Introduction
Osteosarcoma is derived from mesenchymal tissues and
often occurs in the distal femur, proximal tibia and humeral
metaphysis. Osteosarcoma is one of the most common malignant tumors
in children and adolescents. It is estimated that the annual
incidence of osteosarcoma is 4–5 cases per 1,000,000 individuals
worldwide, and osteosarcoma is a leading cause of cancer-associated
mortalities in children and young adults (1–3).
The development of osteosarcoma is a complex,
multistep and multifactorial process in which numerous factors are
implicated (4–6). Several studies have been performed to
investigate cancer stem cells and the potential of these cells to
cause tumors (7,8). The concept that genetic factors are
involved in the development of osteosarcoma has led to numerous
studies investigating genetic determinants for osteosarcoma in the
past decade (10–13).
Vascular endothelial growth factor (VEGF) is one of
the most potent endothelial cell mitogens, and performs an
important role in angiogenesis (14,15). The
VEGF gene, which consists of eight exons that undergo alternative
splicing to form a family of proteins, is located at chromosome
6p21.3. It is well known that the VEGF gene results in several
alternatively spliced isoforms, and the regulation of VEGF
expression can reveal the difference between normal and tumor
tissues. It is estimated that there are >30 types of single
nucleotide polymorphism (SNP) in the VEGF gene (16), and several SNPs in the VEGF gene have
been reported to affect the expression of the VEGF gene (16). Among these SNPs, five common SNPs in
the VEGF gene, consisting of −2578C/A, −1156G/A, +1612G/A, +936C/T
and −634G/C, are reported to be associated with VEGF protein
synthesis (17). The −2578C/A and
−1156G/A SNPs are located at the VEGF promoter region, and the
+1612G/A, +936C/T and −634G/C SNPs are located at the
3′-untranslated region. Previous studies have reported that VEGF
polymorphisms are associated with the risk of several cancers,
including breast, prostate, renal cell and head and neck cancers
(18–20). However, studies reporting the
association between the five SNPs in the VEGF gene and
susceptibility to osteosarcoma are limited (21,22).
Therefore, the aim of the present study was to investigate the
association between five common SNPs in VEGF and the risk of
osteosarcoma, in addition to the role of the SNPs in the prognosis
of osteosarcoma.
Materials and methods
Participants
A hospital-based case-control study was performed in
the present study. A total of 186 patients with osteosarcoma and
186 age- and sex-matched healthy controls were enrolled into the
present study from the No. 4 Hospital of Jinan (Jinan, Shandong,
China) between January 2008 and December 2010. The patients with
osteosarcoma were newly-diagnosed and the diagnosis was
histopathologically confirmed by two independent pathologists. The
clinical and pathological information of the patients was
extracted, including Enneking stage (consisting of stages I, II and
III) (23), tumor location in the
extremities or other locations, histological type (consisting of
osteoblastic, chondroblastic, fibroblastic and mixed types),
presence of tumor metastasis, and family history of cancer. The
control subjects met the following criteria: No medical history of
any tumor or cancer; no family history of osteosarcoma or other
cancers in first-degree relatives; and matched with the same
nationality as the patients. The present study was approved by the
ethics committee of Jinan No. 4 Hospital, and each individual
provided written informed consent for participation in the present
study.
The demographic data and medical and family
histories were obtained by a face to face interview using a
self-designed questionnaire. The face to face interview was
completed by trained nurses or doctors.
All the patients were followed up until 30th
December 2012, with a median follow-up time of 35.6 months (range,
2–60 months). All patients were followed up by telephone every four
weeks until mortality or the end of the study. The overall survival
(OS) time was calculated from the date of enrolling in this study
to the date of mortality or last clinical follow-up.
