.1%) were of
low risk, 8 cases (6.1%) were of intermediate risk and 100 cases
(75.8%) were of high risk. The high risk group included 4 patients
who were initially of low risk and were disease-free for a mean
period of 18 months, but subsequently suffered recurrence in the
form of bone secondary malignancies and bone marrow infiltration,
and were reclassified as high risk, receiving the COG high risk
treatment protocol (5) (Fig. 3).
The clinical, morphological and biological features
of patients with known outcome, their distribution and bivariate
analysis for outcome are listed in Table
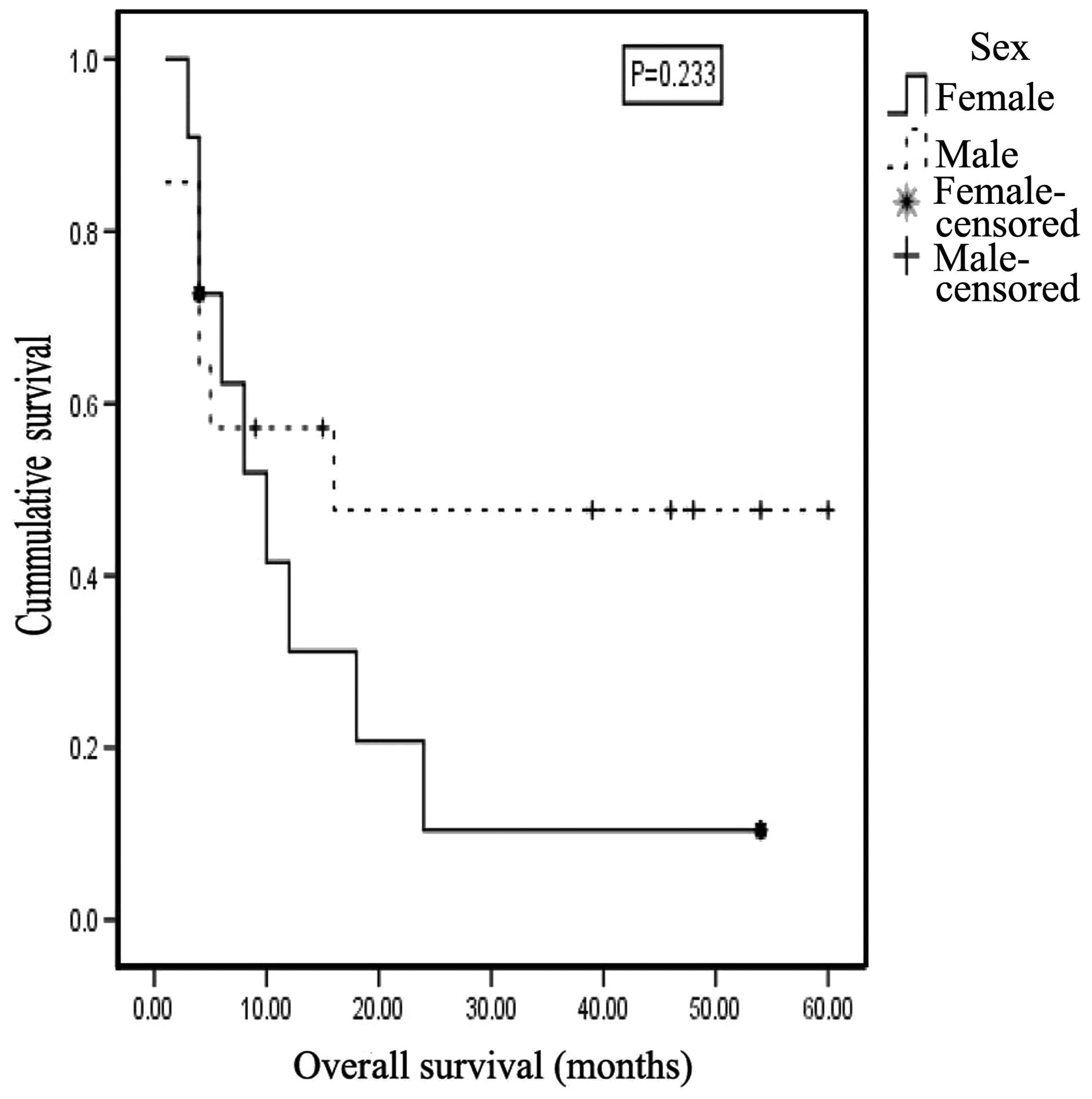
V. Of the 116 cases with known outcome, 64 were males, of which
28 (43.8%) were alive at the end of the current study and 36
(56.2%) succumbed to the disease. Of the 52 female patients, 8
(15.4%) are alive, and 44 (84.6%) succumbed to the disease. The
gender of the patients and the clinical outcome were not
significantly associated (P=0.101, φ test). However, a medium
effect size was estimated for these variables (r=0.305), and the
likelihood of mortality among females was 4.9 times higher compared
with that among males. The 2-year OAS for males was 47.6±14.0%
[mean ± standard deviation (SD)], compared with 10.4±9.8% for
females, with a mean survival time of 31.452±7.588 months for males
and 14.714±4.712 months for females. However, this difference was
not statistically significant (P=0.233) (Fig. 4).
| Table V.Distribution of outcome by clinical,
morphological and biological features. |
Table V.
