Introduction
Endometriosis is a chronic gynecological disease
that has been widely investigated, due to its high prevalence and
substantial complications. It is estimated to affect almost 10% of
women of reproductive age and up to 25–40% of infertile women
(1,2).
Although dysmenorrhea, pelvic pain and infertility constitute the
classic triad of symptoms used in the diagnosis of endometriosis,
20-25% of patients may be asymptomatic (3). Traditionally, endometriosis is defined
as the presence of endometrial glands and stroma in ectopic sites,
other than the uterine cavity, primarily on the pelvic peritoneum,
the ovaries, the rectovaginal septum and the uterosacral ligaments.
The pathogenesis of this benign disease remains obscure, as none of
the described theories (retrograde menstruation, coelomic
metaplasia, lymphatic or vascular spread and dysfunctional immune
response) can offer a complete explanation (4,5).
Continually, various risk factors, such as familial clustering,
genetic mutations or polymorphisms and environmental toxins, have
been implicated, although without clear evidence (6,7). In
addition, special attention has been paid to the similar behavioral
pattern between endometriosis and cancer, as they both exhibit
uncontrolled, estrogen-dependent proliferation, invasion,
neo-angiogenesis and metastases (5,8). As a
matter of fact, recent studies have established a connection
between endometriosis and certain types of malignancies,
particularly ovarian cancer, breast cancer (BC), cutaneous melanoma
and non-Hodgkin's lymphoma (9,10).
Nowadays, much interest is focused on the
interconnection between endometriosis and BC, granted that the
latter forms the most frequent type of female cancer worldwide
(11,12). The latest GLOBOCAN statistics are
really impressive, as 1.67 million new cases of BC and 522,000
deaths were estimated for the year 2012 (13). However, evidence linking endometriosis
with BC is rather vague and relies on the hormonal dependence and
common risk factors of both diseases (14,15).
Scientific study is also pointed towards the interplay of BC
medication in the progress of endometriosis and vice versa. As has
been previously demonstrated, aromatase inhibitors, selective
estrogen receptor modulators and antiprogestins are novel
therapeutic agents used in the treatment of endometriosis (7,16), whereas
oral contraceptives and progestins, which are used as standard
therapies for endometriosis, may have an adverse effect on the
breast (17,18).
The aim of this study was to conduct a survey of
available published epidemiological studies indicating an
association between endometriosis and BC, and simultaneously to
categorize the results based on the strength of the association,
with the intention of the critical evaluation of the existing
data.
Data collection methods
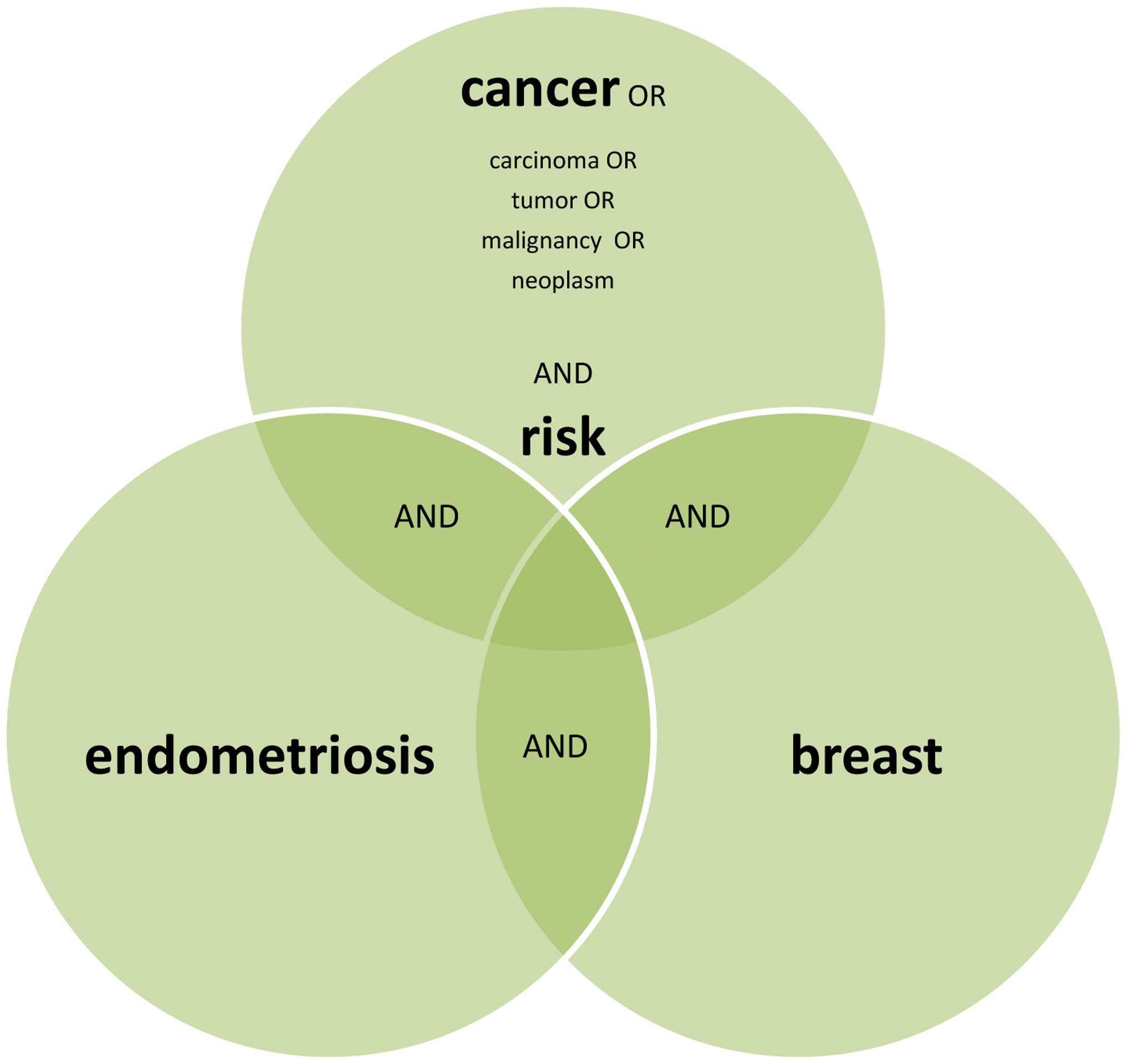
We performed a rigorous search of the PubMed/Medline
database, using the key words ‘endometriosis’ and ‘BC’ for studies
in the English language until September 2015. A supplementary
literature search was carried out using the terms ‘endometriosis’
and ‘breast’ together with ‘cancer’ or ‘malignancy’ or ‘neoplasm’
or ‘tumor’ and ‘risk’. Basic science studies (molecular, genetic
and functional), pathological studies, case reports and reviews
were all excluded from our survey (Fig.
1).
Results
Studies asserting a positive (direct)
association between endometriosis and BC
The first study examining the association between
hormonal-dependent medical disorders and BC was introduced in 1993
by Moseson et al (19). The
participants in this small case-control study were 354 cases of BC
and 747 controls, who were questioned via a telephone interview
about a series of reproductive, menstrual and gynecological