Blood samples and genotyping
Each patient provided 5 ml of peripheral blood,
which was maintained at −70°C prior to use, and EDTA with 0.5 mg/ml
was used as an anticoagulant. Genomic DNA was isolated using the
TIANamp blood DNA kit (Tiangen, Beijing, China) according to the
manufacturer's instructions. Probes and primers for VEGF-2578C/A
(rs699947), −1156G/A (rs1570360), +1612G/A (rs10434), +936C/T
(rs3025039) and −634G/C (rs2010963) were designed using Primer 5.0
software (PREMIER Biosoft, Palo Alto, CA, USA). Polymerase chain
reaction restriction fragment length polymorphism (PCR-RFLP) assay
was conducted to determine the frequency of the VEGF-2578C/A,
−1156G/A, +1612G/A, +936C/T and −634 G/C polymorphisms. The PCR
reaction was conducted using a Perkin-Elmer 9700 thermocycler
(Perkin-Elmer, Waltham, MA, USA) with an initial denaturation step
of 5 min at 94°C, followed by 35 cycles of denaturing at 94°C for
45 sec, annealing at 62°C for 60 sec and extending at 72°C for 60
sec, and a final extension was performed at 72°C for 10 min. The
PCR products were visualized in 1.0% agarose gel electrophoresis
and stained using ethidium bromide staining and ultraviolet light.
In order to perform quality control, a randomly chosen subgroup of
10% of osteosarcoma cases was selected to repeat the genotyping,
and the reproducibility was 100%.
Statistical analysis
Continuous variables were expressed as the mean ±
standard deviation and were analyzed using a Student's
t-test. Categorical variables were expressed as the
frequency and percentage of study participants, and were analyzed
using the χ2-test. The Hardy-Weinberg equilibriums of
the VEGF −2578C/A, −1156G/A, +1612G/A, +936C/T and −634 G/C
genotype frequencies in the control subjects were analyzed using
the χ2-test. The differences in genotype frequencies
between the osteosarcoma and control groups were assessed using the
χ2-test, and the results were assessed in terms of odds
ratio (OR) and confidence intervals (CI). The hazard ratio (HR) and
95% CI were calculated by Cox proportional hazards models, and used
to evaluate the effect of the VEGF −2578C/A, −1156G/A, +1612G/A,
+936C/T and −634 G/C polymorphisms on the OS time of patients with
osteosarcoma. The Kaplan-Meier method was used to plot the OS
curves. P<0.05 was considered to indicate a statistically
significant difference, and all tests were two-tailed. All
statistical analyses were performed using SPSS statistical
software, version 16.0 (SPSS, Inc., Chicago, IL, USA) for
Windows.
Results
The characteristics of patients with osteosarcoma
and control individuals are shown in Table I. No significant differences were
identified between the gender and age at enrollment of patients and
control individuals in the present study. The mean age of patients
with osteosarcoma was 18.5±10.3 years and the mean age of control
individuals was 19.2±11.8 years. Of the 186 patients with
osteosarcoma, 125 patients (72.58%) possessed tumors of the long
tubular bones and 51 (27.42%) possessed tumors of the axial
skeleton. In total, metastasis was identified in 43 (23.12%)
patients at the time of enrollment in the present study.
 | Table I.Characteristics of the patients with
osteosarcoma and the control subjects. |
Table I.
Characteristics of the patients with
osteosarcoma and the control subjects.
