Introduction
Verrucous carcinoma (VC) is a variant of
well-differentiated squamous cell carcinoma and is considered to be
associated with human papilloma virus (HPV) infection. The majority
of VCs occur in the oral cavity, genital area or plantar surface.
VCs are rarely detected in the head and neck region; however, in
such instances they predominantly occur in the mucosa of the
respiratory or digestive tracts (1,2).
Additional locations in the head and neck region include the
larynx, nasopharynx, paranasal sinuses and esophagus. Furthermore,
dermal lesions are rarely observed (1); cutaneous VCs of the head and neck region
predominantly occur on the scalp (3),
and cervical epidermal lesions are rare (4). While the incidence of VC is 5–24% of all
penile cancers and 2–12% of all oral carcinomas, dermal VC of sites
other than the inguinal region and legs has been reported simply as
rare or uncommon, without an accurate incidence rate (1,2). Surgical
resection is the preferred treatment strategy for patients with VC,
however, anal and perianal lesions have a high recurrence rate of
~70%, and a mortality rate of 20–30%. Although radiation therapy is
not considered to be as effective as surgery, its efficacy as an
adjuvant treatment strategy remains a topic of debate (4,5). The
present case report describes a rare case of papillary-type
cutaneous VC of the neck, including the immunohistochemical
findings, which have not previously been well described.
Additionally, the current study includes discussion of the diseases
that VC should be differentiated from.
Case report
Clinical presentation
An 80-year-old man was referred as an outpatient to
Osaka Medical College Hospital (Takatsuki, Japan) in November 2011
exhibiting a cutaneous tumor at the anterior of the neck (Fig. 1). The tumor was observed as a
flesh-colored multinodular protrusion measuring 1.7 cm in diameter.
The patient reported that the lesion had gradually grown in size;
however, precise details of its development were unclear. The
patient had undergone a colonoscopic polypectomy 14 years prior to
referral and, 2 years ago, experienced an angina attack. Following
a clinical diagnosis of fibroma (November 2011), the lesion was
excised with a margin of the intact skin on April 5, 2012.
Recurrence was not observed in the 3 years following the resection
of the tumor. Written informed consent was obtained from the
patient.
Histopathological analysis
The surgical specimen was fixed in 10% buffered
formalin, processed and embedded in paraffin. Paraffin sections
were cut to a thickness of 4 µm, and stained with hematoxylin and
eosin. Immunohistochemical staining was also performed with
antibodies for Ki-67, p53, cytokeratin (CK)7, 8, 10, 13, 18 and 20,
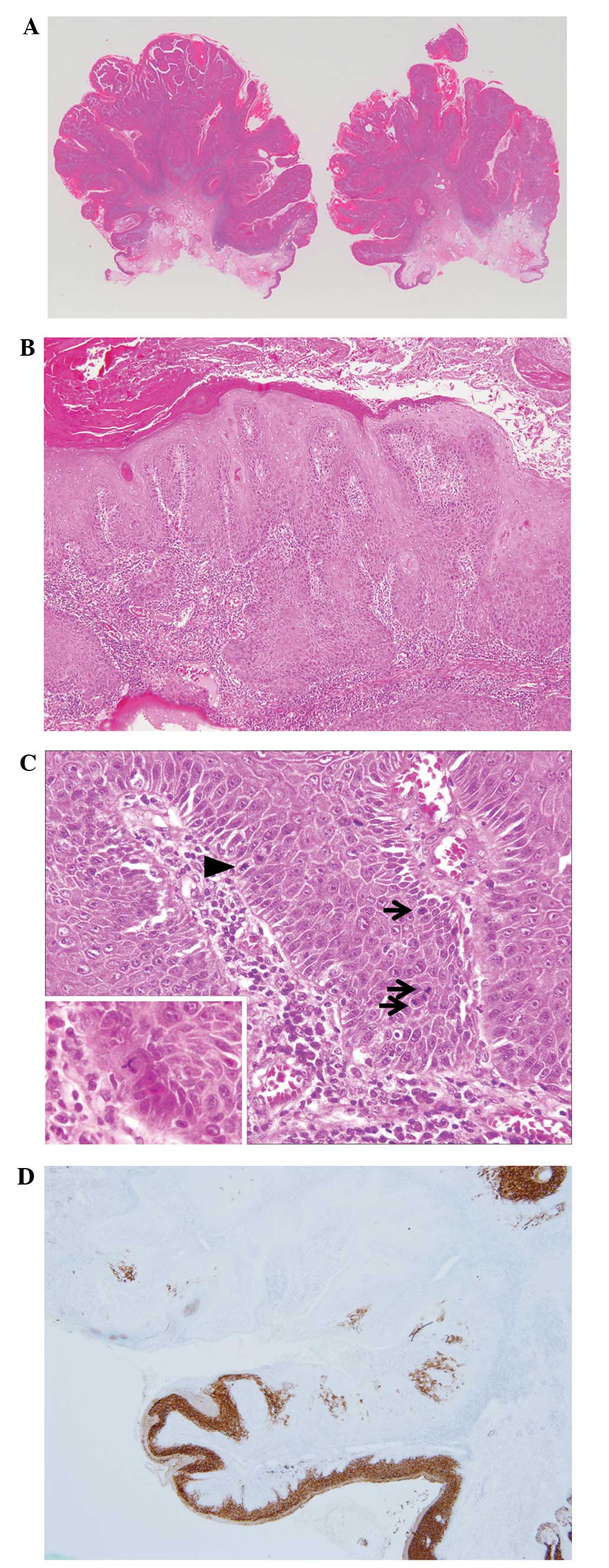
and HPV, using the avidin-biotin-peroxidase complex technique. The
thickened epidermis had proliferated in a papillary pattern
