Introduction
It is understood that myelodysplastic syndrome (MDS)
may be considered to precede acute non-lymphoblastic leukemia
(pre-ANLL), and this concept has reached a consensus (1,2). However,
to date, pre-ALL remains a rare and uncertain condition. A number
of studies have demonstrated that transient pancytopenia, another
bone marrow disorder, may be associated with ALL in children and
adolescents (3,4). The typical pancytopenic phase, which
lasts from several weeks to several months, is transient, followed
by spontaneous remission or remission induced by corticosteroids,
and subsequent transformation into common ALL (5). The prognosis of patients with ALL with
or without pre-ALL is similar following standard chemotherapy
(5). The situation can not be
determined in adult patients because such cases are exceedingly
rare.
Adult ALL with pancytopenia as a preceding symptom
is rare, difficult to diagnose early and prone to misdiagnosis
(6–8).
The present study reports a case of transient pancytopenia
preceding adult ALL with complex chromosomal abnormalities,
including Philadelphia chromosome and P190 breakpoint cluster
region (BCR)-ABL. The genetic characteristics and clinical outcome
of the patient are summarized. The present study aimed to improve
understanding of the etiology and pathogenesis underlying adult
ALL.
Case report
A 50-year-old female was admitted The Second
Affiliated Hospital of Zhejiang University School of Medicine
(Hangzhou, China) on 27 Februrary 2013, with a cough, fever,
fatigue and severe anemia for 1 week. The patient experienced
chills and a fever up to 39.5°C with cough, sputum, chest tightness
and shortness of breath, which were resistant to antibiotics
(ceftazidine administered via injection, 1.0 g every 8 h). Physical
examination revealed an anemic complexion, slight petechiae in the
skin and moist rales in the lungs. No enlargement of the lymph
nodes, liver or spleen was detected. No abnormalities were
identified in the patient's medical history or family history.
Laboratory tests were performed on the day of admittance and
revealed anemia with reticulocytopenia (hemoglobin, 30 g/l; normal
range, 110–160 g/l), leucopenia (white blood cells,
0.4×109/l; normal range, 4.0–10.0×109/l) and
thrombocytopenia (platelets, 17×109/l; normal range,
100–300×109/l). The results of blood biochemical
analysis indicated hypoalbuminemia (albumin, 26.6 g/l; normal
range, 35.0–52.0 g/l) and a marked increase in C-reactive protein
levels (122.5 mg/l; normal range, <6.0 mg/l). An initial bone
marrow (BM) smear and biopsy showed pancytopenia, significantly
reduced numbers of nucleated cells, significantly decreased
precursor myelocytes and relatively increased lymphocyte levels,
while no marked abnormalities were identified in erythroid or
megakaryocytic hematopoietic cell distribution. Flow cytometric and
karyotype analyses were not able to be conducted due to the
scarcity of nucleated cells. Cluster of differentiation 55
(CD55)/CD59 expression in erythrocytes and granulocytes was normal.
The urinary hemosiderin test, as well as direct and indirect
Coombs' tests were negative. Viral serologic studies, including
hepatitis A, B and C virus, human immunodeficiency virus,
Epstein-Barr virus and cytomegalovirus were negative, and
fluorescent nucleic acid detection of parvovirus B19 was also
negative. A pulmonary computed tomography (CT) scan revealed
infectious lesions in the lungs, with little pleural effusion.
B-mode ultrasound showed no notable abnormalities of the liver,
gallbladder, pancreas or spleen and no significant enlargements of
the lymph nodes. Acute arrest of hemopoiesis (AAH) and pulmonary
infection were diagnosed. The patient was therefore treated with
antibiotics (imipenem and cilastatin sodium administered via
injection, 0.5 g every 8 h), red blood cell and platelet
transfusion, granulocyte colony-stimulating factor and human γ
globulin. The condition of the patient rapidly improved, and white
blood cell, hemoglobin and platelet levels had increased three
weeks later (Table I). The BM was
reviewed and revealed normal hematopoiesis without excessive blast
cells or dysplasia. Re-examination via pulmonary CT indicated that
the infectious lesions had significantly remitted. The patient was
subsequently discharged 22 days following discharge and normal
peripheral blood test results were achieved at weekly
follow-ups.
 | Table I.Complete blood counts of the present
patient at the time of initial diagnosis of AAH, at discharge
following recovery of pancytopenia and at the established diagnosis
of ALL. |
Table I.
