Introduction
Not all patients with organ-confined prostate cancer
treated with radical prostatectomy experience long-term disease
control. Increasing levels of prostate-specific antigen (PSA)
following surgery due to biochemical relapse (BCR) typically
precede the development of clinical recurrence. In the setting of
BCR without detectable distant metastases, salvage radiotherapy to
the prostate bed is an established therapeutic option (1–6), based on
the assumption that all residual cancer cells are located there.
Two different immediate results might be observed: success, as
indicated by PSA decline (possibly followed by relapse during
follow-up), or failure, as indicated by unaffected PSA progression.
In the case of immediate failure (or a continuous increase in PSA),
the hypothesis is proved incorrect: in these patients, the residual
cancer cells are not located in the prostate bed. The imaging
methods currently in use are unable to detect microscopic cancer
deposits. Therefore, optimal patient selection needs to be based on
other approaches. Pre-treatment identification of all patients who
are likely to develop continuously rising PSA despite radiotherapy
to the prostate bed would be desirable as these patients could be
considered for other therapies. The purpose of this study was to
analyze predictive factors for continuous PSA increase, and to
describe the pattern of radiologically detected recurrences during
follow-up. We perform a retrospective comparison of two patient
groups with PSA decline or continuous increase following salvage
radiotherapy to the prostate bed.
Patients and methods
This retrospective analysis included 83 males with
prostate cancer treated with radical prostatectomy who had
persistently elevated PSA or who developed BCR, i.e. PSA >0.2
ng/ml, after non-detectable PSA immediately after surgery. The
patients were treated with 3-D conformal salvage radiotherapy at
the University Hospital in Tromsø or the affiliated academic
teaching hospital Nordland Hospital in Bodø, Norway. The patients
were treated between 2006 and 2014. The study was performed as a
retrospective analysis of salvage radiotherapy. As a quality of
care analysis, no approval from the Regional Committee for Medical
and Health Research Ethics (REK) was necessary. None of the
patients had clinical or radiological evidence of macroscopic
disease following isotope bone scan, computed tomography (CT) of
the pelvis and abdomen, and magnetic resonance imaging of the
pelvis. Positron-emission tomography (PET)-CT was not used.
Patients with node-positive disease at the time of surgery or
re-staging were not included. In addition to N0 stage, all patients
were required to have had a maximum PSA of 2.0 ng/ml at the time of
salvage radiotherapy and to be endocrine treatment-naïve. The
patient characteristics are shown in Table I. The dose was prescribed according to
the the ICRU 50 guidelines. The 95% isodose line encompassed the
planning target volume (PTV) and the maximum dose did not exceed
107% of the prescribed dose. The dose per fraction was 2 Gy, and
the total dose was 70 Gy. CT scans were used to define the clinical
target volume (CTV) based on histological and surgical reports. The
prostate bed was contoured and in case of seminal vesicle
involvement the CTV was expanded to include this area. None of the
patients received treatment to the pelvic lymph nodes. The margins
added to the CTV to create the PTV were 1 cm in all directions. All
patients were treated with 6–15 MV photons from a linear
accelerator via 4 to 6 individually shaped treatment fields.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
|
| Continuous PSA
increase | PSA decline | Significance
level |
|---|