Distribution of outcome by clinical,
morphological and biological features.
|
Characteristics | n | Valid, % | Alive | Deceased | Statistic | P-value | Test |
|---|
| Gender, n (%) |
|
|
|
|
| 0.101 | φ test |
|
Male | 64 | 51.5 | 28 (43.8) | 36 (56.2) |
|
|
|
|
Female | 52 | 48.5 | 8
(15.4) | 44 (84.6) |
|
|
|
| Age, n (%) |
|
|
|
| 0.493 | 0.005 | Kendall's
τB |
| <1
year | 28 | 24.2 | 20 (71.4) | 8
(28.6) |
|
|
|
| ≥1
year | 88 | 75.8 | 16 (18.2) | 72 (81.8) |
|
|
|
| Primary tumor site,
n (%) |
|
|
|
| 0.414 | 0.187 | Cramer's V |
|
Suprarenal | 84 | 75.0 | 20 (23.8) | 64 (76.2) |
|
|
|
|
Retroperitoneal | 24 | 21.4 | 16 (66.7) | 8
(33.3) |
|
|
|
|
Cervical | 4 |
3.6 | 0
(0.0) | 4
(100.0) |
|
|
|
| INSS, n (%) |
|
|
|
| 0.235 | 0.659 | Cramer's V |
| II | 8 |
6.9 | 4
(50.0) | 4
(50.0) |
|
|
|
|
III | 16 | 13.8 | 8
(50.0) | 8
(50.0) |
|
|
|
| IV | 88 | 75.9 | 24 (27.3) | 64 (72.7) |
|
|
|
|
IVS | 4 |
3.4 | 0
(0.0) | 4
(100.0) |
|
|
|
| Shimada, n (%) |
|
|
|
| 0.492 | 0.049 | φ test |
|
Favorable | 28 | 43.8 | 20 (71.4) | 8
(28.6) |
|
|
|
|
Unfavorable | 36 | 56.2 | 8
(22.2) | 28 (77.8) |
|
|
|
| COG risk, n
(%) |
|
|
|
| 0.448 | 0.067 | Cramer's V |
|
Low | 4 |
3.7 | 0
(0.0) | 4
(100.0) |
|
|
|
|
Intermediate | 8 |
7.4 | 8
(100.0) | 0
(0.0) |
|
|
|
|
High | 96 | 88.9 | 24 (25.0) | 72 (75.0) |
|
|
|
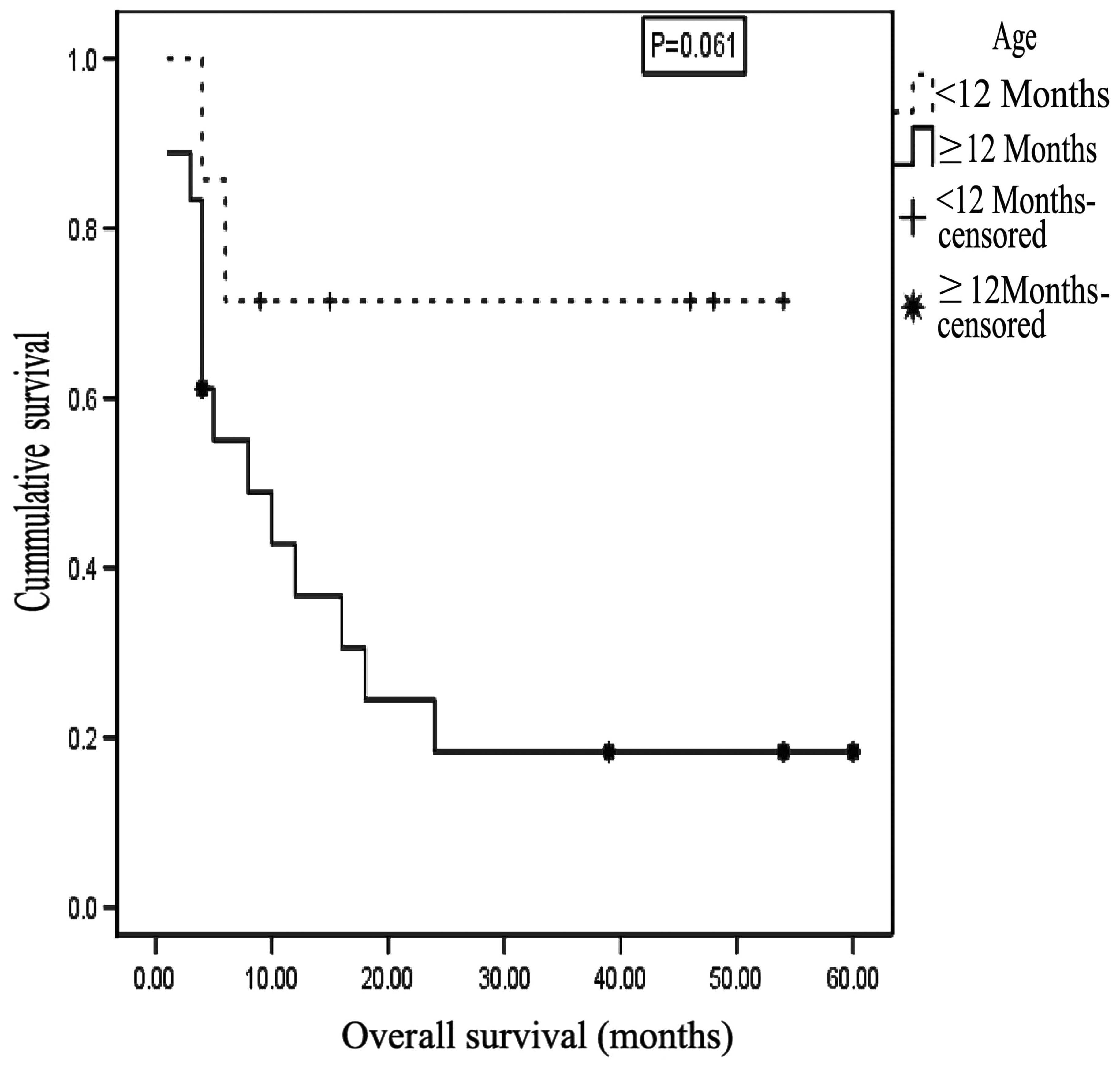
A significant negative correlation was identified
between age (in months) at presentation and outcome [r=-0.269, with
a medium effect size identified; P=0.047 (one-tailed), Kendall's
τB test]. Furthermore, the correlation was stronger and
significant at the P<0.01 level (one-tailed) when an age cutoff
of 12 months was applied (r=-0.493 with a large effect size;
P=0.005, Kendall's τB test). Among patients with known
outcome, 88 were aged ≥1 year, of which 18.2% survived and 81.8%
died (P=0.003, χ2 test for non-parametric distribution).
The median age at presentation was 10 months for survivors and 33
months for non-survivors. The odds of mortality among patients aged
≥1 year was 9 times higher compared with that of patients aged
<1 year. The 2-year OAS for patients <1 year of age upon
presentation was 71.4±17.1%, while for patients ≥1 year of age the