| Characteristics | Osteosarcoma
group | Control group | t or
χ2 test | P-value |
|---|
| Total, n (%) | 186 (100.00) | 186 (100.00) |
|
|
| Age, years |
|
| 0.03 | 0.87 |
| Mean
age | 18.5±10.3 | 19.2±11.8) |
|
|
|
<20 | 119 (63.98) | 127 (68.28) |
|
|
|
>20 | 67 (36.02) | 69 (37.10) |
|
|
| Gender, n (%) |
|
| 0.00 | 1.00 |
| Male | 114 (61.29) | 114 (61.29) |
|
|
|
Female | 72 (38.71) | 72 (38.71) |
|
|
| Tumor location, n
(%) |
|
|
|
|
| Long
tubular bones | 135 (72.58) |
|
|
|
| Axial
skeleton | 51 (27.42) |
|
|
|
| Metastasis, n
(%) |
|
|
|
|
| No | 43 (23.12) |
|
|
|
| Yes | 143 (76.88) |
|
|
|
The frequency of the VEGF-2578C/A, −1156G/A,
+1612G/A, +936C/T and −634G/C genotypes in the osteosarcoma and
control groups are shown in Table
II. The genotype frequencies of the VEGF-2578C/A, −1156G/A,
+1612G/A, +936C/T and −634G/C SNPs were found to be in line with
the Hardy-Weinberg equilibrium. Conditional logistic regression
analysis revealed that subjects carrying the −634GG genotype
possessed a significantly increased risk of osteosarcoma, with an
adjusted OR (95% CI) of 2.00 (1.07–3.75). However, no significant
association was identified between the VEGF-2578C/A, −1156G/A,
+1612G/A and +936C/T SNPs and the risk of osteosarcoma.
| Table II.Genotype distribution of five SNPs in
VEGF gene between osteosarcoma cases and controls. |
Table II.
Genotype distribution of five SNPs in
VEGF gene between osteosarcoma cases and controls.
| SNPs | Genotype | Osteosarcoma, n
(%) | Control group, n
(%) | OR (95%
CI)a | P-value |
|---|
| −2578C/A | CC | 79
(42.47) | 87
(46.77) | 1.0 (Ref.) | – |
|
| CA | 75
(40.32) | 73
(39.25) | 1.13 (0.62–1.81) | 0.59 |
|
| AA | 32