Complete blood counts of the present
patient at the time of initial diagnosis of AAH, at discharge
following recovery of pancytopenia and at the established diagnosis
of ALL.
| Parameter | At diagnosis of
AAH | Following
recovery | At diagnosis of
ALL |
|---|
| Time, weeks | 0 | 3 | 7 |
| Hemoglobin, g/l | 30 | 98 | 104 |
| Leukocytes,
×109/l | 0.4 | 5.6 | 291.3 |
| Neutrophils,
×109/l |
| 4.9 | 24.7 |
| Platelets,
×109/l | 17 | 128 | 18 |
| Peripheral blood
blasts, % | 0 | 0 | 85 |
However the patient was readmitted high fever three
weeks following discharge. Routine blood tests revealed
leukocytosis, mild anemia and thrombocytopenia. The peripheral
blood test identified a white blood cell count of
291.3×109/l (normal range, 4.0–10.0×109/l),
hemoglobin levels of 104 g/l (normal range, 110–160 g/l), platelet
levels of 18×109/l (normal range,
100–300×109/l) and 85% blast cells (Table I, day 50). Extensive lymphadenopathy
and splenomegaly were confirmed by B-mode ultrasound. BM
examination showed extreme hyperplasia with 65% excess blast cells
and inhibited normal hematopoiesis function. Blast cells accounted
for 87% of bone marrow cells, as indicated by immunophenotyping,
which had positive expression of membrane antigens, including
HLA-DR, CD10, CD15, CD19, CD20, CD22, CD34, CD38, CD123, CD79a and
terminal deoxynucleotidyl transferase. All available leukemia
fusion genes were examined, and positive BCR/ABL (P190) was
detected. The remaining fusion genes, including MLL/AFX, MLL/AF1P,
MLL/AF4, dupMLL, MLL/ENL, E2A/PBX1, SIL/TAL1, HOX11, TEL/AML1 and
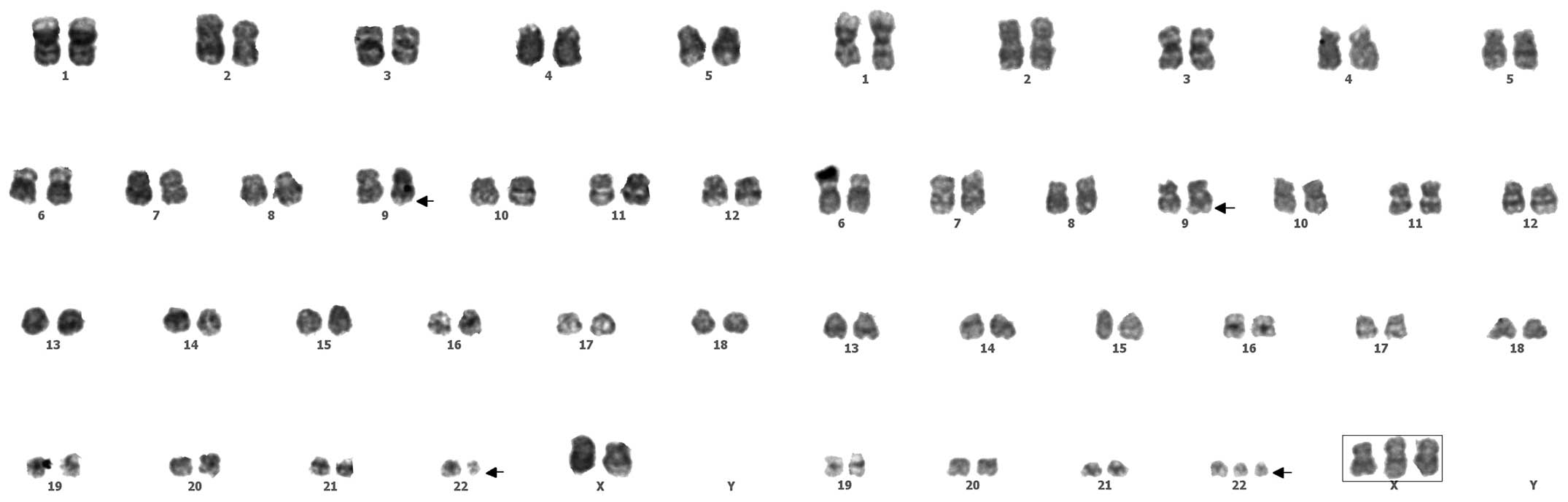
TEL/ABL, were all negative. Complex chromosomal mutations were
detected during karyotype analysis (Fig.
