Introduction
Advanced pancreatobiliary tract cancer has a poor
prognosis, despite recent advances in systemic treatments. Although
gemcitabine (GEM) has been the reference regimen, demonstrating a
clinical benefit and prolonging survival, survival times remain
short (1). More intensive and
combined chemotherapy regimens with platinum agents (e.g.,
cisplatin or oxaliplatin), erlotinib or nab-paclitaxel have been
developed and represent an area of great interest; however, it
remains difficult to achieve >1-year survival, and intensive
side effect management is required (2–4). Compared
with pancreatobiliary tract cancer, urothelial carcinoma is
slightly less aggressive and more chemosensitive, and the
GEM/cisplatin (GC) regimen is generally considered to be the
current standard care for metastatic cases, replacing the
methotrexate/vinblastin/doxorubicin/cisplatin regimen (5). Thus, GEM is a key drug in the
chemotherapeutic treatment of pancreatobiliary tract and urothelial
carcinoma, and may be used alone or in combination with other
anticancer drugs. Its dose is practically determined based on the
patient's body surface area, and is adjusted according to patient
age, hematological data, adverse events, and other factors
(6–8).
However, when determining its administration or doses, there are
few useful adjunct indices that may be used easily and
non-invasively to understand the patient's condition and to predict
changes in their pathological state.
The importance of body composition measurement in
the clinical setting has been increasing in recent years. The
prevalence of obesity has become a public health problem, in
association with cardiovascular disease, throughout the world,
particularly in developed countries. Loss of skeletal muscle mass
is associated with impaired mobility and lower quality of life
(9). Magnetic resonance imaging (MRI)
is considered to be the most precise and reliable method for
measuring skeletal muscle in vivo (10), whilst the adipose tissue distribution
is commonly evaluated by computed tomography (CT) or MRI (11,12).
However, there is emerging interest in the use of bioelectrical
impedance (BI) analysis to assess body fat and skeletal muscle
mass, and numerous studies have developed equations for estimating
body compositions using the BI method (13–15). The
principle of BI analysis is based upon the greater electrolyte
content of fat-free mass and its greater conductivity of
electricity compared with that of adipose tissue or bone. The
majority of the BI current flows through skeletal muscle as this
has a large volume and a low resistance (16). BI is now becoming more widely used as
simple, safe and inexpensive method for estimating body
composition. However, as the BI method was developed primarily by
analyzing healthy subjects, applying it to a patient care is not
sufficiently understood at present.
Therefore, the current study retrospectively
analyzed the body composition rates measured over time in patients
who were being treated with GEM-based chemotherapy on an outpatient
basis.
Patients and methods
Patients
The study subjects were 37 patients (26 with
pancreatobiliary tract cancer and 11 with urothelial carcinoma) who
were treated with GEM-based chemotherapy at the Chemotherapy Unit
for Outpatients of Ageo Central General Hospital (Ageo, Japan)
between November 2012 and April 2014. All outpatients who were
eligible to receive GEM-based chemotherapy were included in the
study. Standardized inclusion criteria for chemotherapy in the
outpatient unit were an Eastern Cooperative Oncology Group (ECOG)
performance status score of 0, 1 or 2 (17) and adequate bone marrow, liver and
renal function (white blood cell count, ≥2,000/mm3;
platelet count, ≥70,000/mm3; bilirubin, ≤3.0 mg/dl;
aspartate transaminase/alanine aminotransferase, ≤150 IU/l; and
creatinine, ≤1.5 mg/dl). Patient characteristics are summarized in
Table I. This study was conducted
after obtaining informed consent from all the patients, and with
approval from the ethics committee of Ageo Central General
Hospital.
 | Table I.Characteristics of patients
(n=37). |
Table I.
Characteristics of patients
(n=37).
| Cancer type | Patients, n | Treatment
regimens | Age, years; mean
(range) | BMI at treatment
initiation, kg/m2; mean (range) |
|---|
| Pancreatic
cancer | 16 | GEM (n=15); GEM/S-1
(n=1) |
|
|
|
Female | 10 |
| 69.3 (50–82) | 19.7
(18.6–24.4) |
|
Male | 6 |
| 63.5 (47–76) | 20.7
(18.4–22.7) |
| Biliary cancer | 10 | GEM (n=9); GEM/CDDP
(n=1) |
|
|
|
Female | 2 |
| 71.0 (67–75) | 19.5
(17.3–21.6) |
|
Male | 8 |
| 67.7 (62–83) | 21.4
(15.6–25.7) |
| Urothelial
cancer | 11 | GEM (n=4);
CBDCA/GEM (n=7) |
|
|
|
Female | 2 |
| 69.4 (60–79) | 25.8
(25.3–26.2) |
|
Male | 9 |
| 68.9 (60–74) | 24.2
(19.7–27.3) |
Measurement of the body composition
rate
At each visit for chemotherapy, the total weight
(kg), body fat rate (%), skeletal muscle rate (%), body mass index
(BMI), and basal metabolism of the subjects were measured as body
composition parameters using a BI method-based body weight/body
composition monitor (Karada Scan HBF-375; Omron Corporation, Kyoto,
Japan). When using this measurement method, an electric
microcurrent was applied with the patient in a standing position,
between the hands and feet to the whole body, including the
abdomen; measurements were obtained by subtracting the impedance
value between both hands from the impedance value of the whole body
(18,19). Following the acquisition of these
values, the measurement was calculated by factoring in the height,
weight, age, gender and basic physical data of the patients; Omron
(http://www.omron.com/) has used research
information from several hundred subjects using the
hydrodensitometry method to develop the formulas by which the Omron
composition monitor calculates the various body composition rates
(19–28). In the current study, a retrospective
analysis was conducted of the associations between the measurement
results (i.e., the aforementioned body composition parameters) and
various other factors, including the following: Relative dose
intensity (RDI; dose intensity / planned dose intensity × 100) of
the GEM; adverse events [according to Common Terminology Criteria
for Adverse Events (CTCAE) version 4.03; U.S. Department of Health
and Human Service, National Institutes of Health and National
Cancer Institute]; ECOG performance status (PS); and progression of
the pathological conditions in the subjects evaluated by Response
Evaluation Criteria in Solid Tumors guidelines, version 1.1
(29).