(17.20) | 26
(13.98) | 1.36 (0.73–2.59) | 0.32 |
| −1156G/A | AA | 107 (57.53) | 116 (62.37) | 1.0 (Ref.) | – |
|
| AG | 53
(28.49) | 49
(26.34) | 1.17
(0.64–1.93) | 0.51 |
|
| GG | 27
(14.52) | 21
(11.29) | 1.39
(0.68–2.76) | 0.30 |
| +1612G/A | GG | 75
(40.32) | 84
(45.16) | 1.0 (Ref.) | – |
|
| GA | 86
(46.24) | 83
(44.62) | 1.16
(0.74–1.83) | 0.50 |
|
| AA | 25
(13.44) | 19
(10.22) | 1.47
(0.71–3.07) | 0.25 |
| +936C/T | CC | 125 (67.20) | 134 (72.04) | 1.0 (Ref.) | – |
|
| CT | 46
(24.73) | 42
(22.58) | 1.17
(0.66–1.96) | 0.52 |
|
| TT | 16 (8.60) | 10 (5.38) | 1.71
(0.71–4.39) | 0.20 |
| −634G/C | CC | 50
(26.88) | 69
(37.10) | 1.0 (Ref.) | – |
|
| CG | 91
(48.92) | 86
(46.24) | 1.46
(0.89–2.40) | 0.11 |
|
| GG | 45
(24.19) | 31
(16.67) | 2.00
(1.07–3.75) | 0.02 |
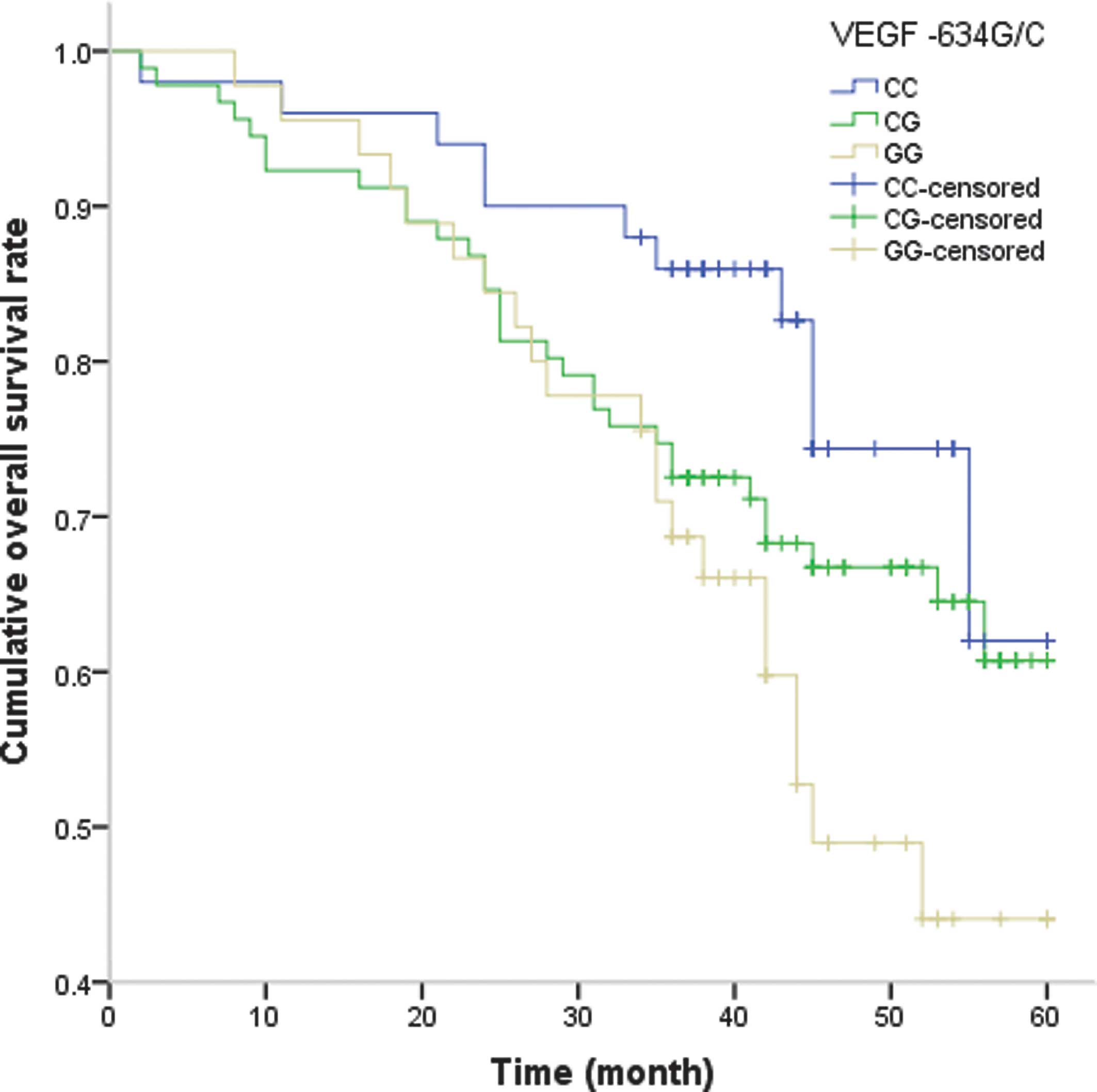
In addition, an analysis was performed to assess the
association between the five SNPs in the VEGF gene and the OS time
of patients with osteosarcoma (Table
III). During the follow-up period, 63 patients (33.87%)
succumbed to osteosarcoma during the follow-up period. In the Cox
proportional hazards model, subsequent to adjusting for potential
confounding factors, patients with osteosarcoma carrying the −634GG
genotype demonstrated a shorter OS time (HR, 3.10; 95% CI,
1.17–8.38), and the −634G/C polymorphism was therefore an
independent prognostic factor for osteosarcoma (Fig. 1). However, no significant association
was observed between the −2578C/A, −1156G/A, +1612G/A and +936C/T
polymorphisms and the OS time of patients with osteosarcoma.
| Table III.Role of five SNPs in VEGF gene in the
overall survival of osteosarcoma cases. |
Table III.