| Parameter | (n=21) | (n=62) | (if P<0.2) |
|---|
| Median age, years
(range) | 64 (57–70) | 64 (51–71) |
|
| Median PSA (ng/ml)
before surgery | 8.8 (3.1–19.0) | 9.0 (2.8–35.0) |
|
| Median PSA before RT
(range) | 0.6 (0.3–1.8) | 0.5 (0.2–2.0) | 0.176 |
| Median interval to
RT, months | 16 (3–86) | 25 (4–101) | 0.195 |
| PSA detected
cancer | 12 | 35 |
|
| Clinically
symptomatic cancer | 9 | 27 |
|
| Pre-surgery low-risk
diseasea | 2 | 11 |
|
| Pre-surgery
intermediate risk disease | 13 | 40 |
|
| Pre-surgery high-risk
disease | 5 (1 unknown) | 11 |
|
| Gleason score
differenceb | 10 | 33 |
|
| No Gleason score
difference | 11 | 29 |
|
| Perineural
infiltration | 13 | 38 |
|
| No perineural
infiltration | 8 | 24 |
|
| Involved margin
(R1) | 8 | 40 |
|
| Clear margin
(R0) | 12 (1 unknown) | 21 (1 unknown) | 0.066 |
| Post-surgery Gleason
score 3+3 | 1 | 10 |
|
| Post-surgery Gleason
score 3+4 | 6 | 29 |
|
| Post-surgery Gleason
score 4+3 | 6 | 10 |
|
| Post-surgery Gleason
score 3+5 | 0 | 2 |
|
| Post-surgery Gleason
score 4+4 | 1 | 5 |
|
| Post-surgery Gleason
score 9 | 7 | 4 (2 unknown) | 0.007 |
| Post-surgery T stage
2 | 11 | 32 |
|
| Post-surgery T stage
3a | 5 | 23 |
|
| Post-surgery T stage
3b | 4 (1 unknown) | 7 |
|
| Lymph node
dissectionc | 7 | 19 |
|
| No lymph node
dissection | 14 | 43 |
|
| Charlson comorbidity
index 0 | 12 | 34 |
|
| Comorbidity
presentd | 8 (1 unknown) | 28 |
|
Biochemical relapse-free survival
(BRFS) and further treatment
A biochemical recurrence following salvage
radiotherapy was defined as a PSA value above 0.2 ng/ml. PSA was
assessed every 3 months following radiotherapy. We defined
continuous rise as at least two subsequent PSA increases from the
pre-radiotherapy level. Re-staging following radiotherapy included
the same imaging modalities as mentioned above; i.e. no PET-CT. The
timing of imaging and additional treatment following BCR was at the
discretion of the patient's urologist. No uniform criteria for any
intervention were applied.
Statistical analysis
The Chi-square test and Fisher's exact test, where
applicable, were employed for comparison of dichotomous variables,
and the Mann-Whitney U test was employed for continuous variables.
The Kaplan-Meier method was employed for estimates of BRFS and
metastasis-free survival from the initiation of salvage
radiotherapy. P<0.05 was considered to indicate a statistically
significant difference. All tests were two-sided.
Results
Of the 83 patients, 21 developed continuously rising
PSA. The others responded biochemically (51 completely, i.e. PSA
<0.2 ng/ml, and 11 partially, i.e. a variable degree of PSA
decline). There was a trend towards a shorter interval between
surgery and radiotherapy in patients with continuous PSA increase
(P=0.07 if the cut-off was set to <24 vs. ≥24 months). There was
also a trend towards higher rates of R0 resection, i.e. no
microscopically involved margins, in patients with continuous PSA
increase (P=0.066). Thirty-six percent of patients with R0
resection developed continuously rising PSA, compared with 17% of
patients with involved margins. Sixty-four percent of patients with
Gleason score 9 developed continuously rising PSA. The Gleason
score was the only statistically significant risk factor (P=0.007).
Of the five patients with Gleason score 9 and perineural invasion,
four developed continuously rising PSA. Neither pre- nor
post-surgical risk classification (low, intermediate or high) were
significantly associated with the risk of continuous PSA increase.
Neither the diagnosis of pT3b stage nor simultaneous presence of
two high-risk features was a significant risk factor.
Table II shows the
outcome parameters in the groups with different PSA responses.