OAS was 18.3±9.5%, with a mean survival time of 40±8.4 months for
the former group and 17.6±5.1 months for the latter group. This
difference was not statistically significant (P=0.061, test
statistic=3.509, log rank test; Fig.
5).
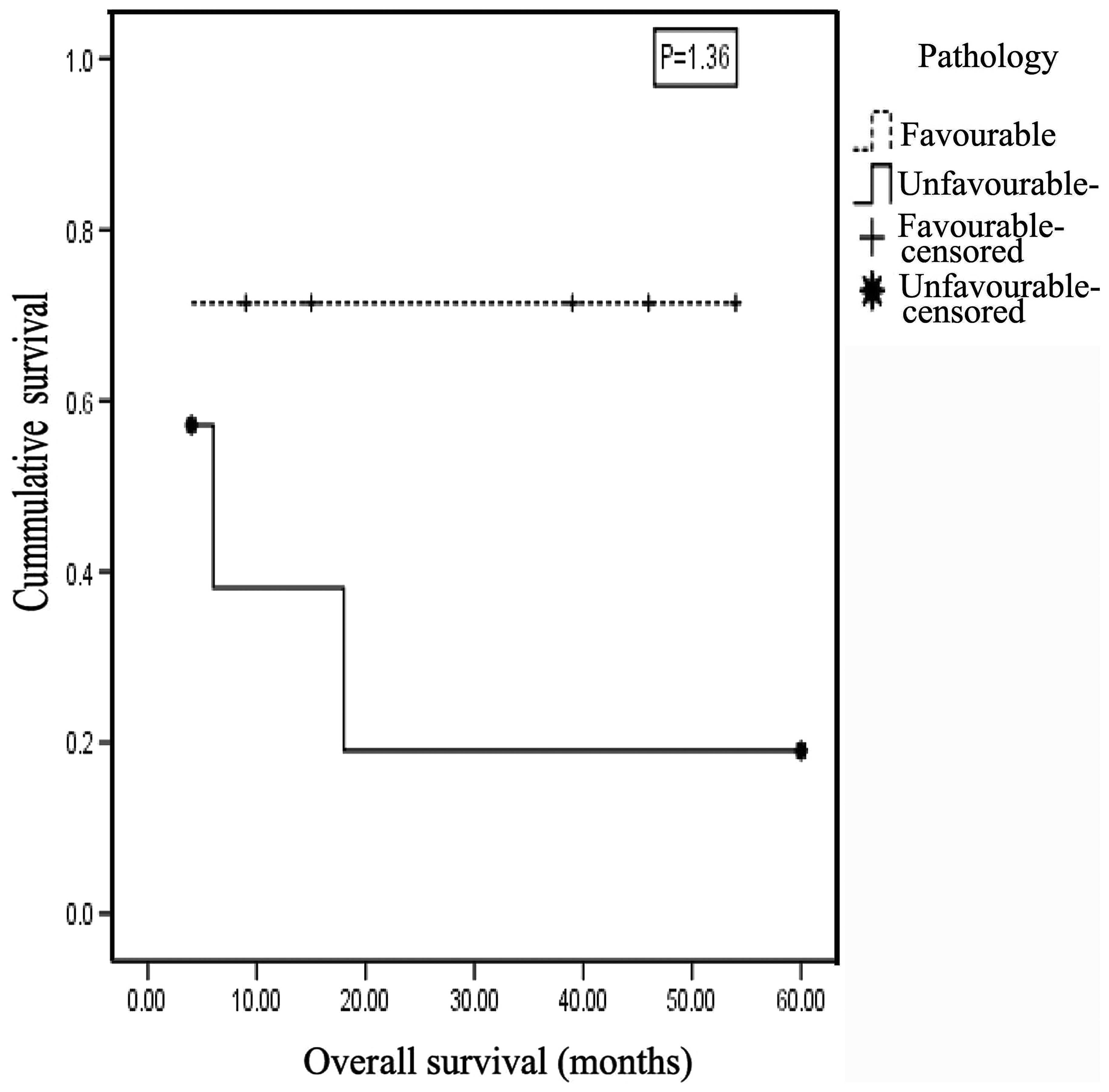
A significant association was identified between
Shimada pathological status and outcome (P=0.049, φ test) and the
effect size estimate indicated a large effect (r=0.492). The 2-year
OAS for the favorable pathology group was 71.4±17.1%, compared with
19.0±16.8% for the unfavorable pathology group, with a mean
survival time of 39.7±8.5 months for the former and 17.7±8.9 months
for the latter; this difference was not statistically significant
(P=1.36, test statistic=2.221, log rank test; Fig. 6). The odds of mortality among cases
with unfavorable pathology was 5.8 times higher compared with those
of favorable pathology.
The site of the primary tumor was not significantly
associated with outcome (P=0.187, Cramer's V test). However, a
large effect size was identified (r=0.414). The 2-year OAS for
patients with suprarenal mass did not differ significantly from
those with retroperitoneal mass (27.8±10.6% vs. 75.0±21.7%,
respectively; P=0.449, test statistic=2.648, log rank test).
In addition, no significant association was observed
between INSS stage and outcome (P=0.659, Cramer's V test; r=0.235,
small effect size) or between risk stratification and outcome
(P=0.067, Cramer's V test); however, a large effect size was
estimated for the latter (r=0.448).
Discussion
In the present study, the male-to-female ratio was
1.06, in concordance with the majority of reviewed studies in which
the ratio ranged from 1.1–1.5 (6,7). However,
in South Africa, a marginal female predominance has been identified
(8). SEER pediatric monograph
illustrated that the overall incidence among males was 6.5% higher
compared with that of females (9).
The majority of patients (75.8%) were aged ≥1 year
at the time of diagnosis, while 24.2% were aged <1 year; the
median age was 30 months. This is comparable with the results of a
study conducted in Denmark between 1943 and 1980, in which the