variables. Women with a reported history of endometriosis had a
substantial increased risk of BC, particularly if they belonged to
the premenopausal subgroup [odds ratio (OR), 4.3; 95% confidence
interval (CI), 0.9–20.4]. However, a fundamental study indicating a
significant correlation between endometriosis and BC was undertaken
in 1997 by Schairer et al (20). In a case-cohort study, involving
15,844 Swedish women who underwent surgery for benign gynecological
conditions, the risk of developing BC was evaluated with regard to
the indication for surgery. Following data linkage to the National
Swedish Cancer Registry, 295 cases of BC were recognized during a
follow-up period of 12.2 years. Information about the type of
surgery (oophorectomy and hysterectomy), age at surgery and the
underlying medical conditions was also available. The authors
concluded that endometriosis per se, as an exclusive indication for
surgery, was associated with a >3-fold increase in the risk of
developing BC when hysterectomy alone was performed [standardized
morbidity ratio (SMR), 3.2; 95% CI, 1.2–8.0], whilst a slight
increase was noticed when an oophorectomy was performed without a
hysterectomy (SMR, 1.7; 95% CI, 0.7–4.1). Moreover, in 1997,
Brinton et al accomplished a larger retrospective cohort
study, including 20,686 Swedish women with a hospital discharge
diagnosis of endometriosis (21).
Record linkage to cancer registers allowed the identification of
297 patients with a subsequent diagnosis of BC at a mean follow-up
of 11.4 years. The authors agreed that the total risk of developing
BC was notably affected by the history of endometriosis
[standardized incidence ratio (SIR), 1.3; 95% CI, 1.1–1.4]. The
risk of developing BC was also related to the site of origin of
endometriosis and was found to be higher among women with
endometriosis arising in the pelvis (SIR, 1.79; 95% CI,
1.2–2.6).
In 1999, Weiss et al presented a
population-based case-control study, concerning the influence of
several medical conditions on the risk of developing BC (22). The authors collected questionnaires
from 2,173 young American women, newly diagnosed with in
situ or invasive BC, and 1,990 controls. Multivariate logistic
regression analysis revealed a greater risk of developing BC among
premenopausal women with endometriosis (OR, 1.68), particularly
among those with recent surgery (OR 1–9 years, 2.38; 95% CI,
1.0–5.5). However, the risk was relatively lower among young women
who had previously undergone surgery for endometriosis (OR, 1.14;
95% CI, 0.7–1.8). At the same time, Venn et al conducted a
case-cohort study in 2,970 Australian in vitro fertilisation
(IVF) candidates, in order to assess the incidence of invasive
breast, ovarian and uterine cancer combined with the infertility
cause and administration of superovulation drugs (23). As a result, infertile women with
endometriosis were found to have a borderline increase in the risk
of developing BC, particularly 12 months following exposure to
fertility drugs and when 3–6 oocytes per ovulation cycle were
collected (SIR, 1.04; 95% CI, 0.71–1.54). In 2004, Borgfeldt and
Andolf evaluated the incidence of gynecological cancer in patients
with benign ovarian cysts, functional ovarian cysts, or
endometriosis (24). By the optimal
use of the Swedish database, they designed a nested case-control
study of 28,163 women with a hospital diagnosis of endometriosis
each matched with 3 controls. Briefly, the authors detected a
subtle increase in the risk of developing BC among women with
endometriosis (OR, 1.10; 95% CI, 1.0–1.2). Utilizing Swedish
Inpatient and Cancer records once again, in 2006, Melin et
al conducted a larger retrospective cohort study for the
purpose of examining cancer risk, particularly ovarian cancer risk,
among women with endometriosis (25).
