Introduction
Synovial osteochondromatosis is a benign rare
disease, which is characterized by synovial metaplasia and
hyperplasia, in which cartilaginous nodule shedding of loose bodies
into the synovial cavity is frequently observed (1–4). It's
exact incidence is unknown (5,6). The knee
joint is the most common articulation involved, followed by the
hip, elbow and shoulder. However, the wrist is rarely affected
(7–9).
One retrospective case series reported a prevalence of 7.5% in the
wrist, compared with 74% in the knee (10). Our literature review revealed ~29
cases of synovial osteochondromatosis have been reported in the
wrist. The primary clinical manifestations of synovial
osteochondromatosis are non-specific, including swelling, pain, a
palpable mass, tenderness and restricted movement of the joint,
which may develop slowly over several years (4,11). The
majority of patients affected by synovial osteochondromatosis are
primarily in the third or fifth decade of life (5). Furthermore, the incidence in men is 3–5
times greater than that in women (12). In general, treatment of synovial
osteochondromatosis consists of surgical excision of the diseased
synovium and cartilaginous nodules, which frequently achieves a
satisfactory result (13,14).
Although no comparative studies for the wrist have
been performed, removal of loose bodies and synovectomy of the knee
leads to positive results for function, pain and control of
synovitis in 90% of subjects (15).
However, synovial osteochondromatosis may be locally aggressive
with a tendency to recur, but has no metastatic potential.
Malignant transformation of preexisting primary synovial
osteochondromatosis to synovial chondrosarcoma is recognized to be
a rare event with reports estimating the incidence to be in the
range of 1–7% (6,16). Overall, synovial osteochondromatosis
is a benign disease, and prognosis following removal of the nodules
is reported as excellent.
In order to analyze the clinical, imaging
characteristic and therapeutic modalities of synovial
osteochondromatosis of the wrist, and to prevent orthopedic
surgeons from misdiagnosis that could lead to a delay in treatment,
the relevant literature was reviewed and a rare case of synovial
chondromatosis in the wrist was reported in the present study.
Written informed consent was obtained from the patient for
publication of this study.
Case report
A 33-year-old male patient presented at the First
Affiliated Hospital of Nanchang University (Nanchang, China) on
July 3, 2014, with the symptom of swelling of the left wrist joint
for ~2 years, which had become increasingly painful over the
previous 2 months. There were no systemic symptoms, including
weight loss and night sweats, prior to the patient's
hospitalization, and the patient had not experienced any previous
tumors. The patient was otherwise healthy with a benign medical
history, and had no history of previous surgeries. There was no
history of trauma to the patient's left wrist joint. Physical
examination revealed local tenderness and a soft pliable mass, with
no involvement of the skin and little pain; however, there was no
profound restriction of wrist joint motion. Therefore, the patient
was referred to the Department of Orthopedics (The First Affiliated
Hospital of Nanchang University, Nanchang, China) for additional
investigation of the lump in the left wrist joint on July 5, 2014.