Role of five SNPs in VEGF gene in the
overall survival of osteosarcoma cases.
| SNPs | Genotype | Osteosarcoma group,
n (%) | Mortalities, n
(%) | Five-year survival
rate, % | HR (95%
CI)a | P-value |
|---|
| −2578C/A | CC | 79
(42.47) | 30 (47.62) | 87.10 | 1.0 (Ref.) | – |
|
| CA | 75
(40.32) | 24 (38.10) | 85.48 | 1.29
(0.62–2.67) | 0.46 |
|
| AA | 32
(17.20) | 9
(14.29) | 93.55 | 1.38
(0.52–3.51) | 0.47 |
| −1156G/A | AA | 107 (57.53) | 39 (61.90) | 81.72 | 1.0 (Ref.) | – |
|
| AG | 53
(28.49) | 17 (26.98) | 89.78 | 1.20
(0.56–2.53) | 0.61 |
|
| GG | 27
(14.52) | 7
(11.11) | 94.09 | 1.48
(0.55–3.81) | 0.38 |
| +1612G/A | GG | 75
(40.32) | 29 (46.03) | 87.63 | 1.0 (Ref.) | – |
|
| GA | 86
(46.24) | 28 (44.44) | 83.87 | 1.21
(0.59–2.48) | 0.57 |
|
| AA | 25
(13.44) | 6 (9.52) | 94.62 | 1.51
(0.52–4.22) | 0.39 |
| +936C/T | CC | 125 (67.20) | 45 (71.43) | 77.96 | 1.0 (Ref.) | – |
|
| CT | 46
(24.73) | 14 (22.22) | 90.86 | 1.20
(0.55–2.56) | 0.61 |
|
| TT | 16 (8.60) | 4 (6.35) | 96.24 | 1.59
(0.46–5.18) | 0.38 |
| −634G/C | CC | 50
(26.88) | 11 (17.46) | 78.00 | 1.0 (Ref.) | – |
|
| CG | 91
(48.92) | 31 (49.21) | 65.93 | 1.83
(0.78–4.51) | 0.13 |
|
| GG | 45
(24.19) | 21 (33.33) | 53.33 | 3.10
(1.17–8.38) | 0.01 |
Discussion
VEGF, a growth factor that regulates angiogenesis,
is localized on chromosome 6p21.3. In total, >30 SNPs have been
identified in this gene. VEGF is regarded as the most potent
stimulatory cytokine for the initiation of tumor angiogenesis and
is also an important factor for the development, metastasis,
survival and spread of the tumor (24). Previous studies have reported that the
expression of VEGF demonstrates an effect on the development and
prognosis of several types of cancer (18–20,25). The
VEGF-2578C/A, −1156G/A, +1612G/A, +936C/T and −634G/C SNPs have
been previously identified, and all the polymorphisms were found to
be located at the promoter region of VEGF. The five SNPs perform a
role in the alteration of the transcription of the VEGF gene and
also affect the expression of the VEGF gene. Several previous
clinical studies have revealed that the five SNPs are associated
with the development and prognosis of cancers (18–20,25). In
the present study, it was found that subjects carrying the −634GG
genotype possessed a significantly increased risk of osteosarcoma,
and this genotype was also associated with a shorter OS time in
patients with osteosarcoma. The present study suggested that the
−634G/C polymorphism may be an independent factor for the
development and prognosis of osteosarcoma.