median age was 29 months (10). A
further Danish study, conducted between 1981 and 2000, observed the
median age at diagnosis to be 27 months, and 32% of the patients
were <1 year of age (11).
Additionally, a study of 20 Saudi patients with neuroblastoma
reported the median age at onset to be 36 months (12). In a Turkish study, the median age at
diagnosis was 43 months, with 21.8% of patients aged <1 year
(13), while a study in southern
Brazil reported that 25% of patients were ≤1 year of age, with
median age of 33 months at onset (7).
Children diagnosed at an age of <1.5 years accounted for 63.2%
of a Spanish study population (6).
The results of the present study were in discordance with the SEER
Pediatric Monograph, which revealed that incidence rate during the
second year of life was less than half that of infancy (9). Similarly, Wilson et al (14) reported that young infants, aged <1
year, have high incidence of neuroblastoma. This may be attributed
to spontaneous regression of neuroblastoma in the younger age group
(<1 year) and the lack of diagnosis in primary health care
centers, combined with the vagueness of the symptoms, which may
lead to a delay in diagnosis (14).
Suprarenal glands were the most common (72.7%)
primary tumor site, which was consistent with the findings of
previous studies. SEER monograph reported that, regardless of age,
neuroblastomas most frequently occurred in the adrenal gland
(9). Moon et al (15) also reported that the adrenal glands
were the most common primary site. In addition, the results from a
Norwegian cohort indicated that 46.6% of neuroblastoma masses were
identified in the adrenal glands (16). A study of neuroblastoma patients over
a period of 10 years in a Saudi hospital reported that the primary
sites of involvement included the following: Adrenal, 55%;
retroperitoneal, 15%; thoracic, 10%, cervical, 5%; pharyngeal, 5%;
lumbar, 5%; unknown, 5% (12). In a
study conducted in southern Africa, the most common primary tumor
sites included the abdomen (75%), thorax (15%), pelvis (5%), with
5% located in other sites (8). In
addition, a study conducted in southern Brazil over 11 years
identified adrenal tumors in 49% of patients (7).