A mass was detected using X-ray imaging (Fig. 1A and B), which revealed a soft-tissue
lump over the volar radial side of the left wrist joint, with no
erosion of the adjacent cortex. Pre-operative blood test results,
including those for tumor markers, were normal. Computed tomography
(CT) imaging (SOMATOM Sensation 16; Siemens AG, Munich, Germany)
revealed a lesion within the soft tissue of the radial side of the
left wrist joint, measuring ~44×31 mm. The articular surface of the
lesion was smooth, with no indication of any ossification or
erosion of the adjacent cortex. No joint effusion was observed,
however, the mass exhibited a low uneven density, accompanied by
punctate or ringed calcification bodies, while the boundary of the
lesion was distinctive (Fig. 1C and
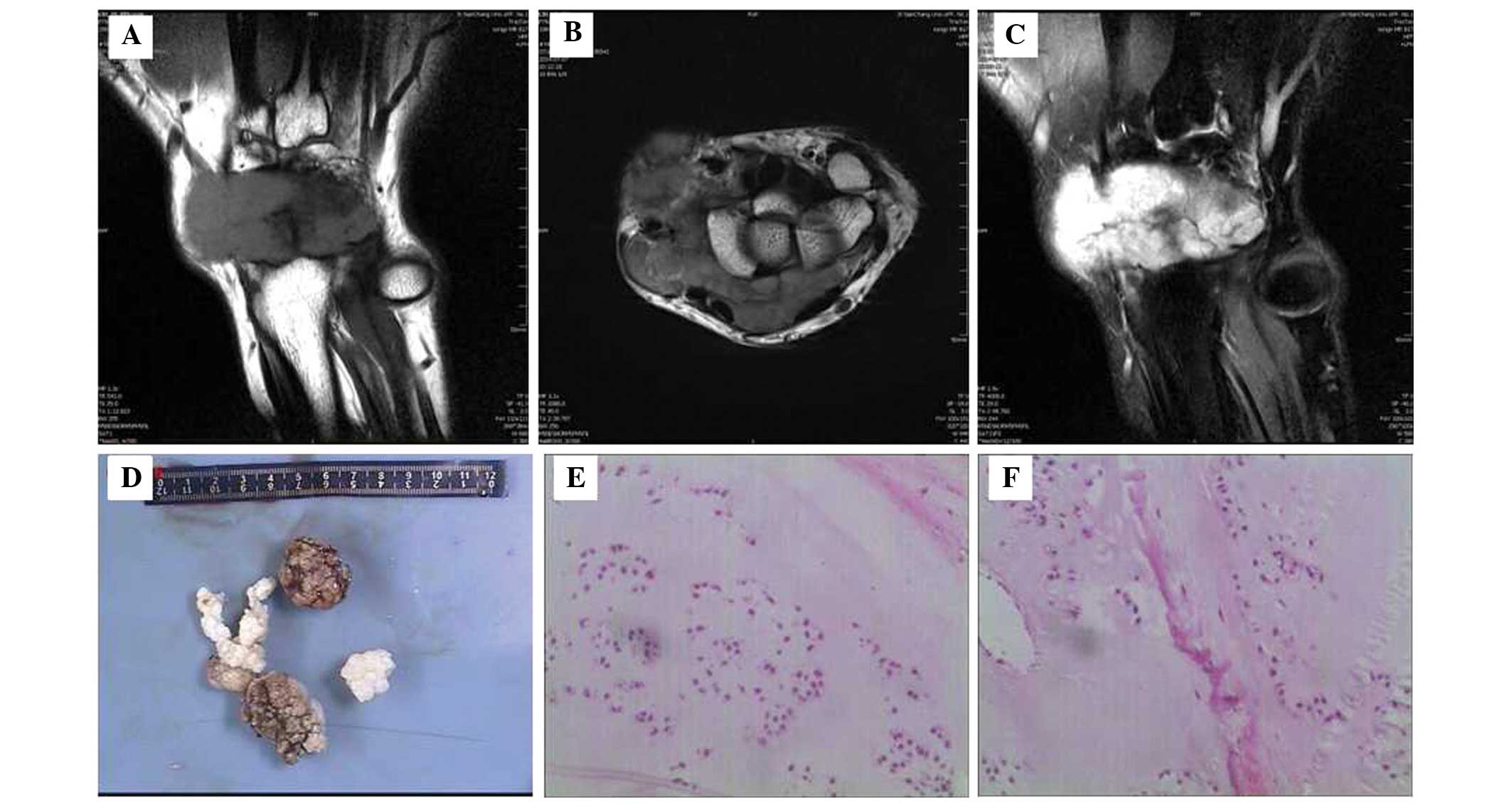
D). Magnetic resonance imaging [MRI; Magnetom Trio, A Tim
System, ultra high field MRI (3.0T); Siemens AG] was subsequently
performed to investigate the lesion. This revealed a mass expanding
into the intra-articular radial side of the joint and around the
synovial membrane. The mass demonstrated long signal intensity on
T1-weighted images (WI) and a reduced intensity on T2WI. Fat
suppression sequences revealed a high signal, which demonstrated a
creeping proliferation and a clear boundary. There were no abnormal
signals over the adjacent bone, however, a small number of joint
effusions were observed (Fig.
