Introduction
Neuroendocrine carcinomas (NECs) comprise a
heterogeneous group of neoplasms, which arise from peptide- or
amine-producing endocrine cells throughout the body (1). This type of tumor is mainly encountered
in the lungs. Extrapulmonary counterparts are rarely encountered,
although they have been described in a variety of organs, including
the esophagus, stomach, pancreas, gallbladder, uterine cervix,
kidney, urinary bladder and prostate gland (2). To the best of our knowledge, there are
only few case reports of NECs located in the genitourinary tract,
with the majority of cases reported in the bladder, whereas tumors
originating from the ureter are extremely rare (3). The histogenesis of this type of tumor
has not been fully elucidated, although several hypotheses have
been suggested. Furthermore, due to its rarity, the clinical
behavior and theory underlying the development of primary NEC of
the ureter have not been well established. The aim of the present
study was to report the clinical and pathological characteristics
and management of a case of NEC with combined small-cell and
atypical carcinoid components. In the light of the present case
report, a recent systematic literature review of the clinical
presentation and management of this rare tumor was also performed.
Written informed consent was obtained from the patient's
family.
Case report
A 69-year-old Chinese Han male patient was admitted
to the Department of Urology of Tianjin First Central Hospital
(Tianjin, China) with a 10-month history of gross hematuria and
1-month history of left flank pain. The medical history of the
patient included 17 years of hypertension, 20 years of coronary
heart disease and an allergy to iodine. The findings of the
physical examination were normal. The findings of the routine