In the present study, the majority of patients
(76.7%) had stage IV disease, which is comparable with the results
of a Mexican study, in which 88.0% of patients were classified as
stage III, IV, or IVS (17). The
findings are also similar to those of Mora et al (2) who found that the majority of
neuroblastoma patients presented with advanced, and often
unresectable, metastatic disease. Additionally, in southern Brazil,
one study reported that 64% of patients were classified as stage IV
(7).
The high percentage of stage IV in the present study
may be attributed to a lack of awareness by general practitioners
of the probability of cancer, particularly in infancy when
localized stages are more common, and to the lack of ultrasound
usage, such that tumors are not initially identified, and
subsequently regress or are later diagnosed at a more advanced
stage in a tertiary hospital. This explanation may also account for
the similar findings in Mexico and Brazil (7,17), and is
consistent with the postulation by Spix et al (18), in a study of neuroblastoma in Europe
between 1978 and 1992, that the variation in stage distribution
between countries may be explained by differences in the frequency
of diagnosis of localized cases.
Thus, greater consideration of neuroblastoma as a
potential diagnosis in primary care centers, and more frequent use
of ultrasound, may lead to a higher observed incidence of the
disease (due to detection of cases that would otherwise have
spontaneously regressed) and a greater proportion of cases of
younger patients and of localized disease.
In the present study, 43.8% of patients exhibited
favorable pathology and 56.2% had unfavorable pathology. These
findings were similar to those of a study of Spanish patients in
which 39.5% of neuroblastomas were considered to be of favorable
pathology, and 60.5% of unfavorable pathology (6).
Of the patients in the current study, 60.6%
succumbed to the disease. The estimated survival rate was
30.7±10.0%, and the mean survival time was 24.2±5.2 months. By
contrast, a study of Spanish patients reported a mortality rate of
25.8%, with a three-year estimated survival rate of 72.9% and a
mean survival time of 73 months (6).
However, 63.2% of these patients were <1.5 years of age and
29.7% were classified as stage IV, compared with the 24.2% aged
<1 year and 76.7% stage IV in the current cohort. These
variations, in addition to differences in medical care level and
economic issues, may have contributed to the discrepancies between
the findings of the two studies.
In a Mexican study, an overall 5-year survival rate
of 64% was reported (17) whilst in
Denmark, the 5-year survival rate showed an increase from 38% in
1981–1985, to 59% in 1996–2000 (11).
In a cohort study of neuroblastoma in Europe between 1978 and 1992,
the 5-year overall survival was 48% (18). In the present study, the probability
of survival was greater for patients of a younger age at onset,
with a significantly better outcome for patients <1 year of age
at presentation; this was consistent with findings from previous
studies (7,19,20). SEER
monograph revealed that infants aged <1 year with neuroblastoma
had a more favorable prognosis compared with children >1 year of
age (9). These findings are
consistent across a number of studies, which have reported that an
age cut-off of 365 days is clinically significant for risk
stratification (21,22). This age cut-off was based on
observations by Breslow and McCann over 40 years ago (23).
However, there is conflicting evidence regarding the
age cut-off. A number of studies have proposed a higher cut-off of
460 days (24) or 18 months (13). In a Spanish study, patients <18
months of age demonstrated better outcomes and a prolonged survival
(87 months) compared with those aged >18 months. Of the patients
who survived, the mean age at diagnosis was 17 months; this was
almost half the age of the patients who did not survive (31.3
months) (6).
The association between age and survival is also
supported by the results of a large European study, which found
that survival was highest in Germany, and that UK mortality rates
were significantly higher compared with that of Germany or France.
This was due to the higher incidence of the disease below 12 months
of age in Germany; in the UK, a deficit of low-stage disease in
infants was accompanied by an excess of stage IV disease in older
children. Significantly fewer incidental diagnoses were reported in
the UK (8%) compared with Austria (27%) and Germany (34%). In
Finland, which has the highest survival in the Nordic countries,
>50% of children with newly diagnosed neuroblastoma were aged
<12 months, compared with only 33% of Danish children (25).
Furthermore, age at presentation affects the impact
of other prognostic factors on survival due to the genomic
amplification of MYCN, which has a profound adverse
influence on tumor behavior in infant neuroblastoma patients with
metastatic disease. Schmidt et al (26) reported that 3-year event-free survival
(EFS) rates were 93±4% versus 10±7% based on the absence or
presence, respectively, of MYCN amplification in patients
<1 year of age. By contrast, the adverse prognostic effect of
MYCN amplification is diluted in stage IV patients >1
year of age at diagnosis.
In the present study, a strong association was
observed between the primary tumor site and survival, with 84.2% of
mortalities associated with a suprarenal mass. These results were
consistent with that of the European Neuroblastoma Study Group in
its study of neuroblastoma in Europe (1982–1992), which revealed
that the site of the primary malignancy significantly affected
prognosis (27). In two Danish
studies, the prognosis was observed to be most favorable in cases
involving cervical or thoracic tumors, progressively worsening for
thoraco-abdominal and abdominal tumors (other than adrenal), and
poorest for adrenal tumors (10,11).