Statistical analysis
Microsoft Excel with the Statcel Add-in, 2nd Edition
(OMS publishing Inc., Saitama, Japan) was used as the analytical
software (30). The association
between RDI and body composition was tested using a Pearson's
correlation coefficient test; body composition rates and adverse
events were tested using a repeated measures two-way analysis of
variance, and changes in body composition and in pathological
conditions were tested with cross analysis and comparative tests.
P<0.05 was considered to indicate statistically significant
differences in all tests.
Results
Patient characteristics
Of 26 patients with pancreatobiliary tract cancer,
10 were able to receive long-term (>6 months) GEM-based
chemotherapy, and 11 received adjuvant chemotherapy. All 11
patients with urothelial carcinoma had progressive recurrent
cancer. In addition, the age at disease onset and BMI of patients
with pancreatobiliary tract cancer and urothelial carcinoma were
close to the average for that of the general Japanese population
(Table I) (31).
Changes in pathological conditions and
body composition over time
Of the 26 patients with pancreatobiliary tract
cancer, 14 became unable to continue GEM-based chemotherapy due to
progressive disease (PD) or a decreased PS; in these 14 patients,
body fat rate had markedly decreased prior to the discontinuation
of chemotherapy. Representative changes in body composition over
time are presented in Fig. 1A–G.
Compared to the start of the GEM administration, there was a
statistically significant decrease in the amount of body fat at
discontinuation (Figs. 1 and 2A; P=0.01). An increased body weight and
skeletal muscle rate were observed in 3 of the 4 patients in whom
the chemotherapy was discontinued due to ascites retention
associated with the progression of pathological conditions;
however, a decrease in body fat rate was observed (Fig. 1F and G). The body fat rate increased
along with an improvement in PS and general conditions in 3
patients who had undergone biliary drainage due to the onset of
jaundice during chemotherapy (Fig.
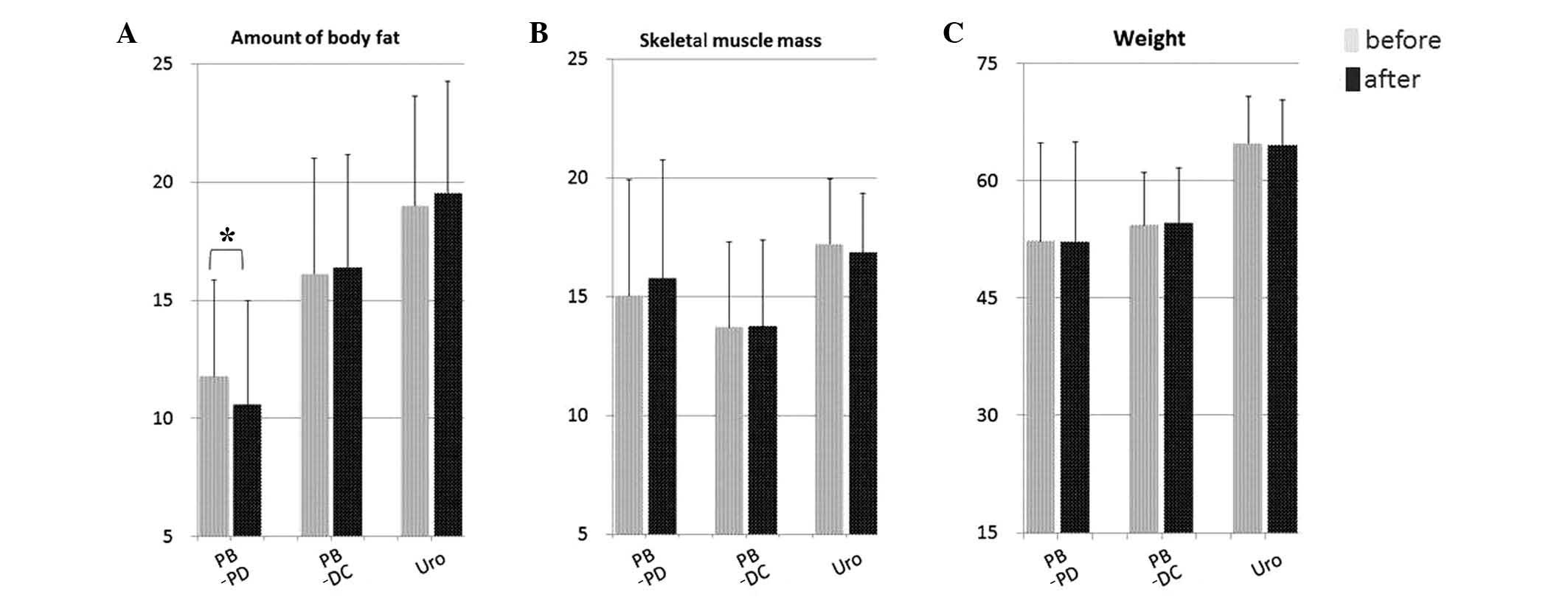
1H). Meanwhile, a stable body composition was maintained in 6
of 7 patients with no progression of disease or a complete
response/disappearance of the lesion during chemotherapy (Figs. 1I and 2). No significant differences in body
composition were observed over time in the control patients with
progressive urothelial carcinoma who were similarly treated with
GEM-based chemotherapy, despite the progression of pathological
conditions (Figs. 1J–K and 2).
