Introduction
Metastases are the major cause of cancer-associated
death in cancer patients, and are the predominant sites to which
metastasis occurs (1,2,3). The
primary tumors that most frequently metastasize to the bones
include breast, prostate and lung cancer (4–6). Pain is
the most common symptom experienced by patients, among all
potential complications associated with bone metastasis, and
results in a significant deterioration in quality of life (QoL)
(1,4,5,7,8). Current
treatment objectives are designed to decrease the tumor burden in
patients with overt bone metastases, maximize pain control and
reduce the incidence of skeletal-related events (5). Pain management/analgesia, surgery,
radiation therapy (RT), systemic therapy, or a combination of these
techniques are current strategies for the management of skeletal
metastasis (9). However, the
long-term results of these treatments require improvement (10,11).
Thermoablation is a category of non-surgical
approaches used to treat otherwise unresectable tumors, and the
techniques it includes utilize a variety of power sources.
Furthermore, an array of delivery methods for ablation exist,
including laser ablation, radiofrequency ablation (RFA),
cryoablation (CA), microwave ablation and high intensity focused
ultrasound (HIFU) (12–14). These techniques have proven to be
useful therapeutic options for bone tumor management, in addition
to the treatment of metastatic liver and malignant primary tumors
for which they were originally developed (15–18).
Recent studies have demonstrated that the association of RT with
RFA is well tolerated, and has a satisfactory profile of adverse
side effects (19,20). The aim of the present study was to
investigate whether RFA and CA improve the clinical management of
osteolytic solitary painful bone metastases, selecting the study
population retrospectively by propensity analysis.
Materials and methods
Patient selection
In the present study, patients >18 years, with
painful solitary osteolytic bone metastases, confirmed by
radiological and histological investigations were retrospectively
selected from a pool of subjects who underwent CA or RFA between
September 2011 and September 2014. Magnetic resonance imaging (MRI)
examination, computed tomography (CT), and nuclear isotope
(technetium 99) bone scans were performed within the 4 weeks prior
to the procedures. Eligibility criteria included: (i) A pain score
of ≥5 on the validated visual analog scale (VAS) over the previous
24 hours (or a score of <5 with the use of narcotic
medications); (ii) pain localized to the site of the bone
metastases; (iii) life expectancy >3 months, and (iv), a
Karnofsky performance status (KPS) score >70. Exclusion criteria
were: (i) The area of pain had been previously treated with RT,
palliative surgery or interventional radiological approaches; (ii)
radiographic evidence of spinal cord or cauda-equina compression;
(iii) lesions positioned within 0.5 cm of a critical site, such as
the spinal cord, brain, aorta, inferior vena cava, bowel, or
bladder; (iv) abnormal fracture of the treatment site. Written
informed consent was obtained from all patients. The present
retrospective study was approved by the San Salvatore Hospital
institutional Ethical Committee.
Cryoablation
Percutaneous CA was carried out under conscious
sedation with an argon-based cryotherapy system (SeedNet® Gold
Cryoablation System, Galil Medical Ltd., Yokneam, Israel).
Following sterile preparation, one or more cryoprobes (IceRod®,
Galil Medical Ltd.) were introduced into the target lesion with CT
guidance by experienced radiologists. The cryoprobes were
introduced in a parallel arrangement ~2 cm apart. For larger
lesions, a cluster of cryoprobes was placed within 1 cm of the
tumor margin to provide adequate coverage of the outer border of
the target lesion. Cryoprobe positioning was confirmed by CT
imaging. Rapid freezing of the target lesion (−100 °C within a few
seconds) was performed, and two 15 min freezes separated by a 10
min thaw were used at each cryoprobe position.