Furthermore, the International Neuroblastoma Risk Group Task Force
reported that an adrenal primary tumor site was associated with
significantly worse EFS compared with all other primary sites
combined (28). The effect of the
primary malignancy site on survival may be due to the fact that the
tumors localized to the neck or thorax result in early symptoms, in
contrast to the ‘silent’ abdominal tumors, which are typically not
diagnosed until symptoms from dissemination occur (14).
In the present study, the risk of death from
neuroblastoma among females was observed to be 4.9 times higher
than that of males, with females accounting for only 22.2% of
survivors. The age at presentation did not differ between males and
females, however, 12/14 females (85.7%) had stage IV disease, in
comparison to 11/16 males (68.8%). Additionally, 5/7 female
patients (71.4%) exhibited unfavorable pathology, compared with 4/9
male patients (44.4%).
In a Spanish study (6), 56.3% of survivors were males. Although
this was similar with regard to the improved outcome for male
patients, the percentages differ markedly from that of the present
study, in which only 22.2% of the survivors were females.
Furthermore, in contrast to the current investigation, a number of
studies have reported no differences in survival between genders
(10,18,27), and a
Turkish study found that male gender was a significant determinant
of poor prognosis (13).
The pathological status of patients according to the
International Neuroblastoma Pathology Classification (INPC) was
significantly and strongly correlated with outcome: 77.8% of
patients with unfavorable pathology succumbed to the disease, with
a mean survival time of 17.7±8.9 months, whilst 71.4 % of those
with favorable pathology survived with a mean survival time of
39.7±8.5 months. A study by Burgues et al (6) reported that pathology was associated
with outcome; the majority of patients (93.8%) in the favorable
pathology group survived, and the mean survival time for this group
(89 months) was significantly higher compared with that of the
unfavorable group (57 months). The prognostic value of the INPC
system has been confirmed in a number of reports (29).
The findings of the present study revealed that the
number of mortalities was significantly increased for the higher
disease stages, with a mean survival time of 21.9±5.6 months for
those with stage IV disease. Similarly, the European Neuroblastoma
Study Group reported that disease stage is a highly significant
prognostic factor (27). Furthermore,
a Spanish study demonstrated that stage IV disease was associated
with poor prognosis: In these patients, the a mean survival time
was 35 months, and the rate of mortality was 59.3% (6). Two subsequent studies in Denmark found
that clinical stage was a highly significant prognostic factor,
with survival rate progressively worsening from stage I to stage
IV, and the survival of stage IV-S patients intermediate to these
two stages (10,11). In an Iranian study of 43 neuroblastoma
patients over 8 years, disease stage was found to be the most
important factor predicting outcome (19).
In the current study, biochemical and genetic data
were relatively sparse, providing little insight with regard to
their impact on long-term outcomes. MYCN status was known
for only 24 patients as these were the only cases for which
MYCN status had been requested. This was attributed to the
fact that, from 2005–2006, the chemotherapy protocol used for
neuroblastoma was the same for all patients [PE-CADO protocol
(30)] since data regarding different
risk factors was limited and risk-based treatments had not yet been
established, and MYCN status did not affect the treatment
strategy. Even after application of the risk stratification system
in treatment, the hospital assessed MYCN status only in
patients for whom this would determine risk classification.
Accordingly, 5 out of 6 patients for whom MYCN status was
assessed had favorable pathology. These restrictions on the
determination of MYCN status are attributed to the cost of
such assessment and to limited resources. This was also observed in
a Turkish study (9), and in a study
in southern Africa (8), which
proposed that serum LDH, serum ferritin and histology may be
utilized as simple and inexpensive tests, with good predictive
values for outcome, in countries with limited resources with which
to stratify patients due to the unavailability of molecular tests.
This is used in many developing countries where detailed molecular
or biological tests remain unavailable. Tailored therapy is
primarily based on clinical factors including age, disease stage
and pathology. Consistently, the results of the present study
revealed that clinical data were valuable and useful in the risk
stratification of patients when other biological and molecular
determinants were not available. However, previous studies support
the association between adverse outcomes and MYCN
amplification (31).
The results of the present study revealed that
risk-based chemotherapy protocols did not improve cure rates or
survival compared with the previously used PE-CADO protocol. The
limited supportive care and financial resources in Egypt, as in
other developing countries, hinders the application of aggressive
chemotherapy followed by bone marrow transplantation (8).
In the current study, suprarenal primary tumor sites
were significantly associated with an age of ≥1 year at
presentation. This is consistent with a Turkish study, in which
thoracic and neck tumors were more prevalent in patients aged
<18 months, and abdominal disease was more prevalent in patients
aged >18 months (13). This may be
due to the in utero initiation of neuroblastoma, meaning
that tumors originating in hidden sites, including suprarenal
sites, take a greater period of time to present, and are therefore
associated with the older age group, in contrast to tumors
originating in sites such as the neck and paraspinal regions, where
they are detectable at an earlier stage.
The present study revealed a statistically
significant association between age at presentation and INSS stage,
with older age associated with higher stages, and a significant
cut-off age of 12 months. This finding is concordant with previous
studies in which biological evidence of a correlation between age
and stage was identified (13,32).
However, a Mexican study found no association between disease stage
and age at the time of diagnosis (17).