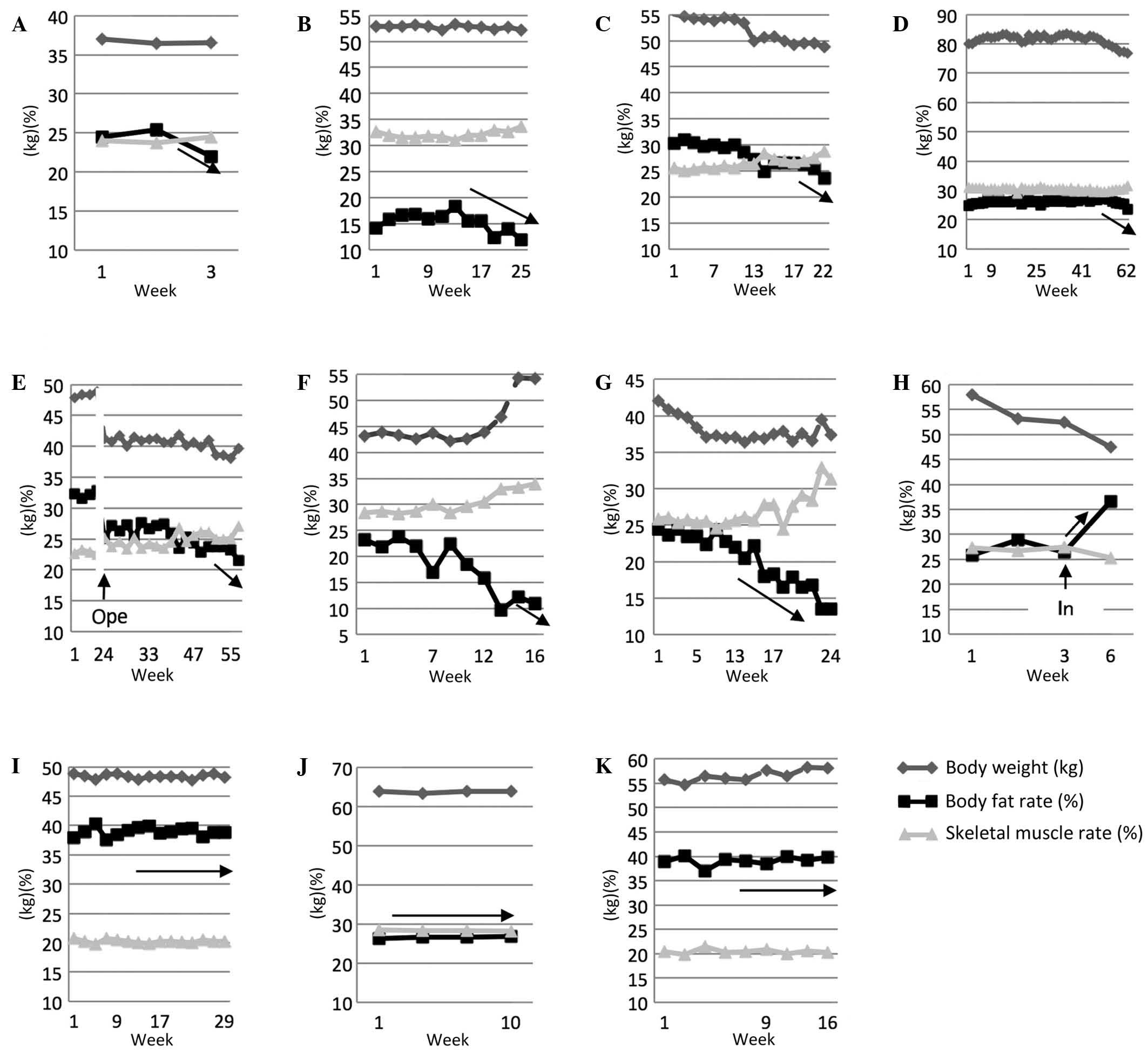 | Figure 1.Changes in body composition over time
and course of treatment. The values of the vertical axis represent
the subject's body weight, skeletal muscle rate (%), and body fat
rate (%), and the horizontal axis treatment indicates time elapsed
(weeks). Arrows indicate changes in the body fat rate. (A)
83-year-old male patient with biliary cancer; treatment was
discontinued due to severe adverse events and decreased PS. (B)
Male patient, aged 64 years, with pancreatic cancer; the patient
was receiving adjuvant chemotherapy, but treatment was discontinued
due to PD (lymph node metastasis). (C) Female patient, aged 72
years, with pancreatic cancer who received preoperative
chemotherapy; the patient underwent exploratory laparotomy and
continued to receive chemotherapy, but treatment was discontinued
due to PD (locally advanced disease). (D) 60-year-old male patient
with biliary cancer; the patient received GEM 46 times, but the
treatment was discontinued due to PD (locally advanced disease).