laboratory examinations were unremarkable. However, on urinalysis,
there was macroscopic hematuria and 40–50 white blood cells per
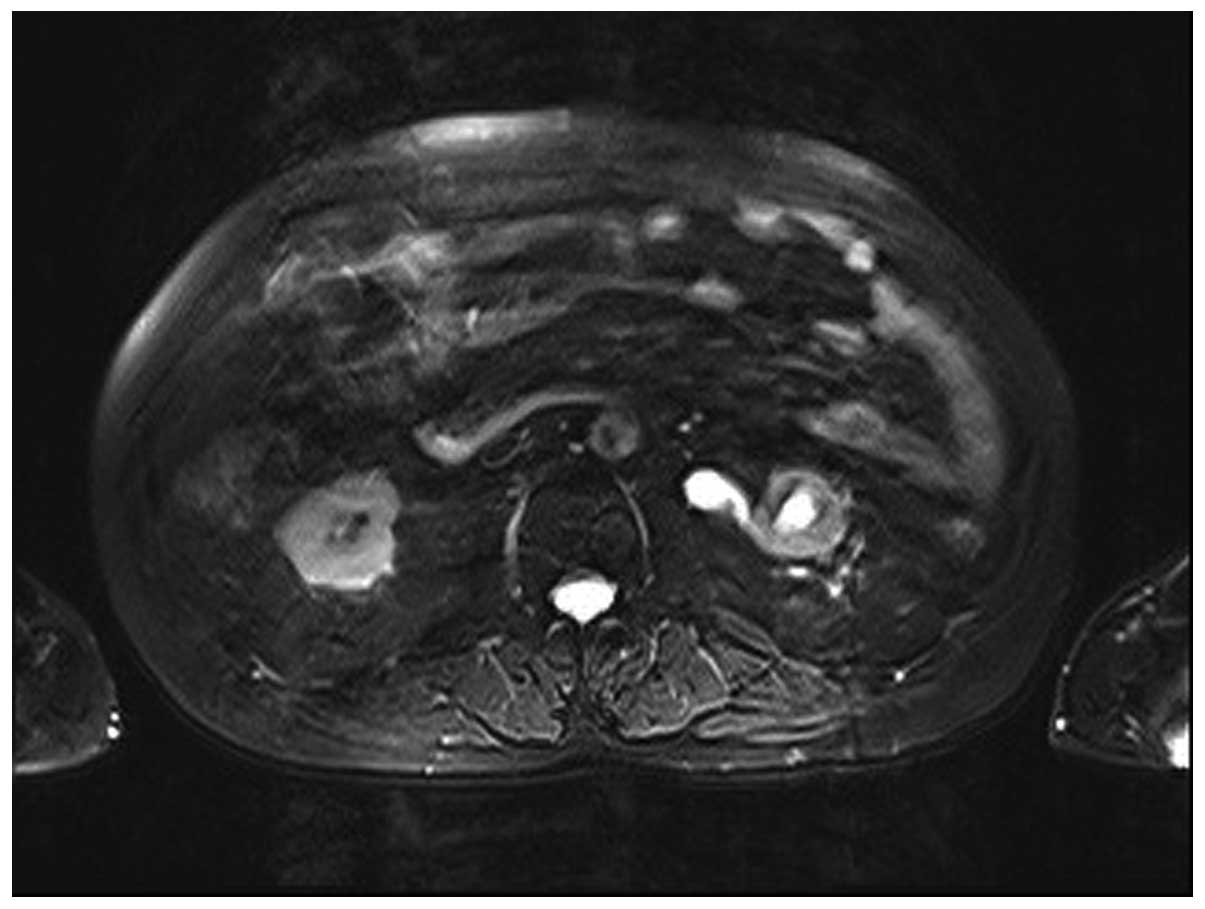
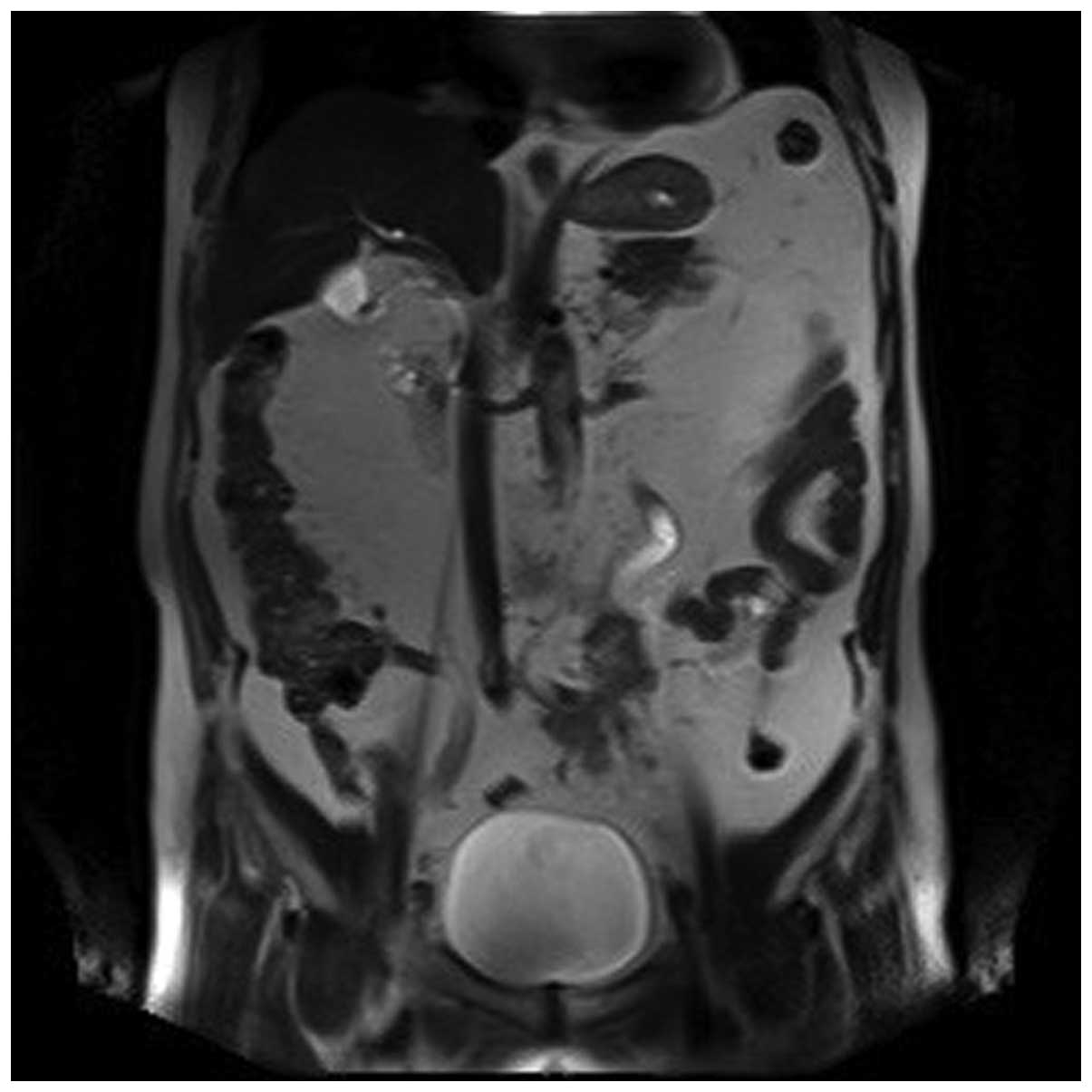
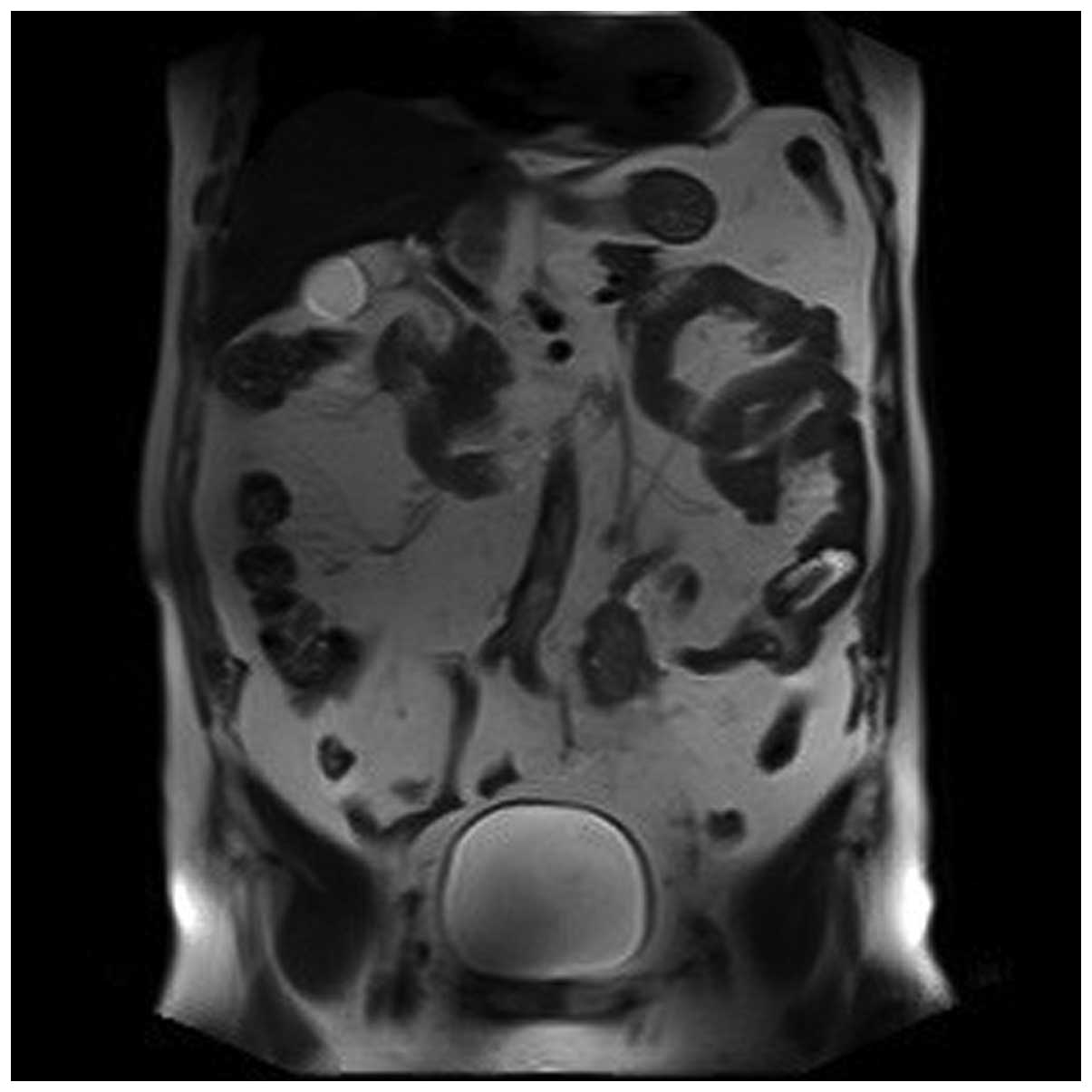
high-power field. On magnetic resonance imaging of the urinary
tract, the iliac wing level around the left ureter exhibited an
iso-intense T2 signal, an irregular mass with a rough outline and
unclear boundaries of the corresponding level of the left iliac
vessels. There was occlusion of the left ureter at the
corresponding level, with hydronephroureterosis above the mass and
undevelopment of the segment of the left ureter below the mass
(Figs. 1, 2 and 3). The
right kidney was normal. Chest radiographs were performed and
revealed no primary or metastatic lung lesions. Left
nephroureterectomy was performed and the clinical diagnosis was