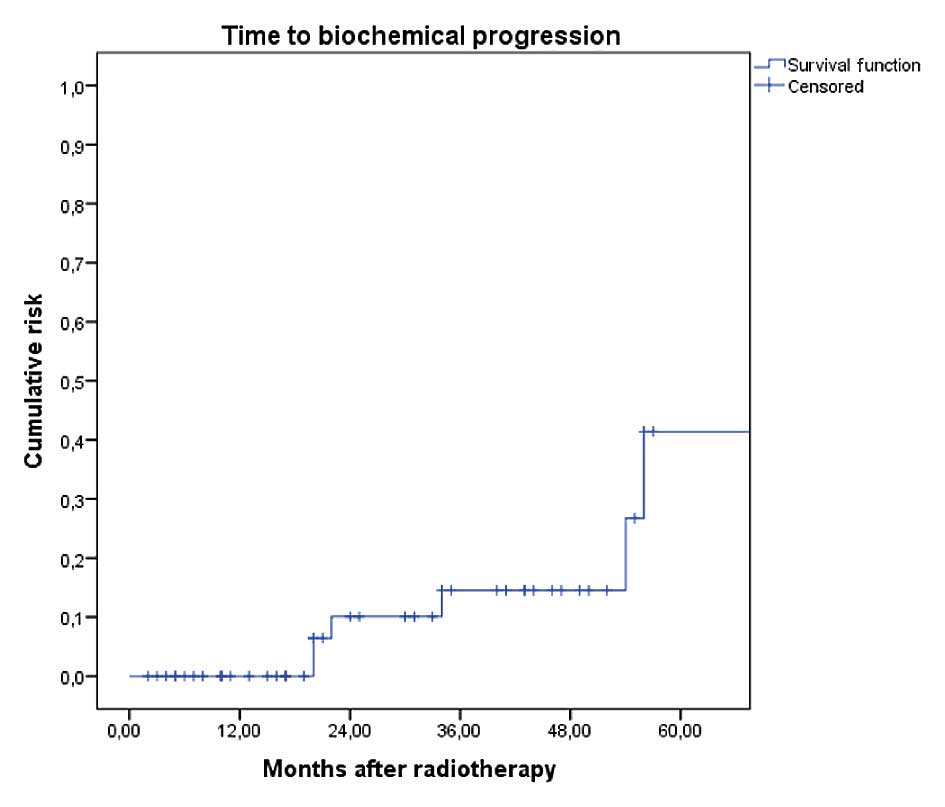
Figure 1 shows actuarial BRFS in
patients with optimal initial response, i.e. PSA nadir <0.2
ng/ml. Patients without PSA relapse had a median follow-up of 21
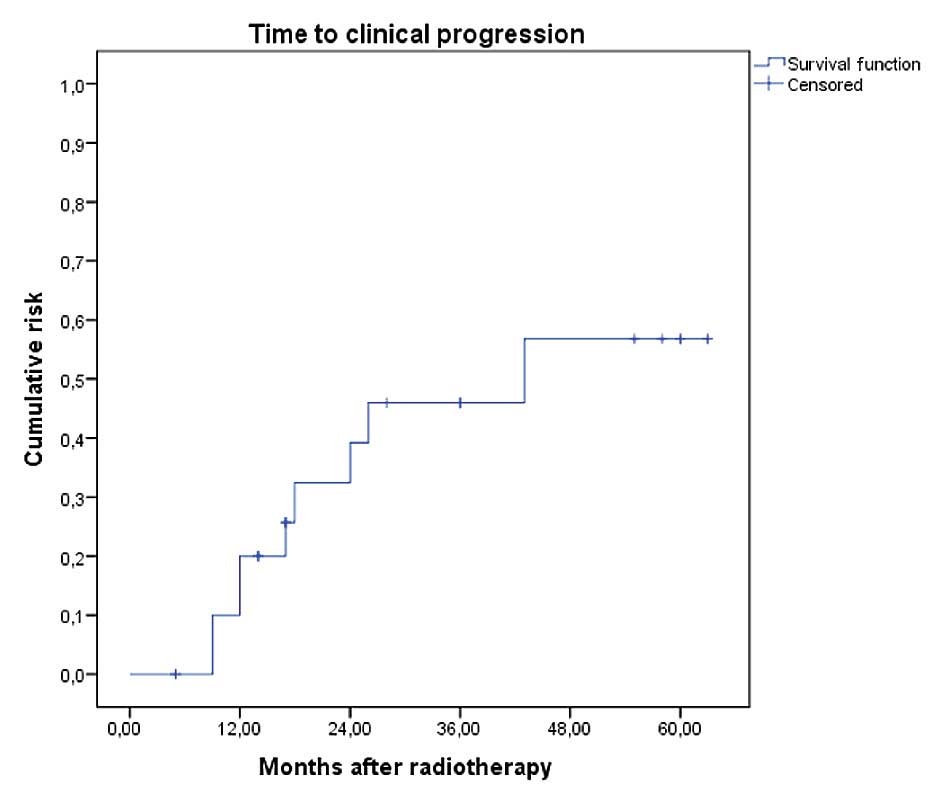
months. Figure 2 shows the actuarial
time to radiological recurrence in patients with continuous PSA
increase. A total of nine recurrences were detected (three in
pelvic nodes only, three in pelvic and para-aortic nodes
simultaneously, and three cases with bone metastases), and one
patient succumbed 23 months after the diagnosis of bone metastases.