(Fig. 2A) and exhibited swelling rete
ridges indicating downgrowth. Cellular atypia was low in the
majority of keratinocytes (Fig. 2B).
The basilar nuclei were plump and, in general, the nuclei contained
a single enlarged nucleolus. Mitoses were easily identified and
abnormal karyokinesis was observed in a small number of cells
(Fig. 2C). Clusters of cancer cells
invading into the subepidermal layer were surrounded by a large
number of lymphocytes and a small number of lymph follicles had
formed. Cellular atypia of the invasive nests was greater than that
of intraepidermal cells. Furthermore, immunohistochemical analysis
of Ki-67 and p53 did not reveal any differences in the expression
of these proteins in the lesion compared with the surrounding
healthy epidermis. Additional immunostaining revealed a positive
signal for CK10 in all layers, excluding the basal layer of the
healthy epidermis. By contrast, CK10-positive staining was observed
in the upper half of the intraepidermal carcinoma, but was not
expressed in the deeper layer. CK10 expression was not observed in
any of the epidermal layers of the lesion (Fig. 2D). Furthermore, the neoplastic and
surrounding non-neoplastic epidermis were identified to be
immunonegative for CK7, 8, 13, 18 and 20, and HPV immunostaining
was negative. The aforementioned histopathological and
immunohistochemical findings were used to determine a diagnosis of
VC and dismiss the previous clinical diagnosis of fibroma.
Discussion
VC is a low-grade variant of squamous cell
carcinoma. The majority of VCs in the head and neck region occur in
the oral cavity, rarely arising in the respiratory or digestive
tracts of the neck (1,2). VC presenting on the buccal and gingival
mucosa is known as florid papillomatosis, while VC located on the
plantar surface is referred to as carcinoma cuniculatum (3). Cutaneous VC of the head and neck
predominantly occurs on the scalp, however, cutaneous VC of the
neck is rare. Macroscopically, VC typically forms a flat or
exophytic elevation, the surface of which exhibits aggregation of
small nodules (6). However, due to
papillary growth of the epidermis, the present lesion formed a
multinodular semi-pedunculated protrusion. VC histology is commonly
characterized by a wart-like appearance with hyperkeratosis and/or
hyperparakeratosis, and minimal cell atypia (2). In addition, VC typically grows in an
expansive manner towards surrounding tissue, with a
well-circumscribed margin. Infiltrating irregular nests, observed
in normal squamous cell carcinoma, are not present in VC. A case of
pedunculated VC previously reported by Shimizu et al
exhibited similarities to the present lesion (7). However, the current study emphasizes the
histological papillary growth pattern of the VC, as the epidermal
growth pattern determines the macroscopic form of the lesion.