2A–C).
As the patient complained of continuously increasing
pain, which was caused by the lesion, surgical joint exploration
and synovial biopsy were recommended. There were no clear signs of
surgical contraindications. Initially, sterile drapes were
routinely draped, exposing the surgical field following successful
brachial plexus anesthesia. The surgery was performed with an
approach that combined a front and rear incision of the left wrist
joint. Subcutaneous tissue, superficial fascia and tendons were
separated layer by layer.
It was observed that the radial artery and radial
vein were wrapped by the lesion, which originated from the wrist.
The lesion was stripped away cautiously and was found to be
milky-white in color, with the appearance of several
cauliflower-like firm cartilaginous nodules, which were located in
the front and back of the wrist joint capsule and partly lined by
synovium. However, the nodules adhered loosely to the joint capsule
and no evidence of erosion over the adjacent bone was detected. The
mass was excised as completely as possible and a histological
examination was performed. The wound was lavaged using a
power-pulsed lavage device (Pulsavac® Plus Wound Debridement System
Component kit; Zimmer Biomet, Warsaw, IN, USA) and a drainage tube
was placed. Finally, each layer of tissue was sutured gradually
following sheer hemostasis. During surgery, the patient's estimated
blood loss was 100 ml and there was no requirement for a blood
transfusion.
Histological examination revealed that the excised
bodies were gray, firm, cartilaginous tissue nodules, ~7.5×5×3 cm
in size (Fig. 2D). Tissue sections
were prepared as follows: Tissue samples were selected and fixed by
immersion in 10% neutral buffered formalin (Macklin Biochemical
Technology Co., Ltd., Shanghai, China) for 8 h. Subsequently, the
samples were decalcified (nitrate decalcifying liquid; Gefan
Biological Technology Co., Ltd., Shanghai, China) for 12 h,
dehydrated using ethanol (Macklin Biochemical Technology Co., Ltd.)
and a dewatering machine (PELORIS II; Leica Microsystems GmbH,
Wetzlar, Germany) and transparentized (xylene; Macklin Biochemical
Technology Co., Ltd.), followed by paraffin embedding (paraffin;
Macklin Biochemical Technology Co., Ltd.). Sections (3 µm thick)
were sliced from the paraffin block using a microtome (RM2235;
Leica Microsystems GmbH), and subsequently deparaffinized (draught
drying cabinet; ZBY 149-83; Shanghai Yuejin Medical Instruments
Co., Ltd, Shanghai, China) and stained with hematoxylin and eosin
(Boster Biological Technology, Pleasanton, CA, USA). Finally, the
sections were dehydrated and hyalinized (hyalin; Macklin
Biochemical Technology Co., Ltd.), followed by mounting with
Permount™ mounting medium (Boster Biological Technology).
Histopathological assessment under light microscopy (Eclipse Ci-E;
Nikon Corp., Tokyo, Japan) revealed small, metaplastic
cartilaginous nodules accompanied by calcifications (Fig. 2E and F). Therefore, the tumor was
diagnosed as synovial osteochondromatosis.
The associated symptoms improved significantly
following excision of the lesion. The patient underwent follow-up
for 1.5 years and no residual or recurrent lesions were observed,
as well as no evidence of malgnancy.
Discussion
Synovial osteochondromatosis of the wrist joint is a
rare benign tumor, characterized by the presence of multiple
cartilaginous nodules within the synovial or tenosynovial membrane
(4,13,17).
Occasionally, the mass may proliferate beyond the joint and into
the adjoining soft tissue. The exact etiology of synovial
osteochondromatosis remains to be elucidated. However, Milgram
(13) divided it into 3 histological
phases based on the maturation of the lesion: i) Active
intrasynovial disease with no appearance of loose bodies; ii) loose
bodies and active synovial disease; and iii) multiple osteochondral
bodies without intrasynovial disease. The present patient was in
the second phase of the disease.