primary ureteral tumor. The gross examination revealed an ovoid,
solid, white mass, sized 3.5×3.0×1.6 cm, originating from the
ureteral mucosa and protruding into the ureteral lumen, with
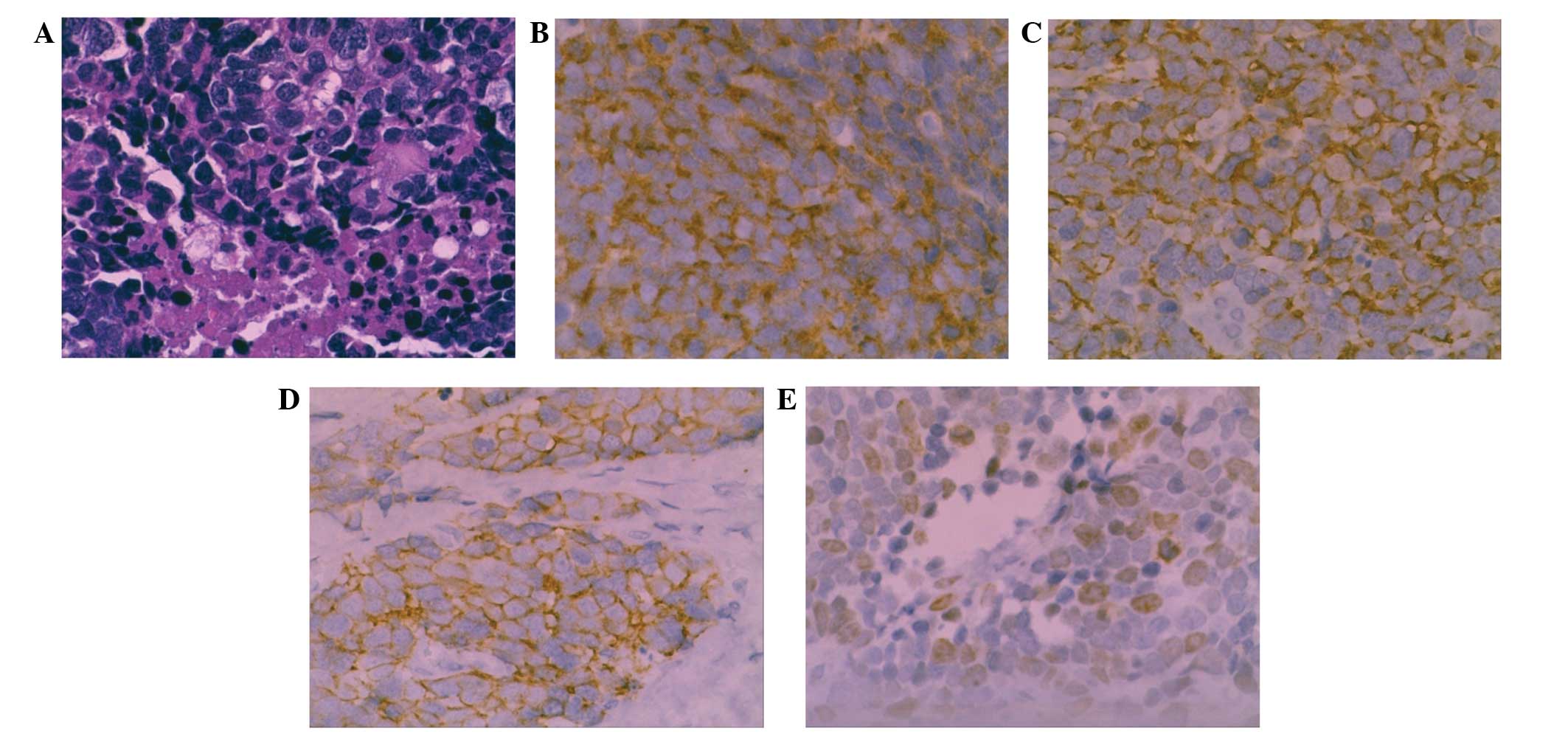
invasion of the periureteral adipose tissue. Examination under a
light microscope revealed that the tumor was composed of atypical
carcinoid cells with diverse shapes, with common mitotic figures,
and small cells with a round to fusiform shape, scant cytoplasm,
fine granular nuclear chromatin, and absent or inconspicuous
nucleoli (Fig. 4). The tumor cells
exhibited cytoplasmic positivity for cytokeratin (CK)7, epithelial
membrane antigen (EMA), CD56 and synaptophysin, and negativity for
neuron-specific enolase (NSE), chromogranin A (CgA) and CK20. The
Ki-67/MIB1 index was 20%. The patient was diagnosed with NEC of the
ureter with atypical carcinoid and small-cell carcinoma components.