It is necessary to differentiate VCs from lesions
that grow in the same pattern. In particular, the present lesion
should be clinically and histologically differentiated from
papillary squamous cell carcinoma and a number of other benign
lesions, including seborrheic keratosis, fibroepithelial polyp,
verruca vulgaris and pseudocarcinomatous hyperplasia. As with VC,
papillary squamous cell carcinoma is a rare variant of squamous
cell carcinoma (8). The present VC
lesion proliferated in the same pattern as papillary squamous cell
carcinoma, but did not share its characteristic nuclear atypia and
pleomorphism (9). Condylomatous
carcinoma also demonstrates high-grade cytological atypia (6). Although it was previously unclear
whether Buschke-Löwenstein tumor (BLT) should be classified as
non-neoplastic giant condyloma or as a type of VC, a recent study
recognized BLT as VC localized in the anogenital region (10). The histological attributes of BLT are
similar to those of the present lesion (11). Thus, condyloma acuminatum should also
be differentiated from VC. Pseudocarcinomatous hyperplasia is
caused by a proliferation of epithelial cells in response to
infection, neoplasia, inflammation or trauma, and may resemble
well-differentiated squamous cell carcinoma by exhibiting
pseudoinvasion (12). However, the
presence of nuclear atypia, individual necrotic keratinocytes and
numerous mitoses favored the diagnosis of the present lesion as
squamous cell carcinoma over pseudocarcinomatous hyperplasia
(12).
Immunostaining for CK10 revealed reduced CK10
protein expression in the present lesion. CK10 has previously been
described as a valuable tool in the diagnosis of oral squamous cell
carcinoma and clonal seborrheic keratosis (13,14).
Therefore, immunostaining for CK10 may aid in the diagnosis of
cutaneous VC. However, the hypothesis that numerous
immunohistochemical analyses are useful in the diagnosis of
papillary-type cutaneous VC was confuted by the current study.
CK13, 8 and 18 are reported to be useful markers in the diagnosis
of squamous cell carcinoma in the head and neck region (13,15), and
CK8 and 18 appear to be associated with the invasion and metastasis
of squamous cell carcinoma (16).
However, these CKs stained negatively in the neoplastic and
surrounding healthy epidermal tissue of the present lesion, and,
therefore, were not useful in the differential diagnosis of the
present case. Furthermore, an increase in Ki-67 labeling and
positivity for p53 were not observed in the present case. In
agreement with this finding, immunohistochemistry for Ki-67 and p53
expression in VC is reported to be more similar to that of healthy
epidermis than that of squamous cell carcinoma (17).
Immunostaining for HPV did not reveal positivity in
the present case. However, HPV 16 and 18 have been detected in
laryngeal VC, and HPV 6 and 11 infections appear to be associated
with oral VC (2,17). Additionally, ano-urogenital VCs are
closely associated with these viruses (18). There appears to be no association
between HPV infection and rare cutaneous VC occurring at sites
other than oral, ano-urogenital and palmoplantar regions (3). However, a previous study did identify an
association between HPV infection and cutaneous VCs (19). HPV-induced carcinogenesis and
progression of VC may involve amino acid changes caused by
mutations in an HPV oncogene, leading to the degradation of a p53
tumor suppressor gene (17). However,
the present case demonstrated no abnormal immunostaining for p53.
To date, the presence of HPV has yet to effect the therapeutic
strategies used for VC.
In conclusion, the current study reports a rare case
of papillary-type cutaneous VC arising in the neck, an uncommon
location for this tumor type. Unlike VC lesions that occur at more
common sites of VC development, HPV infection was not identified in
the present case. Furthermore, CK10 exhibited a weak staining
pattern compared with the surrounding intact epidermis.