A history of trauma does not increase the
probability of developing synovial osteochondromatosis in the wrist
joint (12). In general, surgical
excision of the neoplasm frequently achieves satisfactory results,
and post-operative follow-up is required in case of recurrence and
potential malignant transformation to chondrosarcoma (1,18–20). Secondary degenerative osteoarthritis
is the primary complication of synovial osteochondromatosis due to
chronic mechanical stimulation and articular cartilage destruction
by loose bodies (20). Due to the low
incidence and non-specific symptoms of synovial
osteochondromatosis, diagnosis of this disease may be difficult,
and increased attention should be given to the differential
diagnosis of wrist tumors or other osteopathies, including
rheumatoid arthritis, secondary synovial osteochondromatosis,
chondrocalcinosis, synovial chondrosarcoma and malignant fibrous
histiocytoma (18). Notably, the
standard method of diagnosis for synovial osteochondromatosis is
tissue biopsy followed by pathological examination. In clinical
practice, imaging studies are frequently suggested to assist with
differentiation between benign and malignant space-occupying
lesions (18,19). However, it must be highly emphasized
that clinicians should fundamentally depend on clinical examination
and imaging during the pre-operative diagnosis of synovial
osteochondromatosis.
The most effective treatment method for synovial
osteochondromatosis is total synovectomy, with removal of loose
cartilaginous nodules, for patients exhibiting constant symptoms
(11,20,21).
Recurrence following resection has been reported and is most likely
due to incomplete excision; therefore, surgeons should ensure a
complete synovectomy is performed (22). In addition, although the rate of
malignant degeneration and recurrence is low, it is useful to
follow up the disease post-operatively.
In general, roentgenographic procedures identify
non-specific results, including the presence of a soft-tissue mass,
an indefinite quantity of scattered calcifications or a radiopaque
tumor. This imaging method relies on calcification or ossification
of cartilaginous bodies in the mass (23). Additional radiographic features,
including bone erosion, occasional osteoarthritis, novel bone
formation and regional osteoporosis have been reported (17,24).
Although the metaplastic process of the synovium is self-limiting,
multiple loose cartilaginous bodies may lead to mechanical damage
of the joint, which may result in early degenerative arthritis
(23). CT and MRI are able to provide
detailed detection of intra-articular calcifications suggestive of
loose bodies.
In conclusion, the current study reported a case of
synovial osteochondromatosis originating from the synovium of the
wrist joint. The study analyzed the clinical, imaging
characteristic and therapeutic modalities of synovial
osteochondromatosis, aiming to allow clinicians to improve their
performance when encountering patients with lesions of the wrist.
As a result of achieving a differential diagnosis of synovial
osteochondromatosis, which allows a definite pre-operative
diagnosis, a successful synovectomy may be achieved, assisting with
improvement of the pain and swelling in symptomatic patients.
Acknowledgements
The present study was supported by Gan-Po Talents
Project 555 of Jiangxi Province and The Spark Program of the Health
Department of Jiangxi Province (grant no. 20116007).
References
|
1
|
Wittkop B, Davies AM and Mangham DC:
Primary synovial chondromatosis and synovial chondrosarcoma. Eur
Radiol. 12:2112–2119. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
McLennan MK and Margolis M: Radiology
rounds. Synovial osteochondromatosis. Can Fam Physician.
40:13981994.PubMed/NCBI
|
|
3
|
Wong SH, Salama S and Thoma A: Synovial
chondromatosis of the hand: Three case reports and literature
review. Can J Plast Surg. 11:47–52. 2003.PubMed/NCBI
|
|
4
|
McInnes CW and Goetz TJ: Management of
synovial osteochondromatosis of the distal radioulnar joint with
imaging features consistent with malignancy. Case Rep Orthop.
2013:5896312013.PubMed/NCBI
|
|
5
|
Vinaixa Reverté MM, Singh R, Monyart JM,
Llado GD, Dominguez MP, Feliu EC, Vilardaga Nardi J and Palou EC:
Wrist synovial chondromatosis: Case report and literature review.