(E) Female patient, aged 74 years, with pancreatic cancer who
underwent preoperative chemotherapy followed by
pancreaticoduodenectomy (Ope); the patient received adjuvant
chemotherapy postoperatively, but the treatment was discontinued
due to PD (peritonitis and ascites retention). (F) Male patient,
aged 68 years, with biliary cancer; treatment was discontinued due
to PD (peritonitis and ascites retention). (G) 70-year-old female
patient with pancreatic cancer; treatment was discontinued due to
PD (peritonitis and ascites retention). (H) Male patient, aged 64
years, with pancreatic cancer who exhibited onset of jaundice
during the treatment and underwent placement of a drainage stent
(In); after the jaundice reduced, the patient's PS improved and the
continuation of treatment became possible. (I) 67-year-old female
patient with pancreatic cancer; the patient underwent postoperative
chemotherapy, and the treatment was completed following
confirmation of the disappearance of the remaining lesion. (J)
Female patient, aged 60 years, with urothelial carcinoma; treatment
was discontinued due to PD (brain metastasis). (K) 64-year-old male
patient with urothelial carcinoma; treatment was discontinued due
to PD (bone and lung metastases) and a decreased PS. PS,
performance status; PD, progressive disease. |
Association between body composition
and adverse events
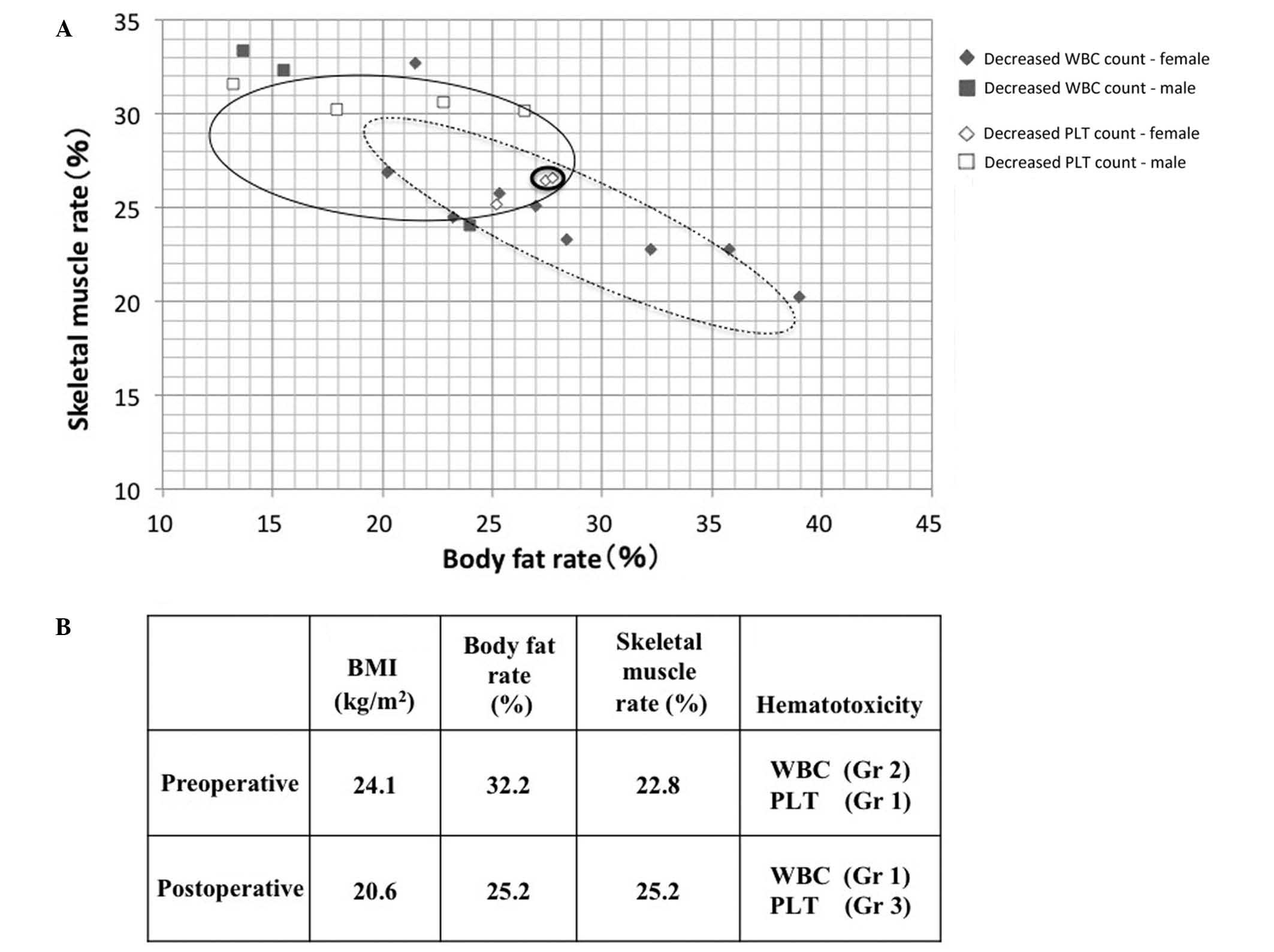
The association between grade ≥2 hematotoxicity
(CTCAE version 4.03) and body composition was examined in patients
with pancreatobiliary tract cancer (Fig.