Therefore, 64,492 women discharged from the hospital and coded for
endometriosis as first time diagnosis, entered the study.
Statistical analysis adjusted for age verified an important risk of
developing BC when endometriosis was diagnosed in older women,
particularly those aged between 50 and 60 years (SIR, 1.28; 95% CI,
1.13–1.45). Later on, Melin et al examined the effect of
parity on the previously documented excess risk of developing
certain malignancies among women with endometriosis (26). In a new cohort study, containing the
two Swedish cohorts of Brinton et al in 1997 (21) and Melin et al in 2006 (25), overall, 63,630 women with a discharge
diagnosis of endometriosis were recruited. Through the National
Swedish Cancer Registry, 1,465 cases of BC were identified at a
mean follow-up time of 13.4 years. Eventually, the study confirmed
that the risk of developing BC was clearly increased in the women
with endometriosis, but was not affected by parity or the lack of
parity (SIR, 1.08; 95% CI, 1.02–1.13). In 2007, Bertelsen et
al evaluated the association between endometriosis and BC on
the grounds of medical history (27).
In their large Danish case-cohort study, including 114,327 women,
they encountered 236/1,978 cases of endometriosis, women who were
diagnosed with BC during a mean follow-up period of 18 years. By
Cox regression analysis, the authors observed that age at the time
of diagnosis of endometriosis influenced the risk of developing BC,
hence premenopausal (approximately ≥40) and postmenopausal women
had a significantly elevated odds ratio (OR, 2.40; 95% CI,
1.43–4.01).
Contrariwise, in 2011, Nichols et al, by a
population-based case-control study that was held in Wisconsin,
Massachusetts and New Hampshire, emphasized that women diagnosed
with endometriosis under the age of 35 years had a borderline
significant increase in the risk of developing BC (OR, 1.83; 95%
CI, 0.95–3.51), particularly those with an intact uterus and
ovaries (28). Ultimately, in 2015, a
new article, discussing the risk-spectrum of ovarian, endometrial,
breast and colorectal cancer in women with recently diagnosed
endometriosis, was published (29).
Kok et al performed a population-based cohort study by using
data from the Taiwan National Health Insurance Research Database
during the years 2003–2005. The participants had a follow-up for
cancer occurrence until December 2008. Of the 2,266 women in the
endometriosis cohort and 9,064 women in the comparison cohort, they
extracted 18 and 51 cases of BC, respectively. Cox regression
analysis adjusted to miscellaneous variants apart from parity, led
to the aggregate outcome of a ‘marginal’ risk of developing BC
among women with surgically confirmed endometriosis [hazard ratio
(HR), 1.15; 95% CI, 0.61–2.15].
Studies asserting a negative (null or
inverse) association between endometriosis and BC
Although the majority of the aforementioned studies
demonstrate a rather significant association between endometriosis
and the risk of developing BC, several other studies are supportive
of a negative correlation. First of all, Moseson et al
(19) in the small case-control study
of 354 BC cases and 747 controls described above, noted a
non-significant protective association in postmenopausal women with
a self-reported diagnosis of endometriosis (OR, 0.5; 95% CI,
0.1–2.6). In 2001, Baron et al, through a large American
case-control study including 5,659 cases of BC and 5,928 controls,
investigated the association between BC and metabolic disorders
(30). Following detailed telephone
interviews composed of a series of questions on reproductive and
medical history, overall, 303 cases of endometriosis were
identified. Eventually, their study demonstrated that women who
reported endometriosis had a modest reduction in the risk of
developing BC (OR, 0.8; 95% CI, 0.7–1.00). A year later, Olson
et al announced the results of the Iowa Women's Health Study
which was a large prospective cohort study of 37,434 participants,
aiming to pinpoint risk factors for cancer in postmenopausal women
(31). In total, 1,392 women with a
self-reported history of endometriosis were followed-up for 13
years for cancer incidence. Among the 1,795 new cases of BC, solely
67 (3.7%) cases were detected in the endometriosis group. By using
Cox proportional hazards and multivariate adjustment, the authors
found that endometriosis was not associated with a significant risk
of breast carcinoma [relative risk (RR), 0.96; 95% CI, 0.75–1.23].
In the above-quoted case-cohort study of Bertelsen et al
(27) examining the association
between different medical conditions and BC, overall, 236 cases of
endometriosis were counted among 16,983 women who laterally
developed BC between 1978 and 1998. In a Cox regression analysis
adjusted for confounding variables, a neutral association between
endometriosis and BC was declared (RR, 0.97; 95% CI, 0.85–1.11).
Moreover, women who were diagnosed with endometriosis at a young
age (>40 years) had a lower relative risk of developing BC than
the older subgroups (RR, 0.77; 95% CI, 0.61–0.96).