Hand Surg. 17:233–238. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Evans S, Boffano M, Chaudhry S, Jeys L and
Grimer R: Synovial chondrosarcoma arising in synovial
chondromatosis. Sarcoma. 2014:6479392014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Roulot E and Le Viet D: Primary synovial
osteochondromatosis of the hand and wrist. Report of a series of 21
cases and literature review. Rev Rhum Engl Ed. 66:256–266.
1999.PubMed/NCBI
|
|
8
|
Llauger J, Palmer J, Rosón N, Bagué S,
Camins A and Cremades R: Nonseptic monoarthritis: Imaging features
with clinical and histopathologic correlation. Radiographics.
20(Suppl): S263–S278. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Boles CA and Ward WG Sr: Loose fragments
and other debris: Miscellaneous synovial and marrow disorders. Magn
Reson Imaging Clin N Am. 8:371–390. 2000.PubMed/NCBI
|
|
10
|
Maurice H, Crone M and Watt I: Synovial
chondromatosis. J Bone Joint Surg Br. 70:807–811. 1988.PubMed/NCBI
|
|
11
|
Chillemi C, Marinelli M and de Cupis V:
Primary synovial chondromatosis of the shoulder: Clinical,
arthroscopic and histopathological aspects. Knee Surg Sport
Traumatol Arthrosc. 13:483–488. 2005. View Article : Google Scholar
|
|
12
|
Loonen MP and Schuurman AH: Recurrent
synovial chondromatosis of the wrist: Case report and literature
review. Acta Orthop Belg. 71:230–235. 2005.PubMed/NCBI
|
|
13
|
Milgram JW: Synovial osteochondromatosis:
A histopathological study of thirty cases. J Bone Joint Surg Am.
59:792–801. 1977.PubMed/NCBI
|
|
14
|
Sim FH, Dahlin DC and Ivins JC:
Extra-articular synovial chondromatosis. J Bone Joint Surg Am.
59:492–495. 1977.PubMed/NCBI
|
|
15
|
Ogilvie-Harris DJ and Weisleder L:
Arthroscopic synovectomy of the knee: Is it helpful? Arthroscopy.
11:91–95. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Murphey MD, Vidal JA, Fanburg-Smith JC and
Gajewski DA: Imaging of synovial chondromatosis with
radiologic-pathologic correlation. Radiographics. 27:1465–14682007.
View Article : Google Scholar
|
|
17
|
Friedman B, Caspi I, Nerubay J, Huszar M,
Ganel A and Horoszowski H: Synovial chondromatosis of the hip
joint. Orthop Rev. 17:994–998. 1988.PubMed/NCBI
|
|
18
|
McKenzie G, Raby N and Ritchie D: A
pictorial review of primary synovial osteochondromatosis. Eur
Radiol. 18:2662–2669. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hallam P, Ashwood N, Cobb J, Fazal A and
Heatley W: Malignant transformation in synovial chondromatosis of
the knee? Knee. 8:239–242. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
McFarland EG and Neira CA: Synovial
chondromatosis of the shoulder associated with osteoarthritis:
Conservative treatment in two cases and review of the literature.
Am J Orthop (Belle Mead NJ). 29:785–787. 2000.PubMed/NCBI
|
|
21
|
Park JH, Noh HK, Bada LP, Wang JH and Park
JW: Arthroscopic treatment for synovial chondromatosis of the
subacromial bursa: A case report. Knee Surg Sports Traumatol
Arthrosc. 15:1258–1260. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Floyd W III and Troum S: Benign
cartilaginous lesions of the upper extremity. Hand Clin.
11:119–132. 1995.PubMed/NCBI
|
|
23
|
Crotty JM, Monu JU and Pope TL Jr:
Synovial osteochondromatosis. Radiol Clin North Am. 34:327–342.
1996.PubMed/NCBI
|
|
24
|
Norman A and Steiner GC: Bone erosion in
synovial chondromatosis. Radiology. 161:749–752. 1986. View Article : Google Scholar : PubMed/NCBI
|