3). With regard to body composition, the mean body fat and
skeletal muscle rates were 25.8 and 26.2%, respectively, in the 14
patients (including 10 female patients) with a decreased white
blood cell (WBC) count (<3000/mm3; Fig. 3A, dotted line); the corresponding
rates were 23.3 and 28.7%, respectively, in the 7 patients
(including 2 female patients) with a decreased platelet count
(<75,000/mm3; Fig. 3A,
gray line); and 27.5 and 26.5%, respectively, in 2 patients
(including 1 female patient) who had both decreased WBC and
platelet counts (Fig. 3A, bold line).
Therefore, a decreased WBC count was more common in female patients
with a relatively high body fat rate, whereas a decreased platelet
count was more common in male patients with a high skeletal muscle
rate. Notably, the patient receiving chemotherapy preoperatively
and postoperatively exhibited a body weight reduction of ≥5 kg
relative to the preoperative weight, which was associated with a
marked decrease in the body fat rate from 32.2 to 25.2%, as well as
a change in the hematotoxicity profile from a decreased WBC count
to a decreased platelet count (Figs. 1E
and 3B).
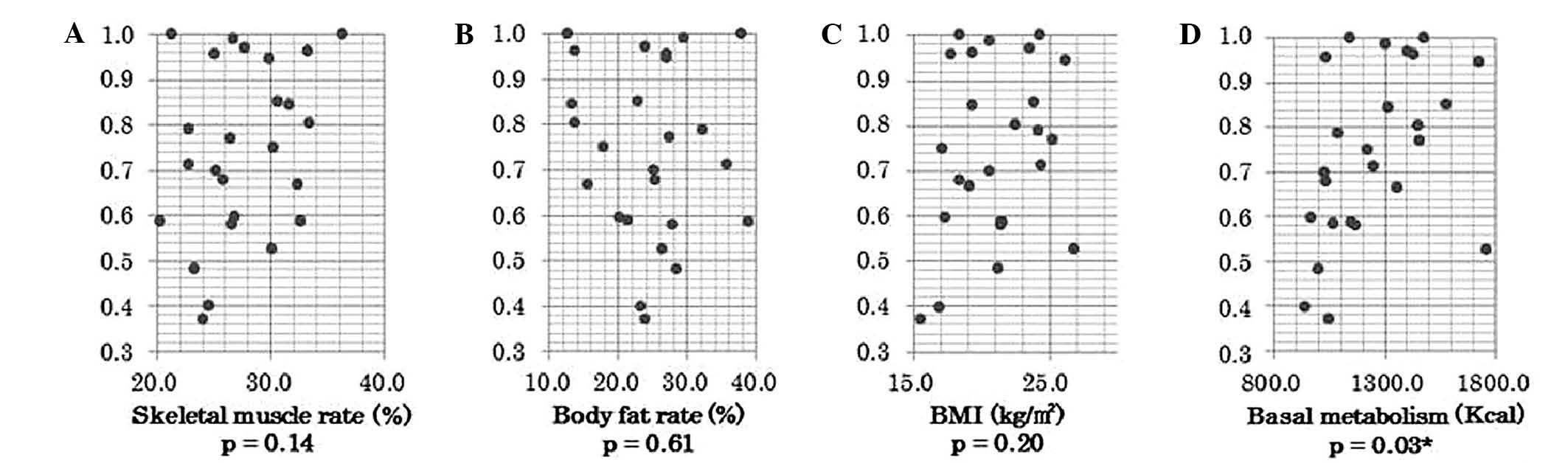
Correlation between body composition
and RDI
The association between body composition parameters
and the RDI of GEM administration in patients with pancreatobiliary
tract cancer was examined. No correlation was identified between
RDI and BMI, body fat rate or skeletal muscle rate; however, RDI
was found to correlate with basal metabolic rate, with RDI values
increasing as the basal metabolic rate increased (P=0.029; Fig. 4).
Discussion
Protein and fat are generally broken down in the
host as cancers enlarge and progress; at the same time, cytokines
and other molecules are released from cancer cells causing
cachexia, which results in marked reductions in muscle mass and fat
(32–36). When sarcopenia develops along with the
progression of cancer lesions, muscle mass decreases first,
progressing further into cachexia and accompanied by a decrease in
body weight and fat (37–39). However, the present study revealed
that the progression of pathological conditions is reflected by
decreased body fat in patients with pancreatobiliary tract cancer
being treated with GEM-based chemotherapy. As the bile duct and
pancreas are deeply involved in the absorption and digestion of
fat, we believe that the disintegration of fat associated with
cancer progression is observed as a decrease in body fat prior to
the development of sarcopenia, accompanied by reduced muscle mass
(40). This is consistent with the
present findings, as patients intubated with a biliary stent due to
the onset of jaundice (Fig. 1H)
exhibited an increase in body fat rate following the reduction of
the jaundice, allowing them to continue the treatment. By contrast,
the urinary tract is a retroperitoneal organ with little effect on
digestion and absorption, thus causing little change in body
composition (41). Therefore, in the
case of patients with urothelial carcinoma who were similarly
treated with GEM-based chemotherapy, no associations were
identified between body fat rates and the progression of
pathological conditions or the possibility of continuing
chemotherapy (Figs. 1J, 1K and
2). In addition, it is notable that,
in the patients with pancreatobiliary tract cancer who had ascites
retention (Fig. 1F and G), BMI and
skeletal muscle mass, estimated using the Omron body composition
monitor, increased along with body weight, and only the amount of
body fat decreased. It appears that the calculation-based increase
in skeletal muscle mass resulted from the principle of the BI
method: Fat does not conduct electricity, whereas muscles and
moisture do conduct electricity (18). Body weight gain resulting from edema
and ascitic fluid makes it very difficult to determine the proper
dose of anticancer drugs. Therefore, as the present findings
indicate, the measurement of changes in body composition over time
with the characteristics of the BI method in consideration may be a
useful adjunct index to easily determine pathological
conditions.