Isolated pelvic nodal recurrence was uncommon. The median time to
radiological recurrence was 43 months. The median follow-up time in
patients without detectable macroscopic recurrence was 32 months.
Eight of the nine patients with radiological recurrence had
high-risk disease (all stage pT3, four with Gleason score 9). The
remaining patient (isolated pelvic nodal relapse) had initial PSA
19 ng/ml, stage pT2c and Gleason score 3+4. Three patients were
already on endocrine treatment when radiological relapse was
detected, and the others started afterwards. Eight of the 12
patients without detectable macroscopic recurrence started
endocrine treatment during follow-up.
| Table II.Prostate-specific antigen outcome
during follow-up. |
Table II.
Prostate-specific antigen outcome
during follow-up.
| Parameter | Continuous PSA
increase (n=21) | PSA decline to nadir
<0.2 ng/ml (n=51) | PSA decline to nadir
≥0.2 ng/ml (n=11) |
|---|
| New biochemical
relapse following salvage RT | 21, immediately after
RT | 5, during follow-up
(Fig. 1) | 8, during
follow-up |
Discussion
The purpose of this study was to analyze predictive
factors for continuous PSA increase following salvage radiotherapy
to the prostate bed, and to describe the pattern of radiologically
detected recurrence during follow-up. We selected this endpoint as
patients whose biochemical disease progression remains unaffected
by radiotherapy to the prostate bed represent a group that does not
benefit from such treatment and rather requires other approaches.
Of course, there is also a certain risk of disease progression in
patients with initial PSA response (7–10).
However, previous studies suggest that the time interval between
post-radiotherapy BCR and overt metastatic disease is often so long
that life expectancy is not affected (11,12). Our
patients with continuous PSA increase had a median age of 64 years
and a median interval to radiological recurrence of 43 months.
Together with the fact that most recurrences were located outside
of the pelvis (M1 stage), these results indicate the
life-threatening character of continuously rising PSA.
When interpreting the results, certain potential
limitations of the study should be noted, e.g. that retrospective
studies typically provide indications and hypotheses rather than
definitive conclusions.
Unfortunately, risk factors for continuously rising
PSA were difficult to identify. With only 21 events, the
statistical power of this study was limited. For this reason, we
refrained from multivariate analysis. Another weak point was the
limited follow-up time following radiotherapy. The only
statistically significant risk factor was high Gleason score, and
there was also a trend for negative surgical margins. In
exploratory analyses, the highest risk was observed in patients
with a Gleason score of 9 and perineural invasion (80%). However,
this finding should be interpreted with caution as it was derived
from an extremely small subgroup of five patients. In a comparably
small study (n=61 vs. 83 in the present analysis), different
results were obtained (13). In
addition to negative surgical margins, PSA velocity ≥0.8 ng/ml/year
was associated with higher risk of persistent PSA increase,
indicating non-response to salvage radiotherapy. The Gleason score
was not statistically significant. In our study, PSA velocity was
unknown. If patients with delayed PSA relapse following salvage
radiotherapy were to be included, as was typically the case in
previous analyses, the interpretation of results becomes more
complicated. Primary non-response is associated with an absence of
cancer cells in the prostate bed. This could also be termed a
‘staging error’ since current imaging is not able to detect
microscopic cancer deposits. If PSA relapse develops later during
follow-up, reasons including surviving cancer cells in the prostate
bed need to be considered in addition to out-of-field relapse.