The exact mechanism of the VEGF gene polymorphisms
on the susceptibility and clinical outcome of osteosarcoma remains
unknown. It is well known that angiogenesis is an important factor
for the development and prognosis of tumors, VEGF expression
regulates angiogenesis, and therefore VEGF may have been involved
in the promotion of endothelial cell proliferation and regulation
of the extracellular matrix in the blood vessels (26,27). The
present study identified that the −634G/C polymorphism affects the
development and prognosis of osteosarcoma. The VEGF-634G/C
polymorphism is located in the 5′- and 3′-UTR of VEGF, and this SNP
has been reported to influence the protein translation efficiency,
circulating plasma concentrations and expression of VEGF in tumor
tissues (28–30). Numerous studies have reported that the
VEGF-634G/C polymorphism is associated with several types of
cancers, including gastric, colorectal, lung and breast cancers
(30–33). Liu et al (30) reported that the VEGF-634GC+CC genotype
was associated with an increased risk of gastric cancer. The
present study is consistent with these results. However, Zhao et
al (31) and Deng et al
(32) revealed that the VEGF-634CC
genotype decreased the risk of colorectal and lung cancers. Yao
et al (33) reported that the
−634G/C polymorphism does not appear to represent a risk factor for
breast cancer. The inconsistent role of the −634G/C polymorphism
may be due to the association between −634G/C and other unknown
functional SNPs or environmental factors in the angiogenesis
pathway. In addition, the variations in ethnicities, study design,
tumor types and sample size demonstrated by these studies may
affect the results and cause such discrepancies. Therefore,
additional studies with different populations are required to
confirm the association between this polymorphism and the risk of
cancer.
In the present study, it was found that the −634G/C
polymorphism is associated with the prognosis of osteosarcoma.
Previous studies have reported that −634G/C polymorphism is
associated with the clinical outcome of breast, gastric, prostate
and ovarian cancers (33–36). One study investigated the association
between VEGF polymorphism and the prognosis of osteosarcoma, but
this previous study did not identify that the −634G/C polymorphism
played a role in the clinical outcome of osteosarcoma (37). Additional studies are required to
confirm the association between this polymorphism and
osteosarcoma.
Several limitations should be considered in the
present study. First, the enrolled patients and control individuals
were selected from one hospital. A certain risk of selection bias
may be present, as the patients and control individuals were not a
random sample of patients with osteosarcoma and may not be
representative of the overall situation of patients with
osteosarcoma. Secondly, due to the rarity of osteosarcoma, only a
small number of patients with osteosarcoma were enrolled. The
relatively small sample size may limit the statistical power to
identify differences between groups. Thirdly, additional factors in
the angiogenesis pathway may affect the development and prognosis
of osteosarcoma, and the VEGF gene polymorphism may interact with
these factors. Therefore, additional large samples are required to
confirm the association between VEGF gene polymorphisms and the
development and prognosis of osteosarcoma.
In summary, the present study revealed that the
VEGF-634G/C polymorphism is an independent factor for the
development and prognosis of osteosarcoma. The VEGF-634G/C
polymorphism may be used as a genetic marker for the prediction of
the risk and clinical outcome of osteosarcoma.
References
|
1
|
Mirabello L, Troisi RJ and Savage SA:
Osteosarcoma incidence and survival rates from 1973 to 2004: Data
from the Surveillance, Epidemiology, and End Results Program.
Cancer. 115:1531–1543. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ottaviani G and Jaffe N: The epidemiology
of osteosarcoma. Cancer Treat Res. 152:3–13. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Picci P: Osteosarcoma (osteogenic
sarcoma). Orphanet J Rare Dis. 2:62007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Powers M, Zhang W, Lopez-Terrada D,
Czerniak BA and Lazar AJ: The molecular pathology of sarcomas.