With regard to the differences in hematotoxicity
profile by body composition in patients with pancreatobiliary tract
cancer, the current findings indicate that a decreased WBC count
was more common in women with a high body fat rate. Similarly,
Miura et al (42) have
reported that a decreased neutrophil count induced by GEM
administration was more common in women. In addition, among the
body composition changes associated with surgery in one patient
from the present study (Fig. 1E), a
marked postoperative reduction in body fat rate resulted in a
decreased platelet count (Fig. 3B),
suggesting that the hematotoxicity profile may differ according to
changes in body composition, as well as to gender. Therefore, it
will be necessary to study the association between body composition
and changes in the hematotoxicity profile by examining more
diseases and regimens (43–45).
Among all body composition parameters investigated
in the present study, the RDI associated with GEM administration
was found to be positively correlated only with basal metabolism
(Fig. 4). Basal metabolism is the
basic amount of metabolism required for life maintenance, and the
value changes according to the age, height, weight, gender and
physical activity levels of individuals (46,47). In
this current study, basal metabolism was calculated using our own
data and data from the Omron Corporation, which is based on the
dietary reference intakes for the Japanese population (31). Approximately 30% of basal metabolism
occurs in the skeletal muscles. In body composition, fat is
classified into subcutaneous and visceral fat; the former is needed
to maintain energy and body temperature, and the latter is
considered to be associated with lifestyle-related diseases such as
dyslipidemia and diabetes (48,49).
Muscles consist of skeletal muscles, smooth muscles and cardiac
muscles, and only skeletal muscles may be increased through
exercise. When the skeletal muscle mass decreases, less energy is
consumed, resulting in a reduced basal metabolism (19–22,37). The
present findings demonstrated that, in patients with
pancreatobiliary cancer, there is little change in the skeletal
muscle rate compared to the body fat rate. As the basal metabolism
was affected by factors such as age and gender differences, an
association with RDI was observed. This is not contradictory to the
study by Prado et al (43),
which reported that doses of 5-fluorouracil correlated with body
weight, excluding body fat, in patients with colorectal cancer.
The BI method is easy and safe, and is able to
easily measure and monitor changes in a patient's body composition
at each visit for chemotherapy. In addition, this method has been
reported to correlate extremely well with the evaluation of body
composition by computed tomography, magnetic resonance imaging and
dual energy X-ray absorptiometry (15,20–22,50,51).
The current findings indicate that regularly assessing the body
composition, using the BI method, of patients with pancreatobiliary
tract cancer receiving GEM-based chemotherapy is a useful adjunct
index for understanding pathological conditions and for predicting
the continuation of chemotherapy treatment.
In conclusion, measurement of body composition in
patients with pancreatobiliary tract cancer over time may be a
helpful adjunct index to understand pathological conditions and
changes in physical conditions.
Glossary
Abbreviations
Abbreviations:
|
BI
|
bioelectrical impedance
|
|
BMI
|
body mass index
|
|
GEM
|
gemcitabine
|
|
PS
|
performance status
|
|
PD
|
progressive disease
|
|
RDI
|
relative dose intensity
|
References
|
1
|
Burris HA III, Moore MJ, Andersen J, Green
MR, Rothenberg ML, Modiano MR, Cripps MC, Portenoy RK, Storniolo
AM, Tarassoff P, et al: Improvements in survival and clinical
benefit with gemcitabine as first-line therapy for patients with
advanced pancreas cancer: A randomized trial. J Clin Oncol.
15:2403–2413. 1997.PubMed/NCBI
|
|
2
|
Moore MJ, Goldstein D, Hamm J, Figer A,
Hecht JR, Gallinger S, Au HJ, Murawa P, Walde D, Wolff RA, et al:
National Cancer Institute of Canada Clinical Trials Group:
Erlotinib plus gemcitabine compared with gemcitabine alone in
patients with advanced pancreatic cancer: A phase III trial of the
National Cancer Institute of Canada Clinical Trials Group. J Clin
Oncol. 25:1960–1966. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Valle J, Wasan H, Palmer DH, Cunningham D,
Anthoney A, Maraveyas A, Madhusudan S, Iveson T, Hughes S, Pereira
SP, et al: ABC-02 Trial Investigators: Cisplatin plus gemcitabine
versus gemcitabine for biliary tract cancer. N Engl J Med.
362:1273–1281. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Conroy T, Desseigne F, Ychou M, Bouché O,
Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de
la Fouchardière C, et al: Groupe Tumeurs Digestives of Unicancer;
PRODIGE Intergroup: FOLFIRINOX versus gemcitabine for metastatic
pancreatic cancer. N Engl J Med. 364:1817–1825. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
von der Maase H, Sengelov L, Roberts JT,
Ricci S, Dogliotti L, Oliver T, Moore MJ, Zimmermann A and Arning
M: Long-term survival results of a randomized trial comparing
gemcitabine plus cisplatin, with methotrexate, vinblastine,
doxorubicin, plus cisplatin in patients with bladder cancer. J Clin
Oncol. 23:4602–4608. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sultana A, Smith CT, Cunningham D,
Starling N, Neoptolemos JP and Ghaneh P: Meta-analyses of
chemotherapy for locally advanced and metastatic pancreatic cancer.