The postoperative recovery of the patient was uncomplicated;
however the patient refused chemotherapy or radiotherapy. During
the regular follow-up examinations, there was no evidence of tumor
recurrence at 5 months postoperatively; however, he succumbed to
extensive metastases after 12 months of follow-up.
Discussion
The types of NEC include large-cell NEC, giant-cell
NEC, small-cell carcinoma, carcinoid and atypical carcinoid tumors.
The term ‘NEC’ describes a heterogeneous group of tumors
originating from neuroendocrine cells in different organs.
Approximately 74% of these tumors originate in the gastrointestinal
tract and 10% originate in the lungs, whereas the remainder are
scattered in various systems (1).
NECs arising from the urinary tract are extremely rare and
represent <0.5% of urinary tract tumors (3). Among these, primary NECs of the kidney,
ureter, bladder and prostate are the most commonly reported, with
the majority originating in the bladder, while primary NECs
originating in the ureter are extremely rare. Due to the low
incidence of ureteral NECs, these tumors are poorly understood and
their origin remains controversial. The following four hypotheses
have been suggested for the origin of the tumors: i) The urothelium
with neuroendocrine differentiation; ii) neuroendocrine cells
present in the urinary tract; iii) the entrapped neural crest in
the ureter during embryogenesis; and iv) undifferentiated stem
cells that differentiate towards a urothelial or squamous cell
lineage (4,5).
NECs of the ureter are similar to other urothelial
carcinomas. The most common symptoms include intermittent painless
gross or microscopic hematuria, blunt pain in the lower back in a
proportion of the patients, whereas a few patients present with the
syndrome of inappropriate antidiuretic hormone secretion. The
diagnosis mainly relies on histology. NECs do not usually consist
of more than a single tissue type (6). Similar to other types of NEC, the
pathological characteristics of urinary NEC are as follows: i)
Large-cell NEC consists of large cells typically exhibiting
significant pleiomorphism, large nuclei with coarse and granular
chromatin and prominent nucleoli, often with significant mitotic
activity and palisading with rosette formation with a sheet-like
and trabecular growth patterns, usually with extensive necrosis
(7); ii) giant-cell NEC mainly
consists of larger cancer cells of different forms, multinucleated
giant cells, common mitotic figures and extensive necrosis
(8); iii) small-cell carcinoma
consists of small cells of uniform shape, with little or no
cytoplasm, round nuclei, unclear cell boundaries, forming flaky or
nested cell masses, with large areas of necrosis; iv) carcinoids
consist of cells that are histologically medium-sized with
consistent shape and size, round or oval centrally located nuclei,
with rare or absent mitotic figures; the cells are arranged in
nests, islets, trabeculae, or cords, with palisading; and v)
atypical carcinoids exhibit microscopic characteristics similar to
carcinoids, although with greater nuclear atypia, higher mitotic
activity and focal necrosis. The overall microscopic morphology is
inconsistent, with atypical characteristics and common mitotic
figures (2–4/10 high-power field), with the cancer cells arranged
in trabeculae, cords or nests. Suspected cases should undergo
immunohistochemical examination, including the detection of CKs and
EMA, which contribute to the diagnosis of the disease.