Cancer Biomark. 9:475–491. 2010.PubMed/NCBI
|
|
5
|
Bovée JV and Hogendoorn PC: Molecular
pathology of sarcomas: Concepts and clinical implications. Virchows
Arch. 456:193–199. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
de Álava E: Molecular pathology in
sarcomas. Clin Transl Oncol. 9:130–144. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Osuna D and de Alava E: Molecular
pathology of sarcomas. Rev Recent Clin Trials. 4:12–26. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Berger M, Muraro M, Fagioli F and Ferrari
S: Osteosarcoma derived from donor stem cells carrying the Norrie's
disease gene. N Engl J Med. 359:2502–2504. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
He M, Wang Z, Zhao J, Chen Y and Wu Y:
COL1A1 polymorphism is associated with risks of osteosarcoma
susceptibility and death. Tumour Biol. 35:1297–1305. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
He ML, Wu Y, Zhao JM, Wang Z and Chen YB:
PIK3CA and AKT gene polymorphisms in susceptibility to osteosarcoma
in a Chinese population. Asian Pac J Cancer Prev. 14:5117–5122.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jia J, Tian Q, Liu Y, Shao ZW and Yang SH:
Interactive effect of bisphenol A (BPA) exposure with −22G/C
polymorphism in LOX gene on the risk of osteosarcoma. Asian Pac J
Cancer Prev. 14:3805–3808. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang SL, Mao NF, Sun JY, Shi ZC, Wang B
and Sun YJ: Predictive potential of glutathione S-transferase
polymorphisms for prognosis of osteosarcoma patients on
chemotherapy. Asian Pac J Cancer Prev. 13:2705–2709. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang W, Wang J, Song H, Liu J, Song B and
Cao X: Cytotoxic T-lymphocyte antigen-4 +49G/A polymorphism is
associated with increased risk of osteosarcoma. Genet Test Mol
Biomarkers. 15:503–506. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Patard JJ, Pouessel D, Bensalah K and
Culine S: Targeted therapy in renal cell carcinoma. World J Urol.
26:135–140. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Motzer RJ, Hutson TE, Tomczak P,
Michaelson MD, Bukowski RM, Rixe O, Oudard S, Negrier S, Szczylik
C, Kim ST, et al: Sunitinib versus interferon alfa in metastatic
renal-cell carcinoma. N Engl J Med. 356:115–124. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Watson CJ, Webb NJ, Bottomley MJ and
Brenchley PE: Identification of polymorphisms within the vascular
endothelial growth factor (VEGF) gene: Correlation with variation
in VEGF protein production. Cytokine. 12:1232–1235. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jain L, Vargo CA, Danesi R, Sissung TM,
Price DK, Venzon D, Venitz J and Figg WD: The role of vascular
endothelial growth factor SNPs as predictive and prognostic markers
for major solid tumors. Mol Cancer Ther. 8:2496–2508. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yan Y, Liang H, Li T, Guo S, Li M, Li S
and Qin X: Vascular endothelial growth factor +936C/T polymorphism
and breast cancer risk: A meta-analysis of 13 case-control studies.
Tumour Biol. 35:2687–2692. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Martinez-Fierro ML, Garza-Veloz I,
Rojas-Martinez A, Ortiz-Lopez R, Castruita-de la Rosa C,
Ortiz-Castro Y, Lazalde-Ramos BP, Cervantes-Villagrana AR,
Castañeda-Lopez ME, Gomez-Guerra L, et al: Positive association
between vascular endothelial growth factor (VEGF) −2578 C/A variant
and prostate cancer. Cancer Biomark. 13:235–241. 2013.PubMed/NCBI
|
|
20
|
Zhang Y, Li S, Xiao HQ, Hu ZX, Xu YC and
Huang Q: Vascular endothelial growth factor gene polymorphisms and
renal cell carcinoma: A systematic review and meta-analysis. Oncol
Lett. 6:1068–1078. 2013.PubMed/NCBI
|
|
21
|
Wang Z, Wen P, Luo X, Fang X, Wang Q, Ma F
and Lv J: Association of the vascular endothelial growth factor
(VEGF) gene single-nucleotide polymorphisms with osteosarcoma
susceptibility in a Chinese population. Tumour Biol. 35:3605–3610.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tie Z, Bai R, Zhai Z, Zhang G, Zhang H,
Zhao Z, Zhou D and Liu W: Single nucleotide polymorphisms in VEGF
gene are associated with an increased risk of osteosarcoma. Int J
Clin Exp Pathol. 7:8143–8149. 2014.PubMed/NCBI
|
|
23
|
Enneking WF, Spanier SS and Goodman MA: A
system for the surgical staging of musculoskeletal sarcoma. Clin
Orthop Relat Res. 106–120. 1980.PubMed/NCBI
|
|
24
|
Salven P, Teerenhovi L and Joensuu H: A
high pretreatment serum vascular endothelial growth factor
concentration is associated with poor outcome in non-Hodgkin's
lymphoma. Blood. 90:3167–3172. 1997.PubMed/NCBI
|
|
25
|
Leng WD, He MN, Chen QL, Gong H, Zhang L
and Zeng XT: Vascular endothelial growth factor (VEGF) gene
polymorphisms and risk of head and neck cancer: A meta-analysis
involving 2,444 individuals. Mol Biol Rep. 40:5987–5992. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kushner EJ and Bautch VL: Building blood
vessels in development and disease. Curr Opin Hematol. 20:231–236.