J Clin Oncol. 25:2607–2615. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Okusaka T, Ishii H, Funakoshi A, Yamao K,
Ohkawa S, Saito S, Saito H and Tsuyuguchi T: Phase II study of
single-agent gemcitabine in patients with advanced biliary tract
cancer. Cancer Chemother Pharmacol. 57:647–653. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ozawa A, Tanji N, Ochi T, Yanagihara Y,
Kikugawa T, Yamaguchi A, Ikeda T, Shimamoto K, Aoki K, Toshino A
and Yokoyama M: Gemcitabine and cisplatin for advanced urothelial
carcinomas: The Ehime University Hospital experience. Int J Clin
Oncol. 12:279–283. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Janssen I, Heymsfield SB and Ross R: Low
relative skeletal muscle mass (sarcopenia) in older persons is
associated with functional impairment and physical disability. J Am
Geriatr Soc. 50:889–896. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mitsiopoulos N, Baumgartner RN, Heymsfield
SB, Lyons W, Gallagher D and Ross R: Cadaver validation of skeletal
muscle measurement by magnetic resonance imaging and computerized
tomography. J Appl Physiol (1985). 85:115–122. 1998.PubMed/NCBI
|
|
11
|
Ferland M, Després JP, Tremblay A, Pinault
S, Nadeau A, Moorjani S, Lupien PJ, Thériault G and Bouchard C:
Assessment of adipose tissue distribution by computed axial
tomography in obese women: Association with body density and
anthropometric measurements. Br J Nutr. 61:139–148. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kuk JL, Lee S, Heymsfield SB and Ross R:
Waist circumference and abdominal adipose tissue distribution:
Influence of age and sex. Am J Clin Nutr. 81:1330–1334.
2005.PubMed/NCBI
|
|
13
|
Nuñez C, Gallagher D, Grammes J,
Baumgartner RN, Ross R, Wang Z, Thornton J and Heymsfield SB:
Bioimpedance analysis: Potential for measuring lower limb skeletal
muscle mass. JPEN J Parenter Enteral Nutr. 23:96–103. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pietrobelli A, Morini P, Battistini N,
Chiumello G, Nuñez C and Heymsfield SB: Appendicular skeletal
muscle mass: Prediction from multiple frequency segmental
bioimpedance analysis. Eur J Clin Nutr. 52:507–511. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Janssen I, Heymsfield SB, Baumgartner RN
and Ross R: Estimation of skeletal muscle mass by bioelectrical
impedance analysis. J Appl Physiol (1985). 89:465–471.
2000.PubMed/NCBI
|
|
16
|
Schwan HP and Kay CF: The conductivity of
living tissues. Ann NY Acad Sci. 65:1007–1013. 1957. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Houtkooper LB, Lohman TG, Going SB and
Howell WH: Why bioelectrical impedance analysis should be used for
estimating adiposity. Am J Clin Nutr. 64(Suppl 3): 436S–448S.
1996.PubMed/NCBI
|
|
19
|
Oshima Y, Shiga T, Namba H and Kuno S:
Estimation of whole-body skeletal muscle mass by bioelectrical
impedance analysis in the standing position. Obes Res Clin Pract.
4:e1–e82. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Oshima Y and Shiga T: Within-day
variability of whole-body and segmental bioelectrical impedance in
a standing position. Eur J Clin Nutr. 60:938–941. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ishiguro N, Kanehisa H, Miyatani M, Masuo
Y and Fukunaga T: A comparison of three bioelectrical impedance
analyses for predicting lean body mass in a population with a large
difference in muscularity. Eur J Appl Physiol. 94:25–35. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tanaka NI, Miyatani M, Masuo Y, Fukunaga T
and Kanehisa H: Applicability of a segmental bioelectrical
impedance analysis for predicting the whole body skeletal muscle
volume. J Appl Physiol. 103:1688–1695. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kushner RF, Kunigk A, Alspaugh M, Andronis
PT, Leitch CA and Schoeller DA: Validation of
bioelectrical-impedance analysis as a measurement of change in body
composition in obesity. Am J Clin Nutr. 52:219–223. 1990.PubMed/NCBI
|
|
24
|
Deurenberg P, Tagliabue A and Schouten FJ:
Multi-frequency impedance for the prediction of extracellular water
and total body water. Br J Nutr. 73:349–358. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Stall SH, Ginsberg NS, DeVita MV,
Zabetakis PM, Lynn RI, Gleim GW, Wang J, Pierson RN Jr and Michelis
MF: Comparison of five body-composition methods in peritoneal
dialysis patients. Am J Clin Nutr. 64:125–130. 1996.PubMed/NCBI
|
|
26
|
Gallagher D, Belmonte D, Deurenberg P,
Wang Z, Krasnow N, Pi-Sunyer FX and Heymsfield SB: Organ-tissue
mass measurement allows modeling of REE and metabolically active
tissue mass. Am J Physiol. 275:E249–E258. 1998.PubMed/NCBI
|
|
27
|
Bosy-Westphal A, Later W, Hitze B, Sato T,
Kossel E, Gluer CC, Heller M and Muller MJ: Accuracy of
bioelectrical impedance consumer devices for measurement of body
composition in comparison to whole body magnetic resonance imaging
and dual X-ray absorptiometry. Obes Facts. 1:319–324. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kataoka H: A new monitoring method for the
estimation of body fluid status by digital weight scale
incorporating bioelectrical impedance analyzer in definite heart
failure patients. J Card Fail. 15:410–418. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nakajima H, Koizumi K, Tanaka T, Ishigaki
Y, Yoshitake Y, Yonekura H, Sakuma T, Fukushima T, Umehara H, Ueno
S, et al: Loss of HITS (FAM107B) expression in cancers of multiple
organs: Tissue microarray analysis. Int J Oncol. 41:1347–1357.