1). A final diagnosis of acute B-cell lymphoblastic leukemia
was reached. The patient refused imatinib treatment due to economic
problems, and was therefore administered VDP regimen chemotherapy
(50 mg daunorubicin on days 1–3; 2 mg vincristin on days 1, 8, 15
and 22; 60 mg prednisone on days 1–21 and 30 mg prednisone on days
22–28). Although complete remission was achieved following one
therapeutic course, the patient discontinued treatment and was lost
to follow-up.
Discussion
A number of studies have indicated that certain
cases of ALL may manifest preceding symptoms of hematopoietic
disorders (pre-ALL), and that the prevalence of pre-ALL is 1.3–2.2%
among children with ALL (3). Pre-ALL
is characterized by fever with pancytopenia as the primary symptom,
which is typically observed in children <10 years old, and has
markedly higher incidence amongst girls. ALL with pre-ALL has a
similar prognosis compared with that of ALL patients without
preceding symptoms of pancytopenia (5).
In the present case, laboratory tests identified
neutropenia, severe anemia and a relatively mild decrease or no
decrease at all in platelets. BM smear and biopsy showed
significantly reduced numbers of nucleated cells, but no notable
morphological abnormalities. A previous study reported that the
majority of these patients restored normal hematopoiesis within 1
month following treatment, but subsequently developed ALL within 6
months (3–5).
However, cases of adult ALL manifesting pancytopenia
are rare, and may be easily neglected or misdiagnosed; few cases
were available in the literature (8,9). In the
present case, symptoms of leukemia were not identified in
peripheral blood or BM on initial examination. The patient
presented with pancytopenia in peripheral blood and suppressed
myeloproliferation in the BM, but these symptoms were rapidly
restored to normal following active treatment. The initial
diagnosis was, therefore, AAH. AAH is also termed spontaneous
remission of aplastic anemia, the attacks last several weeks and
may be associated with external factors such as drug or infection
(10). Certain risk factors may
result in hemopoiesis dysfunction or decompensation, which
manifests as a transient decrease or absence of hematopoietic
cells. This situation may attenuate once the factors have been
removed (11). Common risk factors
include infection (particularly viruses), drugs, various nutrients
deficiencies and immune disorders (11). In the present case, three weeks
following admission, normal hematopoiesis in the BM was restored.
However, once the disease progressed, it was able to be diagnosed
as acute leukemia, characterized by the abnormal proliferation of
leukocytes.
In addition, complex chromosomal abnormalities,
including the Philadelphia (Ph) chromosome, were identified by
karyotype analysis in the present case. Therefore, when a patient
is diagnosed with AAH without clear etiology, the disease should be
monitored more carefully and more detailed BM examinations,
including immunophenotyping and karyotype analysis, should be
conducted. Ph chromosome is characteristic of chronic myeloid
leukemia, which may also be observed in 2–5% of ALL in children and
15–30% of adult ALL (12). Positivity
for the Philadelphia chromosome is an independent prognostic
indicator for adult ALL, predicting the poor efficacy of
conventional chemotherapy, low remission rate and decreased time
prior to relapse. Imatinib-based combined chemotherapy followed by
allogeneic hematopoietic stem cell transplantation is the
first-line treatment for Philadelphia chromosome-positive ALL
(13).
Associations between preceding symptoms of
hematopoietic disorders and subsequent ALL remain controversial.
Whether the pre-ALL period and the subsequent ALL period are
distinct clinical manifestations of one disease or not requires
further clarification. Since it is difficult to explain how pre-ALL
transforms into ALL over the period of a few days to several weeks,
the hypothesis that leukemia occurs prior to pre-ALL may be
plausible (14). Numerous
retrospective studies in children have indicated that pediatric
patients have normal chromosomes during the pancytopenic period and
then abnormal karyotypes may be detected in the ALL period
(3,14). For this reason, it has been suggested
that the former and the latter are distinct stages of one disease.
For example, cells with a normal karyotype proliferate in the forms
of colonization, followed by abnormal chromosome changes that
manifest as the clinical symptoms of typical ALL (14,15). It
has therefore been hypothesized that the pancytopenic period
observed in such patients occurred as a result of the inherent
characteristics of leukemia cells.
Certain studies have reported that parvovirus B19
infection is associated with the inhibited status of bone marrow in
pre-ALL children (16), and that
children infected by parvovirus B19 are more susceptible to severe
anemia (17). However, there was no
evidence of such viral infection in the present patient.