Only 42.9% of patients who presented at <1 year
of age had localized disease (stages I, II, III). This may be
attributed to the lack of diagnosis of localized stages in infants,
leading to the appearance of an aberrantly high percentage of
metastatic stages in this age group. This hypothesis is supported
by the results of a German study in which infants were screened,
and 87% of the cases of the disease were found to be localized
(stages I, II or III) (33). The
present study revealed that progression in stage implied a higher
proportion of cases with unfavorable pathology, reaching 60.0% in
INSS stage IV tumors. This was consistent with the results of a
Spanish study (6), which reported
that tumor stage was significantly associated with INPC prognosis,
with unfavorable cases reaching 89.3% in INSS stage IV tumors.
However, in a Mexican study (17), no
correlation between Shimada classification (favorable or
unfavorable histology) and stage was identified.
In the present study, the higher percentage of
patients with evidence of central nervous system metastasis in the
unfavorable pathology group (85.7%), compared with the favorable
pathology group (55.6%), may account for the association between
pathology and stage.
The present study identified age to be significantly
associated with pathology in continuous manner, however, this was
more clinically and statistically significant when an age cutoff of
12 months was used to group patients. This was consistent with the
findings of London et al (32)
and of Shimada (34), who observed
biological evidence of a correlation between age and
histopathology. The association between age at presentation,
disease stage and pathology supports the hypothesis that
neuroblastoma consists of more than two distinct subtypes (35).
In conclusion, the association between age at
presentation, stage and pathology supports the hypothesis that
neuroblastoma is a heterogeneous disease. The establishment of an
effective, computerized, research-oriented registration system for
neuroblastoma is urgently required in north east Egypt.
Furthermore, larger international multicenter studies are required
to support the findings of the present study.
References
|
1
|
Schwab M, Westermann F, Hero B and
Berthold F: Neuroblastoma: Biology and molecular and chromosomal
pathology. Lancet Oncol. 4:472–480. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mora J, Gerald WL, Qin J and Cheung NK:
Evolving significance of prognostic markers associated with
treatment improvement in patients with stage 4 neuroblastoma.
Cancer. 94:2756–2765. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
De Bernardi B, Mosseri V, Rubie H, et al
SIOP Europe Neuroblastoma Group: Treatment of localised resectable
neuroblastoma. Results of the LNESG1 study by the SIOP Europe
Neuroblastoma Group. Br J Cancer. 99:1027–1033. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Look AT, Hayes FA, Nitschke R, et al:
Cellular DNA content as a predictor of response to chemotherapy in
infants with unresectable neuroblastoma. N Engl J Med. 311:231–235.
1984. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Matthay KK, Reynolds CP, Seeger RC, et al:
Long-term results for children with high-risk neuroblastoma treated
on a randomized trial of myeloablative therapy followed by
13-cis-retinoic acid: A children's oncology group study. J Clin
Oncol. 27:1007–1013. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Burgues O, Navarro S, Noguera R, Pellín A,
Ruiz A, Castel V and Llombart-Bosch A: Prognostic value of the
International Neuroblastoma Pathology Classification in
Neuroblastoma (Schwannian stroma-poor) and comparison with other
prognostic factors: A study of 182 cases from the Spanish
Neuroblastoma Registry. Virchows Arch. 449:410–420. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Parise IZ, Haddad BR, Cavalli LR, et al:
Neuroblastoma in southern Brazil: An 11-year study. J Pediatr
Hematol Oncol. 28:82–87. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hesseling PB, Ankone K, Wessels G,
Schneider JW, Du Plessis L and Moore S: Neuroblastoma in southern
Africa: Epidemiological features, prognostic factors and outcome.
Ann Trop Paediatr. 19:357–363. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Goodman MT, Gurney JG, Smith MA, et al:
Sympathetic nervous system tumors. In: Cancer incidence and
survival among children and adolescents: United States SEER Program
1975–1995National Cancer Institute. SEER Program. NIH Pub.
No.99-4649. Ries LAG, Smith MA, Gurney JG, et al: Bethesda, MD:
1999
|
|
10
|
Carlsen NLT, Christensen IJ, Schroeder H,
Bro PV, Erichsen G, Hamborg-Pedersen B, Jensen KB and Nielsen OH:
Prognostic factors in neuroblastomas treated in Denmark from 1943
to 1980. A statistical estimate of prognosis based on 253 cases.
Cancer. 58:2726–2735. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schroeder H, Wacher J, Larsson H, Rosthoej
S, Rechnitzer C, Petersen BL and Carlsen NL: Unchanged incidence
and increased survival in children with neuroblastoma in Denmark
1981–2000: A population-based study. Br J Cancer. 100:853–857.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
al-Mulhim I: Neuroblastoma in children: A
10-year experience in Saudi Arabia. J Trop Pediatr. 44:77–80. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Aydn GB, Kutluk MT, Yalçn B, Büyükpamukçu
M, Kale G, Varan A, Akyüz C, Senocak ME and Büyükpamukçu N:
Neuroblastoma in Turkish children: Experience of a single center. J
Pediatr Hematol Oncol. 31:471–480. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wilson LM and Draper GJ: Neuroblastoma,
its natural history and prognosis: A study of 487 cases. BMJ.