In a more recent US cross-sectional study published
in 2010, Gemmill et al examined the hypothesis that women
with surgically confirmed endometriosis had a higher prevalence of
other concurrent disorders, such as cancer, endocrine diseases and
infections (32). On this scope,
questionnaires from 4,331 members of the Endometriosis Association
provided efficient data for comparison with national cancer
statistics. The authors isolated only 16 women diagnosed with BC at
a mean age of 40.9 years (across all 75 cancer cases), and thus
realized that BC is less frequent in patients with endometriosis
than in the general population [prevalence odds ratio (POR), 0.54;
95% CI, 0.32–0.90; P=0.016]. Likewise, the previously reported
case-control study by Nichols et al indicated an inverse
association between endometriosis and BC (28). The main purpose of that study was to
determine whether benign indications for bilateral oophorectomy,
such as uterine fibroids and endometriosis, modify the risk of
developing BC post-menopause. The respondents to a telephone
interview were 4,935 women with a first diagnosis of invasive BC,
between the period from 1992 to 1995, and 5,111 controls. In total,
198 cases of endometriosis were found from the survey. Following
multivariate logistic regression analysis and adjustment for
potential confounders, there was no assurance of a significant risk
of developing BC among American women with a history of
endometriosis (OR, 0.99; 95% CI, 0.80–1.21). The authors also
affirmed that the risk of developing BC was not affected by the
history of bilateral oophorectomy with hysterectomy nor by the
history of an intact uterus and ovaries (OR, 0.82; 95% CI,
0.60–1.10). Of note, a strong BC risk reduction (58% lower BC risk
odds) related to bilateral oophorectomy with hysterectomy at age
≤40 years versus no surgery, was observed in the endometriosis pool
(OR, 0.42; 95% CI, 0.21–0.87; P=0.03).
In 2013, Matta et al, through a case-control
study of 991 Puerto Rican women, attempted to explore the
interrelation between endometriosis and BC, from the prospective of
DNA repair capacity (33). In their
study, among the 385 cases of BC and 606 controls recruited over a
5-year period, primary BC was diagnosed in only 20 participants
with surgically confirmed endometriosis (n=80 cases of
endometriosis). Following multiple logistic regression adjusted for
confounders, it was manifested that BC cases had 50% lower odds of
having a history of endometriosis (OR, 0.5; 95% CI, 0.3–0.9;
P=0.038) compared to the controls. Using a similar methodological
approach, Morales et al presented another case-control study
of 1,126 adult female Puerto Rican residents, evaluating the major
risk factors for BC (34). In this
larger incidence-case study, 465 cases of recently diagnosed BC and
661 controls were included. Statistical analysis revealed the
beneficial effect of endometriosis, since the risk of developing BC
was decreased by 39% (OR, 0.61; 95% CI, 0.3–1.0; P=0.039) in women
with a history of endometriosis.
Discussion
Indeed there is an extensive literature on the issue
‘endometriosis and BC’, indicative of the still indefinable
relevance between them. Apart from the aforementioned studies,
numerous other publications have highlighted various noteworthy
aspects of this topic. For instance, Melin et al underlined
that endometriosis plays a pivotal role in cancer survival, since
there was a statistically significant improved survival for women
with endometriosis and BC (HR 0.86) (35). Other studies, such as the one by
Chalas et al, proved that both premenopausal (RR, 1.9; 95%
CI, 1.35–2.70) and postmenopausal (RR, 1.9; 95% CI, 1.29–5.58)
women administered tamoxifen for the treatment/prevention for BC
were almost 2-fold more likely to develop endometriosis compared to
women on the placebo (36). Moreover,
Matalliotakis et al, in a retrospective study on a Yale
series emphasized an elevated risk associated with a family history
of BC among women with endometriosis (37).
Taking the above-mentioned data into account, in
this study, we attempted to separate our results into two different
categories, based on the criterion of the strength of the
association between endometriosis and BC, in terms of RR, OR, HR,
POR, SIR or SMR. Collectively, from our survey, we found 4
retrospective cohort studies (21,25,26,29),
4 case-control studies (19,22,24,28) and 3
case-cohort studies (20,23,27) that
demonstrate a notable risk of developing BC among women with
endometriosis (Table I). By contrast,
we gathered 5 case-control studies (19,28,30,33,34),
1 prospective cohort study (31), 1
case-cohort study (27) and 1
cross-sectional study (32) that
showed a negative association between endometriosis and BC
(Table II).
 | Table I.Overview of studies asserting a
positive (direct) association between endometriosis and breast
cancer. |
Table I.
Overview of studies asserting a
positive (direct) association between endometriosis and breast
cancer.
| Authors/(Refs.)