In conclusion, to the best of our knowledge, this
was the first report of adult transient pancytopenia preceding ALL
with complicated chromosomal abnormalities, including the
Philadelphia chromosome and P190 BCR-ABL. Further investigations
are required to elucidate the etiology and pathology of pre-ALL in
adults.
References
|
1
|
Wegelius R: Bone marrow dysfunctions
preceding acute leukemia in children: A clinical study. Leuk Res.
16:71–76. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shi J, Shao ZH, Liu H, Bai J, Cao YR, He
GS, Tu MF, Wang L, Hao YS, Yang TY and Yang CL: Transformation of
myelodysplastic syndromes into acute myeloid leukemias. Chin Med J
(Engl). 117:963–967. 2004.PubMed/NCBI
|
|
3
|
Hasle H, Heim S, Schroeder H, Schmiegelow
K, Ostergaard E and Kerndrup G: Transient pancytopenia preceding
acute lymphoblastic leukemia (pre-ALL). Leukemia. 9:605–608.
1995.PubMed/NCBI
|
|
4
|
Villarreal-Martínez L, Jaime-Pérez JC,
Rodríguez-Martínez M, González-Llano O and Gómez-Almaguer D: Acute
lymphoblastic leukemia of childhood presenting as aplastic anemia:
Report of two cases. Rev Bras Hematol Hemoter. 34:165–167. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Armata J, Grześkowiak-Melanowska J,
Balwierz W, Najbar-Pabian A and Pawlik-Niesytto E: Prognosis in
acute lymphoblastic leukemia (ALL) in children preceded by an
aplastic phase. Leuk Lymphoma. 13:517–518. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhao H, Zhang L, Zhu X, Chen Y, Zou Y,
Zhang L, Yang R and Han ZC: Transient pancytopenia preceding T
lineage acute lymphoblastic leukemia. Acta Haematol. 112:167–169.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li Q, Chen Z, You Y and Zou P: Transient
pancytopenia preceding acute lymphoblastic leukemia with positive
Philadelphia chromosome. Leuk Res. 32:1317–1320. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kelly K and Murphy P: Aplastic anaemia
preceding acute lymphoblastic leukaemia in an adult with isolated
deletion of chromosome 9q. Leuk Res. 32:1936–1938. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sohn SK, Suh JS, Lee J and Lee KB:
Pancytopenic prodrome (pre-ALL) of acute lymphoblastic leukemia in
adults: possible pathogenesis. Korean J Intern Med. 13:64–67. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee JH, Lee JH, Shin YR, Lee JS, Kim WK,
Chi HS, Park CJ and Lee KH: Spontaneous remission of aplastic
anemia: A retrospective analysis. Haematologica. 86:928–933.
2001.PubMed/NCBI
|
|
11
|
Bozkaya H, Yurdaydin C, Törüner M, Arat M,
Bozdayi AM, Erekul S, Cinar K, Koç H and Uzunalimoğlu O: Remission
of severe aplastic anemia associated with hepatitis B virus
infection after viral clearance: Potential role of lamivudine. Dig
Dis Sci. 47:1782–1785. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Majlis A, Smith TL, Talpaz M, O'Brien S,
Rios MB and Kantarjian HM: Significance of cytogenetic clonal
evolution in chronic myelogenous leukemia. J Clin Oncol.
14:196–203. 1996.PubMed/NCBI
|
|
13
|
Adele K: Current treatment of Philadelphia
chromosome-positive acute lymphoblastic leukemia. Haematologica.
95:8–12. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Matloub YH, Brunning RD, Arthur DC and
Ramsay NK: Severe aplastic anemia preceding acute lymphoblastic
leukemia. Cancer. 71:264–268. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Horsley SW, Colman S, McKinley M, Bateman
CM, Jenney M, Chaplin T, Young BD, Greaves M and Kearney L: Genetic
lesions in a preleukemic aplasia phase in a child with acute
lymphoblastic leukemia. Genes Chromosomes Cancer. 47:333–40. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Heegaard ED, Madsen HO and Schmiegelow K:
Transient pancytopenia preceding acute lymphoblastic leukaemia
(pre-ALL) precipitated by parvovirus B19. Br J Haematol.
114:810–813. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kishore J, Sen M and Kumar A and Kumar A:
A pilot study on parvovirus B19 infection in paediatric
haematological malignancies. Indian J Med Res. 133:407–413.
2011.PubMed/NCBI
|