2012.PubMed/NCBI
|
|
31
|
Ministry of Health. Labour and Welfare:
Health Japan 21 - National Health and Nutrition Survery. http://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/kenkou/kenkounippon21/en/eiyouchousa/
|
|
32
|
Fearon K, Arends J and Baracos V:
Understanding the mechanisms and treatment options in cancer
cachexia. Nat Rev Clin Oncol. 10:90–99. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nelson KA, Walsh D and Sheehan FA: The
cancer anorexia-cachexia syndrome. J Clin Oncol. 12:213–225.
1994.PubMed/NCBI
|
|
34
|
Puccio M and Nathanson L: The cancer
cachexia syndrome. Semin Oncol. 24:277–287. 1997.PubMed/NCBI
|
|
35
|
Parry-Billings M, Leighton B, Dimitriadis
GD, Curi R, Bond J, Bevan S, Colquhoun A and Newsholme EA: The
effect of tumour bearing on skeletal muscle glutamine metabolism.
Int J Biochem. 23:933–937. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Cruz-Jentoft AJ, Baeyens JP, Bauer JM,
Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y,
Schneider SM, et al: Sarcopenia: European consensus on definition
and diagnosis: Report of the European working group on Sarcopenia
in older people. Age Ageing. 39:412–423. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Gordon JN, Green SR and Goggin PM: Cancer
cachexia. QJM. 98:779–788. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Scott HR, McMillan DC, Forrest LM, Brown
DJ, McArdle CS and Milroy R: The systemic inflammatory response,
weight loss, performance status and survival in patients with
inoperable non-small cell lung cancer. Br J Cancer. 87:264–267.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
George J, Cannon T, Lai V, Richey L,
Zanation A, Hayes DN, Shores C, Guttridge D and Couch M: Cancer
cachexia syndrome in head and neck cancer patients: Part II.
Pathophysiology. Head Neck. 29:497–507. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Das SK, Eder S, Schauer S, Diwoky C,
Temmel H, Guertl B, Gorkiewicz G, Tamilarasan KP, Kumari P, Trauner
M, et al: Adipose triglyceride lipase contributes to
cancer-associated cachexia. Science. 333:233–238. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Pelucchi C, Bosetti C, Negri E, Malvezzi M
and La Vecchia C: Mechanisms of disease: The epidemiology of
bladder cancer. Nat Clin Pract Urol. 3:327–340. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Miura A, Onoue M, Terada K, Takahashi K
and Inui K: Gender differences in hematotoxicity induced by
gemcitabine monotherapy. Jpn J Pharm Health Care Sci. 36:57–60.
2010. View Article : Google Scholar
|
|
43
|
Prado CM, Baracos VE, McCargar LJ,
Mourtzakis M, Mulder KE, Reiman T, Butts CA, Scarfe AG and Sawyer
MB: Body composition as an independent determinant of
5-fluorouracil-based chemotherapy toxicity. Clin Cancer Res.
13:3264–3268. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Prado CM, Baracos VE, McCargar LJ, Reiman
T, Mourtzakis M, Tonkin K, Mackey JR, Koski S, Pituskin E and
Sawyer MB: Sarcopenia as a determinant of chemotherapy toxicity and
time to tumor progression in metastatic breast cancer patients
receiving capecitabine treatment. Clin Cancer Res. 15:2920–2926.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Gusella M, Toso S, Ferrazzi E, Ferrari M
and Padrini R: Relationships between body composition parameters
and fluorouracil pharmacokinetics. Br J Clin Pharmacol. 54:131–139.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ganpule AA, Tanaka S, Ishikawa-Takata K
and Tabata I: Interindividual variability in sleeping metabolic
rate in Japanese subjects. Eur J Clin Nutr. 61:1256–1261. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Usui C, Takahashi E, Gando Y, Sanada K,
Oka J, Miyachi M, Tabata I and Higuchi M: Relationship between
blood adipocytokines and resting energy expenditure in young and
elderly women. J Nutr Sci Vitaminol (Tokyo). 53:529–535. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Wu J, Boström P, Sparks LM, Ye L, Choi JH,
Giang AH, Khandekar M, Virtanen KA, Nuutila P, Schaart G, et al:
Beige adipocytes are a distinct type of thermogenic fat cell in
mouse and human. Cell. 150:366–376. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Cohen P, Levy JD, Zhang Y, Frontini A,
Kolodin DP, Svensson KJ, Lo JC, Zeng X, Ye L, Khandekar MJ, et al:
Ablation of PRDM16 and beige adipose causes metabolic dysfunction
and a subcutaneous to visceral fat switch. Cell. 156:304–316. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Ellegård LH, Ahlén M, Körner U, Lundholm
KG, Plank LD and Bosaeus IG: Bioelectric impedance spectroscopy
underestimates fat-free mass compared to dual energy X-ray
absorptiometry in incurable cancer patients. Eur J Clin Nutr.
63:794–801. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Yamakage H, Ito R, Tochiya M, Muranaka K,
Tanaka M, Matsuo Y, Odori S, Kono S, Shimatsu A and Satoh-Asahara
N: The utility of dual bioelectrical impedance analysis in
detecting intra-abdominal fat area in obese patients during weight
reduction therapy in comparison with waist circumference and
abdominal CT. Endocr J. 61:807–819. 2014. View Article : Google Scholar : PubMed/NCBI
|