year | Study design (study
period) | Study size | No. of person
year | Mean follow-up
(years) | No. of
endometriosis cases | No. of BC
cases | No. of
countrols | Median age at entry
(years) | Excludes 1st year
of follow-up | Association |
|---|
| Moseson et
al (19) | Case-control | N/A | N/A | 2.3 | 6 | 354 | 747 | 55–64 | No | OR, 1.7 (95% CI,
0.6–5.1) P=0.33 |
| 1993 | (1977–1981) |
|
|
| 4a |
|
|
|
| OR, 4.3 (95% CI,
0.9–20.4) P=0.07a |
| Schairer et
al (20) | Case-cohort | 15,844 | 193,083 | 12.2 | N/A | 295 | 1,235 | 45.7 | No | SMR, 3.2 (95% CI,
1.2–8.0)b |
| 1997 | (1965–1983) |
|
|
|
|
|
|
|
| SMR, 1.7 (95% CI,
0.7–4.1)c |
| Brinton et
al (21) | Cohort | 21,398 | 216,851 | 11.4 | 20,686 | 297 | N/A | 38.8 | Yes | SIR, 1.3 (95% CI,
1.1–1.4) |
| 1997 | (1969–1983) |
|
|
|
|
|
|
|
| SIR, 1.79 (95% CI,
1.2–2.6)d |
| Weiss et al
(22) | Case-control | N/A | N/A | N/A | 53 | 2173 | 1,990 | <55 | No | RR, 1.14 (95% CI,
0.7–1.8)e |
| 1999 | (1990–1992) |
|
|
|
|
|
|
|
| RR, 1.68 (95% CI,
0.9–3.0)f |
|
|
|
|
|
|
|
|
|
|
| RR, 1.37 (95% CI,
0.7–2.5)g |
| Venn et al
(23) | Case-cohort | 29,700 | 148,672 | 7 | 3613 | 25 | 9,044 | 31 | No | SIR, 1.04 (95% CI,
0.71–1.54)h |
| 1999 | (1986–1994) |
|
|
|
|
|
|
|
|
|
| Borgfeldt and
Andolf (24) | Nested
case-control | 88,378 | N/A | N/A | 28,163 | 427 | 71165 | N/A | Yes | OR, 1.10 (95% CI,
1.0–1.2) |
| 2004 | (1969–1996) |
|
|
|
|
|
|
|
|
|
| Melin et al
(25) | Cohort | 64,492 | 766,556 | 12.7 | N/A | 1,288 | N/A | 39.4 | Yes | SIR, 1.28 (95% CI
1.13–1.45)i |
| 2006 | (1969–2000) |
|
|
|
|
|
|
|
| SIR, 1.23 (95% CI,
0.82–1.78)j |
| Melin et al
(26) | Cohort | 63,630 | 792,013 | 13.4 | N/A | 1,465 | N/A | 39.5 | Yes | SIR, 1.08 (95% CI,
1.02–1.13) |
| 2007 | (1969–2002) |
|
|
|
|
|
|
|
|
|
| Bertelsen et
al (27) | Case-cohort | 114,327 | 2,031,811 | 17.8 | 1978 | 236 | N/A | 40.6 | Yes | OR, 1.10 (95% CI,
0.90–1.34)k |
| 2007 | (1978–1998) |
|
|
|
|
|
|
|
| OR, 2.40 (95% CI,
1.43–4.01)l |
| Nichols et
al (28) | Case-control | N/A | N/A | N/A | 26m | 4,935 | 5,111 | 66.2 | No | OR, 1.83(95% CI,
0.95–3.51)m |
| 2011 | (1992–1995) |
|
|
|
|
|
|
|
|
|
| Kok et al
(29) | Cohort | N/A | 9,842 | 3 | 2266 | 18 | 9,064 | 31–50 | No | HR, 1.15 (95% CI,
0.61–2.15) |
| 2015 | (2003–2005) |
|
|
|
|
|
|
|
|
|
| Table II.Overview of studies asserting
negative (null or inverse) association between endometriosis and
breast cancer. |
Table II.
Overview of studies asserting
negative (null or inverse) association between endometriosis and
breast cancer.
| Authors/(Refs.)
year | Study design (study
period) | Study size | No. of
person-Years | Mean follow-up
(years) | No. of
endometriosis cases | No. of BC
cases | No. of
controls | Median age at entry
(years) | Excludes 1st year
of follow-up | Association |
|---|
| Moseson et
al (19) | Case-control | N/A | N/A | 2.3 | 2a | 354 | 747 | 55–64 | No | OR, 0.5 (95% CI,
0.1–2.6) P=0.40a |
| 1993 | (1977–1981) |
|
|
|
|
|
|
|
|
|
| Baron et al
(30) | Case-control | N/A | N/A | N/A | 303 | 5,659 | 5,928 | 50–79 | No | OR, 0.8 (95% CI,
0.7–1.0) |
| 2001 | (1990–1994) |
|
|
|
|
|
|
|
|
|
| Olson et al
(31) | Cohort | 37434 | N/A | 13 | 1392 | 67 | N/A | >55 | No | RR, 0.96 (95% CI,
0.75–1.23) |
| 2002 | (1986–1998) |
|
|
|
|
|
|
|
|
|
| Bertelsen et
al (27) | Case-cohort | 114,327 | 2,031,811 | 17.8 | 236 | 16,983 | N/A | 40.6 | No | RR, 0.97 (95% CI,
0.85–1.11)b |
| 2007 | (1978–1998) |
|
|
|
|
|
|
|
| RR, 0.77 (95% CI,
0.61–0.96)c |
| Gemmill et
al (32) |
Cross-sectional | 4,745 | N/A | N/A | 4,331 | 16 | N/A | 40.9 | No | POR, 0.54 (95% CI,
0.32–0.90) P=0.016 |
| 2010 | (1998–2010) |
|
|
|
|
|
|
|
|
|
| Nichols et
al (28) | Case-control | N/A | N/A | N/A | 198d | 4,935 | 5,111 | 66.2 | No | OR, 0.99 (95% CI,
0.80–1.21)d |
| 2011 | (1992–1995) |
|
|
|
| 18e |
|
|
| OR, 0.42 (95% CI,
0.21–0.87) P=0.03e |
| Matta et al
(33) | Case-control | 991 | N/A | 5 | 20 | 385 | 606 | 41–60 | No | OR, 0.5 (95% CI,
0.3–0.9) P=0.038 |
| 2013 | (2006–2012) |
|
|
|
|
|
|
|
|
|
| Morales et
al (34) | Case-control | 1,126 | N/A | 5 | 26 | 465 | 661 | 56.4 | No | OR, 0.61 (95% CI,
0.3–1.0) P=0.039 |
| 2013 | (2006–2012) |
|
|
|
|
|
|
|
|
|
On balance, our results seem to be contradictory and
require interpretation in a careful and prudent manner. To begin
with, a broad comparison between Tables
I and II shows a numerical
superiority of the studies confirming a positive association
between endometriosis and BC. Nonetheless, this is a spurious
argument, as three of these studies are included in both tables due
to the ambiguous results of each one (19,27,28).