Survival may result from geographical miss or a more general,
insufficiently low radiation dose.
Possible ways forward for patients with a high risk
of continuous PSA increase following prostate bed radiotherapy
alone include more effective pre-radiotherapy staging, for example
with PET-CT, which has been demonstrated to impact patient
management in this setting (14–17).
Immediate postoperative radiotherapy could also be helpful
(18–20), since it is able to kill residual
cancer cells as early as possible, thereby preventing metastatic
seeding from the prostate bed during the time interval that elapses
between surgery and salvage radiotherapy. Salvage extended-field
pelvic radiotherapy alone may not be sufficient, since most of our
patients had radiological relapses outside of this region. The
addition of systemic therapy appears to be necessary to address the
issue of distant micrometastases, e.g. endocrine, cytotoxic or
immune therapy (21–25).
The majority of patients with biologically
aggressive tumors with Gleason score 9 were not adequately treated
with prostate bed radiotherapy alone. The predominant pattern of
radiological recurrence was outside of the pelvis. Therefore, the
problem of distant micrometastases has to be addressed.
References
|
1
|
De Meerleer G, Fonteyne V, Meersschout S,
et al: Salvage intensity-modulated radiotherapy for rising PSA
after radical prostatectomy. Radiother Oncol. 89:205–213. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bernard JR Jr, Buskirk SJ, Heckman MG, et
al: Salvage radiotherapy for rising prostate-specific antigen
levels after radical prostatectomy for prostate cancer:
dose-response analysis. Int J Radiat Oncol Biol Phys. 76:735–740.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Trock BJ, Han M, Freedland SJ, et al:
Prostate cancer-specific survival following salvage radiotherapy vs
observation in men with biochemical recurrence after radical
prostatectomy. JAMA. 299:2760–2769. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jereczek-Fossa BA, Zerini D, Vavassori A,
et al: Sooner or later? Outcome analysis of 431 prostate cancer
patients treated with postoperative or salvage radiotherapy. Int J
Radiat Oncol Biol Phys. 74:115–125. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Valicenti RK, Thompson I Jr, Albertsen P,
et al: Adjuvant and salvage radiation therapy after prostatectomy:
American Society for Radiation Oncology/American Urological
Association guidelines. Int J Radiat Oncol Biol Phys. 86:822–888.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shelan M, Abo-Madyan Y, Welzel G, et al:
Dose-escalated salvage radiotherapy after radical prostatectomy in
high risk prostate cancer patients without hormone therapy:
outcome, prognostic factors and late toxicity. Radiat Oncol.