3:301–307. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moon SB, Park KW, Jung SE and Youn WJ:
Neuroblastoma: Treatment outcome after incomplete resection of
primary tumors. Pediatr Surg Int. 25:789–793. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Méhes G, Luegmayr A, Kornmüller R, Ambros
IM, Ladenstein R, Gadner H and Ambros PF: Detection of disseminated
tumor cells in neuroblastoma: 3 log improvement in sensitivity by
automatic immunofluorescence plus FISH (AIPF) analysis compared
with classical bone marrow cytology. Am J Pathol. 163:393–399.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Juárez-Ocaña S, Palma-Padilla V,
González-Miranda G, Siordia-Reyes AG, López-Aguilar E,
Aguilar-Martínez M, Mejía-Aranguré JM, Carreón-Cruz R,
Rendón-Macías ME and Fajardo-Gutiérrez A: Epidemiological and some
clinical characteristics of neuroblastoma in Mexican children
(1996–2005). BMC Cancer. 9:2662009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Spix C, Aareleid T, Stiller C, Magnani C,
Kaatsch P and Michaelis J: Survival of children with neuroblastoma.
time trends and regional differences in Europe, 1978–1992. Eur J
Cancer. 37:722–729. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Arzanian MT and Esfahani H: Neuroblastoma;
variable symptoms of a neurogenic tumor; a report from Iran. IJCN.
3:33–39. 2008.
|
|
20
|
Grosfeld JL: Risk-based management of
solid tumors in children. Am J Surg. 180:322–327. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Joshi VV, Cantor AB, Altshuler G, et al:
Age-linked prognostic categorization based on a new histologic
grading system of neuroblastomas. A clinicopathologic study of 211
cases from the Pediatric Oncology Group. Cancer. 69:2197–2211.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Berthold F, Kassenböhmer R and Zieschang
J: Multivariate evaluation of prognostic factors in localized
neuroblastoma. Am J Pediatr Hematol Oncol. 16:107–115.
1994.PubMed/NCBI
|
|
23
|
Breslow N and McCann B: Statistical
estimation of prognosis for children with neuroblastoma. Cancer
Res. 31:2098–2103. 1971.PubMed/NCBI
|
|
24
|
Saito T, Tsunematsu Y, Saeki M, Honna T,
Masaki E, Kojima Y and Miyauchi J: Trends of survival in
neuroblastoma and independent risk factors for survival at a single
institution. Med Pediatr Oncol. 29:197–205. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Powell JE, Estève J, Mann JR, Parker L,
Frappaz D, Michaelis J, Kerbl R, Mutz ID and Stiller CA:
Neuroblastoma in Europe: Differences in the pattern of disease in
the UK. SENSE. Study group for the Evaluation of Neuroblastoma
Screening in Europe. Lancet. 352:682–687. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Schmidt ML, Lukens JN, Seeger RC, et al:
Biologic factors determine prognosis in infants with stage IV c. J
Clin Oncol. 18:1260–1268. 2000.PubMed/NCBI
|
|
27
|
Cotterill SJ, Pearson AD, Pritchard J,
Foot AB, Roald B, Kohler JA and Imeson J: Clinical prognostic
factors in 1277 patients with neuroblastoma: Results of The
European Neuroblastoma Study Group ‘Survey’ 1982–1992. Eur J
Cancer. 36:901–908. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cohn SL, Pearson AD, London WB, et al INRG
Task Force: The International Neuroblastoma Risk Group (INRG)
classification system: An INRG Task Force report. J Clin Oncol.
27:289–297. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Matthay KK, Perez C, Seeger RC, et al:
Successful treatment of stage III neuroblastoma based on
prospective biologic staging: A Children's Cancer Group study. J
Clin Oncol. 16:1256–1264. 1998.PubMed/NCBI
|
|
30
|
Bernard JL, Philip T, Zucker JM, et al:
Sequential cisplatin/VM26 and
vincristine/cyclophosphamide/doxorubicin in metastatic
neuroblastoma: An effective alternating non-cross-resistant
regimen? J Clin Oncol. 5:1952–1959. 1987.PubMed/NCBI
|
|
31
|
Bagatell R, Rumcheva P, London WB, et al:
Outcomes of children with intermediate-risk neuroblastoma after
treatment stratified by MYCN status and tumor cell ploidy. J Clin
Oncol. 23:8819–8827. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
London WB, Castleberry RP, Matthay KK, et
al: Evidence for an age cutoff greater than 365 days for
neuroblastoma risk group stratification in the Children's Oncology
Group. J Clin Oncol. 23:6459–6465. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Schilling FH, Spix C, Berthold F, et al:
Neuroblastoma screening at one year of age. N Engl J Med.
346:1047–1053. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Shimada H, Umehara S, Monobe Y, et al:
International neuroblastoma pathology classification for prognostic
evaluation of patients with peripheral neuroblastic tumors: A
report from the Children's Cancer Group. Cancer. 92:2451–2461.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Pritchard J and Hickman JA: Why does stage
4s neuroblastoma regress spontaneously. Lancet. 344:869–870. 1994.
View Article : Google Scholar : PubMed/NCBI
|