Moreover, safe conclusions cannot be drawn due to the wide range of
the association (between 4.3–1.04 in terms of OR, RR, HR, SIR and
SMR), the different study designs and the inherent weaknesses of
such studies.
At a glance, strong evidence that women with
endometriosis are more vulnerable to later develop BC is shown in 3
case-control studies (19,22,28), 2
case-cohort studies (20,27) and in only 1 retrospective cohort study
(21). Certainly, the first
case-control study of Moseson et al (19) is not of statistical importance, by
reason of an elevated odds ratio (OR, 4.3 with wide-range CI,
0.9–20.4) pertaining to a small number of premenopausal women
(n=4), in opposition to the larger case-cohort study of Schairer
et al (20), which clarifies
that women with endometriosis who underwent hysterectomy with
ovarian retention had a higher morbidity ratio (SMR, 3.2; CI,
1.2–8.0) for BC. Next, in the case-cohort study by Bertelsen et
al (27), higher odds ratios (OR,
2.40) for BC were recorded in women diagnosed with endometriosis at
an older age (over 40 years), whereas in the case-control study of
Nichols et al (28),
comparable odds (OR, 1.83) were found in those diagnosed before the
age of 35. The cohort study of Brinton et al (21) further underlines the effect of the
localization of endometriosis, suggesting a significant incidence
ratio (SIR, 1.79) for BC in the case of the pelvic origin of the
disease. Subsequently, the wide case-control study by Weiss et
al (22) indicated a significant
relative risk of developing BC in premenopausal women ever
diagnosed with endometriosis (RR, 1.68), particularly in those who
underwent recent surgery (RR, 1.37). Lastly, the remaining 2
retrospective cohort studies of Melin et al (25,26)
illustrated a minor increase in the risk of developing BC (SIR,
1.08–1.28) related to an advanced age (>50 years) at the time of
the diagnosis of endometriosis, but not to parity.
Beyond the potential selection and detection bias of
these studies, several limitations basically concerning the
population under study and the cofounding variables, can greatly
hinder the data evaluation process. As an example, selection bias
in some studies may arise from the particular selection of women
who underwent surgery for endometriosis (20,22,29).
Detection bias in other studies may occur by the use of hospital
discharge diagnosis of endometriosis, since only the serious cases
of the disease could have been included (21,22,24–26,29).
Selection and detection bias in conjunction with the exclusion of a
large number of cancer patients as ineligible candidates may have
resulted in an underestimation of the true risk of developing BC.
The self-reported history of endometriosis by questionnaires or
telephone interviews may also have led to recall bias (19,28), and
consequently to an overestimation of the overall risk. A point
often overlooked is that women participants in certain studies were
in their vast majority, postmenopausal (19,28) or
premenopausal (20,27), whereas other studies included entirely
young women (23). The intervals of
follow-up, as well, differ amidst studies with a wide range from
2.3 to 17.8 years (19,27). Particularly problematic in the
majority of studies is the analysis with adjustment for numerous
confounders, such as age, race, parity, hysterectomy status, family
history of BC, mammograms and body mass index (BMI) (22,27).
Another drawback is the lack of data on endometriosis staging by
the revised American Society for Reproductive Medicine (rASRM), on
the histological type of BC, as well as on treatment regimens.
After all, the increased risk of developing BC in postmenopausal
women may be attributed to common risk factors between
endometriosis and BC or to hormone replacement treatment or to
altered endogenous estrogens (20,27).
Comparatively, young women on danazol/GnRH agonists treatment for
endometriosis may have a long term protection against BC (27). On the other hand, we found only 1
prospective cohort study (31), 1
case-cohort study (27) and 1
case-control study (28) supporting a
null association between endometriosis and BC. As can be seen, the
major limitation in the study of Olson et al (31) is that the population under study was
strictly menopausal (>55 years) at entry, and thus a possible
degradation of the true BC must be taken into account, given the
short latency period between endometriosis and BC occurrence.