Ureteral small-cell carcinoma, large-cell NEC and
giant-cell NEC are the most highly malignant among these five types
of NECs, exhibiting strong invasiveness and poor prognosis. We
herein report a case of small-cell carcinoma combined with of
atypical carcinoid characteristics. The patient refused
chemotherapy and radiotherapy following surgery, and succumbed to
the disease after 12 months of follow-up. The treatment principle
for this disease is the use of combined therapies with surgical
excision. If the tumor is completely surgically resectable, it may
significant improve the survival rate and quality of life. The
surgical method usually selected is open radical resection with
excision of a bladder cuff. As the tumor is often larger and may
have already metastasized by the time the patient seeks a
consultation, radical resection should be performed as early as
possible. In addition, due to the advanced stage and early
micro-metastases, tumors often cannot be completely removed;
therefore, radical surgical resection alone usually does not
prevent disease progression. Chemotherapy and radiotherapy
following surgery are often required for effective treatment.
However, the treatment modalities (surgery, chemotherapy and
radiotherapy) are not optimally defined due to the rarity of these
tumors. A potential benefit has been suggested with adjuvant
chemotherapy. Treatment of disseminated disease is based on
chemotherapy with a platinum agent (9–11).
NECs are aggressive tumors that usually present at
an advanced stage. The diagnosis mainly relies on pathological
characteristics. The prognosis is poorer compared with that of
urothelial cancer. Due to the lack of prospective studies, there is
currently no standard therapeutic approach. For localized disease,
aggressive surgical treatment combined with adjuvant chemotherapy
may prolong overall and disease-free survival. For metastatic
disease, chemotherapy using a platinum agent is currently the
mainstay of treatment.
References
|
1
|
Volante M, Rindi G and Papotti M: The grey
zone between pure (neuro) endocrine and non-(neuro) endocrine
tumours: a comment on concepts and classification of mixed
exocrine-endocrine neoplasms. Virchows Arch. 449:499–506. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kim JH, Lee SH, Park J, et al:
Extrapulmonary small-cell carcinoma: a single-institution
experience. Jpn J Clin Oncol. 34:250–254. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ping JH, Chen ZX, Jiong Q, Han YQ and Nong
X: Small cell neuroendocrine carcinoma of the ureter: A case report
and literature review. Oncol Lett. 7:728–730. 2014.PubMed/NCBI
|
|
4
|
Banerji JS, Korula A and Panicker JB:
Multicentric small cell neuroendocrine neoplasm of the renal pelvis
and ureter with concomitant focal high-grade urothelial carcinoma
of the ureter: A case report. Indian J Urol. 24:571–574. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fetissof F, Dubois MP, Lanson Y and Jobard
P: Endocrine cells in renal pelvis and ureter, an
immunohistochemical analysis. J Urol. 135:420–421. 1986.PubMed/NCBI
|
|
6
|
Kim TS, Seong DH and Ro JY: Small cell
carcinoma of the ureter with squamous cell and transitional cell
carcinomatous components associated with ureteral stone. J Korean
Med Sci. 16:796–800. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shin MK, Choi CM, Oh YJ and Kim NI: CK20
Positive Large-cell neuroendocrine carcinoma presenting with skin
metastases. Ann Dermatol. 23(Suppl 1): S20–S24. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dundr P, Pesl M, Povýsil C, Vítková I and
Dvorácek J: Large cell neuroendocrine carcinoma of the urinary
bladder with lymphoepithelioma-like features. Pathol Res Pract.
199:559–563. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Debry C, Rouyer N, Grandjean E, Gentine A,
Stierle JL and Conraux C: Neuroendocrine giant-cell epithelioma.
Description of a clinical case and review of the literature. Ann
Otolaryngol Chir Cervicofac. 109:345–350. 1992.(In French).
PubMed/NCBI
|
|
10
|
Coelho HM, Pereira BA and Caetano PA:
Large cell neuroendocrine carcinoma of the urinary bladder: case
report and review. Curr Urol. 7:155–159. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ahsaini M, Riyach O, Tazi MF, et al: Small
cell neuroendocrine carcinoma of the urinary tract successfully
managed with neoadjuvant chemotherapy. Case Rep Urol.
2013:5983252013.PubMed/NCBI
|