2013.PubMed/NCBI
|
|
27
|
Roy H, Bhardwaj S and Ylä-Herttuala S:
Biology of vascular endothelial growth factors. FEBS Lett.
580:2879–2887. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Renner W, Kotschan S, Hoffmann C,
Obermayer-Pietsch B and Pilger E: A common 936 C/T mutation in the
gene for vascular endothelial growth factor is associated with
vascular endothelial growth factor plasma levels. J Vasc Res.
37:443–448. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Koukourakis MI, Papazoglou D,
Giatromanolaki A, Bougioukas G, Maltezos E and Sivridis E: VEGF
gene sequence variation defines VEGF gene expression status and
angiogenic activity in non-small cell lung cancer. Lung Cancer.
46:293–298. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Liu H, Wang S and Huang C: VEGFA+936C/T
and −634G/C polymorphisms and gastric cancer risk: A meta-analysis.
Asian Pac J Cancer Prev. 12:1979–1983. 2011.PubMed/NCBI
|
|
31
|
Zhao Z, Ba C, Wang W, Wang X, Xue R and Wu
X: Vascular endothelial growth factor (VEGF) gene polymorphisms and
colorectal cancer: A meta-analysis of epidemiologic studies. Genet
Test Mol Biomarkers. 16:1390–1394. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Deng ZC, Cao C, Yu YM, Ma HY and Ye M:
Vascular endothelial growth factor −634G/C and vascular endothelial
growth factor −2578C/A polymorphisms and lung cancer risk: A
case-control study and meta-analysis. Tumour Biol. 35:1805–1811.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yao W, Yan R, Ma L, Wan H, Yu Y, Cheng X
and Li Y: Vascular endothelial growth factor gene polymorphism
(−634G/C) and breast cancer risk. Tumour Biol. 35:7793–7798. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sa-Nguanraksa D, Chuangsuwanich T,
Pongpruttipan T, Kummalue T, Rojananin S, Ratanawichhitrasin A,
Prasarttong-Osoth P, Chuthatisith S, Pisarnturakit P,
Aeumrithaicharoenchok W, et al: Vascular endothelial growth factor
634G/C polymorphism is associated with increased breast cancer risk
and aggressiveness. Mol Med Rep. 8:1242–1250. 2013.PubMed/NCBI
|
|
35
|
Liao WC, Lin JT, Wu CY, Huang SP, Lin MT,
Wu AS, Huang YJ and Wu MS: Serum interleukin-6 level but not
genotype predicts survival after resection in stages II and III
gastric carcinoma. Clin Cancer Res. 14:428–434. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sfar S, Saad H, Mosbah F and Chouchane L:
Combined effects of the angiogenic genes polymorphisms on prostate
cancer susceptibility and aggressiveness. Mol Biol Rep. 36:37–45.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Hefler LA, Mustea A, Könsgen D, Concin N,
et al: Vascular endothelial growth factor gene polymorphisms are
associated with prognosis in ovarian cancer. Clin Cancer Res.
13:898–901. 2007. View Article : Google Scholar : PubMed/NCBI
|