Another weak point of this cohort is the self-reports and not the
surgical confirmation of endometriosis, which may have also
affected the risk estimates. Furthermore, we collected 5
case-control studies (19,28,30,33,34)
and 1 cross-sectional study (32),
providing evidence that women with endometriosis are less likely to
develop BC. A closer look at these reveals participant groups of
premenopausal and postmenopausal women, short follow-up intervals
and variation in effect sizes (in OR) between 0.42 (28) and 0.8 (30). Two of these studies also refer
exclusively to Puerto Rican women (33,34). In
fact, several limitations related to implicit sources of bias in
such studies preclude the acceptance of an inverse association
between endometriosis and BC.
In summary, our conclusions are in accordance with
those of previously published surveys on the same issue thus far,
confirming the lack of data and inconsistent results among studies
(38–40). As regards the clarification of a
‘robust’ or ‘weak’ association between endometriosis and BC, no
definite conclusions can be drawn from our survey, due to the
limited number of studies and the limitations of each of these
studies. Importantly, new studies are urgently required to
investigate whether women with endometriosis have a predisposition
to develop BC, taking into consideration the high mortality rate
associated with BC worldwide. Large well-designed, adequately
powered, prospective cohort or randomized control trials with long
term follow-up periods are thus warranted in order to provide
evidence-based clinical recommendations for proper counseling,
screening and treatment strategies for such patients, and hence to
improve public health.
Glossary
Abbreviations
Abbreviations:
|
BC
|
breast cancer
|
|
RR
|
relative risk
|
|
OR
|
odds ratio
|
|
POR
|
prevalence odds ratio
|
|
HR
|
hazard ratio
|
|
SIR
|
standardized incidence ratio
|
|
SMR
|
standardized morbidity ratio
|
|
CI
|
confidence interval
|
|
IVF
|
in vitro fertilization
|
|
rASRM
|
revised American Society for
Reproductive Medicine
|
|
BMI
|
body mass index
|
References
|
1
|
Crosignani P, Olive D, Bergqvist A and
Luciano A: Advances in the management of endometriosis: An update
for clinicians. Hum Reprod Update. 12:179–189. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ozkan S, Murk W and Arici A: Endometriosis
and infertility: Epidemiology and evidence-based treatments. Ann NY
Acad Sci. 1127:92–100. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bulletti C, Coccia ME, Battistoni S and
Borini A: Endometriosis and infertility. J Assist Reprod Genet.
27:441–447. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sourial S, Tempest N and Hapangama DK:
Theories on the pathogenesis of endometriosis. Int J Reprod Med.
2014:1795152014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Burney RO and Giudice LC: Pathogenesis and
pathophysiology of endometriosis. Fertil Steril. 98:511–519. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Missmer SA, Hankinson SE, Spiegelman D,
Barbieri RL, Marshall LM and Hunter DJ: Incidence of
laparoscopically confirmed endometriosis by demographic,
anthropometric, and lifestyle factors. Am J Epidemiol. 160:784–796.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mehedintu C, Plotogea MN, Ionescu S and
Antonovici M: Endometriosis still a challenge. J Med Life.
7:349–357. 2014.PubMed/NCBI
|
|
8
|
Thomas EJ and Campbell IG: Evidence that
endometriosis behaves in a malignant manner. Gynecol Obstet Invest.
50(Suppl 1): 2–10. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kokcu A: Relationship between
endometriosis and cancer from current perspective. Arch Gynecol
Obstet. 284:1473–1479. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kvaskoff M, Mu F, Terry KL, Harris HR,
Poole EM, Farland L and Missmer SA: Endometriosis: A high-risk
population for major chronic diseases? Hum Reprod Update.
21:500–516. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Roy D, Morgan M, Yoo C, Deoraj A, Roy S,
Yadav VK, Garoub M, Assaggaf H and Doke M: Integrated
bioinformatics, environmental epidemiologic and genomic approaches
to identify environmental and molecular links between endometriosis
and breast cancer. Int J Mol Sci. 16:25285–25322. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fung JN, Holdsworth-Carson SJ, Sapkota Y,
Zhao ZZ, Jones L, Girling JE, Paiva P, Healey M, Nyholt DR, Rogers
PA and Montgomery GW: Functional evaluation of genetic variants
associated with endometriosis near GREB1. Hum Reprod. 30:1263–1275.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tao Z, Shi A, Lu C, Song T, Zhang Z and
Zhao J: Breast Cancer: Epidemiology and Etiology. Cell Biochem
Biophys. Dec 28–2014.(Epub ahead of print).
|
|
14
|
Shah R, Rosso K and Nathanson SD:
Pathogenesis, prevention, diagnosis and treatment of breast cancer.
World J Clin Oncol. 5:283–298. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Breast Cancer Screening (PDQ®): Health
Professional Version. Authors PDQ Screening and Prevention
Editorial Board. SourcePDQ Cancer Information Summaries [Internet]
(Bethesda (MD)). National Cancer Institute (US). Jul
14–2002.2015.
|
|
16
|
Goyeneche AA and Telleria CM:
Antiprogestins in gynecological diseases. Reproduction.