References
|
1
|
Rinker MH, Fenske NA, Scalf LA and Glass
LF: Histologic variants of squamous cell carcinoma of the skin.
Cancer Control. 8:355–363. 2001.
|
|
2
|
Schwartz RA: Verrucous carcinoma of the
skin and mucosa. J Am Acad Dermatol. 32:1–21. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Assaf C, Steinhoff M, Petrov I, et al:
Verrucous carcinoma of the axilla: Case report and review. J Cutan
Pathol. 31:199–204. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Miller ME, Martin N, Julliard GF, Bhuta S
and Ishiyama A: Temporal bone verrucous carcinoma: Outcomes and
treatment controversy. Eur Arch Otorhinolaryngol. 267:1927–1931.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Indinnimeo M, Impagnatiello A, D'Ettorre
G, et al: Buschke-Löwenstein tumor with squamous cell carcinoma
treated with chemo-radiation therapy and local surgical excision:
Report of three cases. World J Surg Oncol. 11:2312013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cassarino DS, Derienzo DP and Barr RJ:
Cutaneous squamous cell carcinoma: A comprehensive
clinicopathologic classification. Part one. J Cutan Pathol.
33:191–206. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shimizu A, Tamura A, Tanaka S, et al:
Pedunculated verrucous carcinoma of the thigh. Eur J Dermatol.
15:393–395. 2005.PubMed/NCBI
|
|
8
|
Landman G, Taylor RM and Friedman KJ:
Cutaneous papillary squamous cell carcinoma. A report of two cases.
J Cutan Pathol. 17:105–110. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Azorín D, Rodríguez-Peralto JL,
García-García E and Salamanca J: Cutaneous papillary squamous cell
carcinoma. Report of three new cases and review of the literature.
Virchows Arch. 442:298–301. 2003.PubMed/NCBI
|
|
10
|
Asato Y, Taira K, Yamamoto Y and Uezato H:
Detection of human papillomavirus type 11 in a case of
Buschke-Löwenstein tumor. Eur J Dermatol. 18:329–331.
2008.PubMed/NCBI
|
|
11
|
Hicheri J, Jaber K, Dhaoui MR, et al:
Giant condyloma (Buschke-Löwenstein tumor). A case report. Acta
Dermatovenerol Alp Pannonica Adriat. 15:181–183. 2006.PubMed/NCBI
|
|
12
|
El-Khoury J, Kibbi AG and Abbas O:
Mucocutaneous pseudoepitheliomatous hyperplasia: A review. Am J
Dermatopathol. 34:165–175. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fillies T, Jogschies M, Kleinheinz J, et
al: Cytokeratin alteration in oral leukoplakia and oral squamous
cell carcinoma. Oncol Rep. 18:639–643. 2007.PubMed/NCBI
|
|
14
|
Böer-Auer A, Jones M and Lyasnichaya OV:
Cytokeratin 10-negative nested pattern enables sure distinction of
clonal seborrheic keratosis from pagetoid Bowen's disease. J Cutan
Pathol. 39:225–233. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Okada Y and Moride M: Immunohistochemical
study of differential expressions of cytokeratin-13, −14, −17 and
p53 in epithelial dysplasia and carcinoma of the tongue. J Hard
Tissue Biol. 19:123–130. 2010. View Article : Google Scholar
|
|
16
|
Yamashiro Y, Takei K, Umikawa M, et al:
Ectopic coexpression of keratin 8 and 18 promotes invasion of
transformed keratinocytes and is induced in patients with cutaneous
squamous cell carcinoma. Biochem Biophys Res Commun. 399:365–372.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dubina M and Goldenberg G:
Viral-associated nonmelanoma skin cancers: A review. Am J
Dermatopathol. 31:561–573. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Petter G and Haustein UF: Histologic
subtyping and malignancy assessment of cutaneous squamous cell
carcinoma. Dermatol Surg. 26:521–530. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Murao K, Kubo Y, Fukumoto D, et al:
Verrucous carcinoma of the scalp associated with human
papillomavirus type 33. Dermatol Surg. 31:1363–1365. 2005.
View Article : Google Scholar : PubMed/NCBI
|