8:2762013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stephenson AJ, Scardino PT, Kattan MW, et
al: Predicting the outcome of salvage radiation therapy for
recurrent prostate cancer after radical prostatectomy. J Clin
Oncol. 25:2035–2041. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Macdonald OK, D'Amico AV, Sadetsky N,
Shrieve DC and Carroll PR: Predicting PSA failure following salvage
radiotherapy for a rising PSA post-prostatectomy: from the CaPSURE
database. Urol Oncol. 26:271–275. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Moreira DM, Jayachandran J, Presti JC Jr,
et al: Validation of a nomogram to predict disease progression
following salvage radiotherapy after radical prostatectomy: results
from the SEARCH database. BJU Int. 104:1452–1456. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lohm G, Lütcke J, Jamil B, et al: Salvage
radiotherapy in patients with prostate cancer and biochemical
relapse after radical prostatectomy: long-term follow-up of a
single-center survey. Strahlenther Onkol. 190:727–731. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Geinitz H, Riegel MG, Thamm R, et al:
Outcome after conformal salvage radiotherapy in patients with
rising prostate-specific antigen levels after radical
prostatectomy. Int J Radiat Oncol Biol Phys. 82:1930–1937. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wiegel T, Lohm G, Bottke D, et al:
Achieving an undetectable PSA after radiotherapy for biochemical
progression after radical prostatectomy is an independent predictor
of biochemical outcome-results of a retrospective study. Int J
Radiat Oncol Biol Phys. 73:1009–1016. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Miyake M, Tanaka N, Asakawa I, et al:
Proposed salvage treatment strategy for biochemical failure after
radical prostatectomy in patients with prostate cancer: a
retrospective study. Radiat Oncol. 9:2082014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ceci F, Herrmann K, Castellucci P, et al:
Impact of (11) C-choline PET/CT on clinical decision making in
recurrent prostate cancer: results from a retrospective two-centre
trial. Eur J Nucl Med Mol Imaging. 41:2222–2231. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
D'Angelillo RM, Sciuto R, Ramella S, et
al: 18F-choline positron emission tomography/computed
tomography-driven high-dose salvage radiation therapy in patients
with biochemical progression after radical prostatectomy:
feasibility study in 60 patients. Int J Radiat Oncol Biol Phys.
90:296–302. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rischke HC, Schäfer AO, Nestle U, et al:
Detection of local recurrent prostate cancer after radical
prostatectomy in terms of salvage radiotherapy using dynamic
contrast enhanced-MRI without endorectal coil. Radiat Oncol.
7:1852012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Beresford MJ, Gillatt D, Benson RJ and
Ajithkumar T: A systematic review of the role of imaging before
salvage radiotherapy for post-prostatectomy biochemical recurrence.
Clin Oncol (R Coll Radiol). 22:46–55. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bolla M, van Poppel H, Collette L, et al:
Postoperative radiotherapy after radical prostatectomy: a
randomised controlled trial (EORTC trial 22911). Lancet.
366:572–578. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Thompson IM Jr, Tangen CM, Paradelo J, et
al: Adjuvant radiotherapy for pathologically advanced prostate
cancer: a randomized clinical trial. JAMA. 296:2329–2335. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wiegel T, Bottke D, Steiner U, et al:
Phase III postoperative adjuvant radiotherapy after radical
prostatectomy compared with radical prostatectomy alone in pT3
prostate cancer with postoperative undetectable prostate-specific
antigen: ARO 96-02/AUO AP 09/95. J Clin Oncol. 27:2924–2930. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Choo R, Danjoux C, Gardner S, et al:
Efficacy of salvage radiotherapy plus 2-year androgen suppression
for postradical prostatectomy patients with PSA relapse. Int J
Radiat Oncol Biol Phys. 75:983–989. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pai HH, Eldridge B, Bishop D, et al: Does
neoadjuvant hormone therapy improve outcome in prostate cancer
patients receiving radiotherapy after radical prostatectomy? Can J
Urol. 16:4541–4552. 2009.PubMed/NCBI
|
|
23
|
Leung CM, Li SC, Chen TW, et al:
Comprehensive microRNA profiling of prostate cancer cells after
ionizing radiation treatment. Oncol Rep. 31:1067–1078.
2014.PubMed/NCBI
|
|
24
|
Guttilla A, Bortolus R, Giannarini G, et
al: Multimodal treatment for high-risk prostate cancer with
high-dose intensity-modulated radiation therapy preceded or not by
radical prostatectomy, concurrent intensified-dose docetaxel and
long-term androgen deprivation therapy: results of a prospective
phase II trial. Radiat Oncol. 9:242014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Grenader T, Plotkin Y, Gips M, Cherny N
and Gabizon A: Diethylstilbestrol for the treatment of patients
with castration-resistant prostate cancer, Retrospective analysis
of a single institution experience. Oncol Rep. 31:428–434.
2014.PubMed/NCBI
|