149:R15–R33. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gierisch JM, Coeytaux RR, Urrutia RP,
Havrilesky LJ, Moorman PG, Lowery WJ, Dinan M, McBroom AJ,
Hasselblad V, Sanders GD, et al: Oral contraceptive use and risk of
breast, cervical, colorectal, and endometrial cancers: A systematic
review. Cancer Epidemiol Biomarkers Prev. 22:1931–1943. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Prentice RL: Postmenopausal hormone
therapy and the risks of coronary heart disease, breast cancer, and
stroke. Semin Reprod Med. 32:419–425. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Moseson M, Koenig KL, Shore RE and
Pasternack BS: The influence of medical conditions associated with
hormones on the risk of breast cancer. Int J Epidemiol.
22:1000–1009. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schairer C, Persson I, Falkeborn M,
Naessen T, Troisi R and Brinton LA: Breast cancer risk associated
with gynecologic surgery and indications for such surgery. Int J
Cancer. 70:150–154. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Brinton LA, Gridley G, Persson I, Baron J
and Bergqvist A: Cancer risk after a hospital discharge diagnosis
of endometriosis. Am J Obstet Gynecol. 176:572–579. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Weiss HA, Brinton LA, Potischman NA,
Brogan D, Coates RJ, Gammon MD, Malone KE and Schoenberg JB: Breast
cancer risk in young women and history of selected medical
conditions. Int J Epidemiol. 28:816–823. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Venn A, Watson L, Bruinsma F, Giles G and
Healy D: Risk of cancer after use of fertility drugs with in-vitro
fertilisation. Lancet. 354:1586–1590. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Borgfeldt C and Andolf E: Cancer risk
after hospital discharge diagnosis of benign ovarian cysts and
endometriosis. Acta Obstet Gynecol Scand. 83:395–400. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Melin A, Sparén P, Persson I and Bergqvist
A: Endometriosis and the risk of cancer with special emphasis on
ovarian cancer. Hum Reprod. 21:1237–1242. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Melin A, Sparén P and Bergqvist A: The
risk of cancer and the role of parity among women with
endometriosis. Hum Reprod. 22:3021–3026. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bertelsen L, Mellemkjaer L, Frederiksen K,
Kjaer SK, Brinton LA, Sakoda LC, van Valkengoed I and Olsen JH:
Risk for breast cancer among women with endometriosis. Int J
Cancer. 120:1372–1375. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Nichols HB, Visvanathan K, Newcomb PA,
Hampton JM, Egan KM, Titus-Ernstoff L and Trentham-Dietz A:
Bilateral oophorectomy in relation to risk of postmenopausal breast
cancer: Confounding by nonmalignant indications for surgery? Am J
Epidemiol. 173:1111–1120. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kok VC, Tsai HJ, Su CF and Lee CK: The
risks for ovarian, endometrial, breast, colorectal, and other
cancers in women with newly diagnosed endometriosis or adenomyosis:
A population-based study. Int J Gynecol Cancer. 25:968–976. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Baron JA, Weiderpass E, Newcomb PA,
Stampfer M, Titus-Ernstoff L, Egan KM and Greenberg ER: Metabolic
disorders and breast cancer risk (United States). Cancer Causes
Control. 12:875–880. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Olson JE, Cerhan JR, Janney CA, Anderson
KE, Vachon CM and Sellers TA: Postmenopausal cancer risk after
self-reported endometriosis diagnosis in the Iowa Women's Health
Study. Cancer. 94:1612–1618. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Gemmill JA, Stratton P, Cleary SD, Ballweg
ML and Sinaii N: Cancers, infections, and endocrine diseases in
women with endometriosis. Fertil Steril. 94:1627–1631. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Matta JL, Flores I, Morales LM, Monteiro
J, Alvarez-Garriga C and Bayona M: Women with endometriosis have a
higher DNA repair capacity and diminished breast cancer risk. Mol
Cancer Biol. 1:12013.
|
|
34
|
Morales L, Alvarez-Garriga C, Matta J,
Ortiz C, Vergne Y, Vargas W, Acosta H, Ramírez J, Perez-Mayoral J
and Bayona M: Factors associated with breast cancer in Puerto Rican
women. J Epidemiol Glob Health. 3:205–215. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Melin A, Lundholm C, Malki N, Swahn ML,
Sparen P and Bergqvist A: Endometriosis as a prognostic factor for
cancer survival. Int J Cancer. 129:948–955. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chalas E, Costantino JP, Wickerham DL,
Wolmark N, Lewis GC, Bergman C and Runowicz CD: Benign gynecologic
conditions among participants in the Breast Cancer Prevention
Trial. Am J Obstet Gynecol. 192:1230–1239. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Matalliotakis IM, Cakmak H, Mahutte N,
Goumenou AG, Koumantakis G and Arici A: The familial risk of breast
cancer in women with endometriosis from Yale series. Surg Oncol.
17:289–293. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Munksgaard PS and Blaakaer J: The
association between endometriosis and gynecological cancers and
breast cancer: A review of epidemiological data. Gynecol Oncol.
123:157–163. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Vlahos NF, Economopoulos KP and Fotiou S:
Endometriosis, in vitro fertilisation and the risk of
gynaecological malignancies, including ovarian and breast cancer.
Best Pract Res Clin Obstet Gynaecol. 24:39–50. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Anifantaki FI, Boutas I, Kalampokas T,
Kalampokas E, Sofoudis C and Salakos N: Association of
endometriosis and breast cancer: Mini review of the literature.
Arch Gynecol Obstet. Jul 03–2015.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|