Radiofrequency ablation
Percutaneous RFA was performed under conscious
sedation. Following sterile preparation, a LeVeen™ needle electrode
(Boston Scientific Corp., Natick, MA, USA) was introduced under CT
guidance into the metastases. After unfolding the electrode tines
into the metastases, the needle was connected to a radiofrequency
generator (RF 3000®; Boston Scientific Corp.). The procedure was
conducted according to the protocols supplied by the equipment
manufacturers. Briefly, the developed energy was increased 10 W
every 3 min up to 90 W, until tissue impedance increased and
further current flow was prevented (roll-off). A target
intratumoural temperature higher than 60 °C was considered as an
indicator of adequate thermocoagulation. A single ablation was
performed for lesions measuring <3 cm in the longest diameter.
For larger lesions (3–7 cm) a cluster RFA electrode technique was
used (3 needles spaced 5 mm apart). At the end of each CA or RFA, a
CT was performed to ensure that the extent of ablation was confined
to the target tissue and that there was no substantial damage in
the tissue surrounding the target. After all combined procedures,
patients were observed for 2 h in the recovery room and were then
admitted to the hospital for a minimum of 24 h.
Patient assessment
A full physical examination was performed and data
on direct and indirect changes in pain levels were assessed by VAS
and a medication level questionnaire. QoL was assessed with a
single question from the McGill Quality of Life Questionnaire
(MQOL) (21). The strongest evidence
of validity comes from comparison with the single-item quality of
life measure (21).
Complications of the procedures
Complications related to ablative approaches were
rated as major or minor according to the guidelines of the Society
of Interventional Radiology (22).
Study endpoints and response
criteria
The primary endpoints were to assess the changes
from baseline (pre-CA or RFA) to week 12 in the rate of (1) complete (CR) and (2) partial (PR) responses (23). The secondary endpoints were to assess
the changes from baseline (pre-CA or RFA) to week 12 in the rate
(1) of subjects requiring opioid
analgesic use and (2) in
self-experienced QoL.
Statistical analysis
The data analyzed in the present study were derived
from a population-based retrospective study. In order to reduce
treatment selection bias and realistically determine the treatment
effects, a case control-matched propensity analysis was performed.
Multivariate logistic regression was used to calculate the
predicted probability of the dependent variables, as well as the
propensity score for all observations in the dataset. The dependent
variables included in the multivariate analysis were age, KPS,
primary tumor number, metastasis location, VAS scale, and the QoL
prior to the procedures. A 1:1 matched analysis was performed,
where one subject treated by CA was matched to one subject treated
by RFA. Continuous variables not normally distributed (Shapiro-Wilk
test) were presented as medians and 95% confidence intervals (95%
CI). The Mann-Whitney U test was used to evaluate the difference
between two groups and the Kruskal-Wallis test was used to evaluate
the difference between more than two tests. If the Kruskal-Wallis
test was statistically significant, a pairwise comparison of
subgroups was performed according to Conover. Dichotomous variables
were summarized by absolute and/or relative frequencies. The
Chi-squared test or Fisher's exact test was used to evaluate the
difference between two groups. For multiple comparisons, the alpha
value threshold was adjusted by using Bonferroni correction. For
matched pairwise multiple comparisons, dichotomous variables were
compared with Cochran's Q test. For matched pair-wise comparisons
McNemar's test was used. All tests were two-sided except where
specified, and were determined by Monte Carlo significance. An
alpha value threshold of 0.05 was used. All statistical analyses
were performed using the SPSS® statistical analysis software
package, version 10.0 (SPSS, Inc., Chicago, IL, USA).
Results
Table I lists the
clinical and demographic characteristics of treated patients
stratified according to propensity score and treatment received. At
12 weeks following treatment, all patients were analyzed, as the
selected patients were long-term survivors of a solitary bone
lesion. The VAS scale before treatments was 7 (95% CI, 5–7) in the
group treated by RFA and 7.5 (95% CI, 5–67.6) in the group treated
by CA. The mean tumor size was 4 cm in both groups. Primary tumor
lesions were located in lung, prostate, kidney, colorectum and
breast, and the metastatic sites were pelvis, sacrum, rib,
vertebrae, humerus and femur (Table
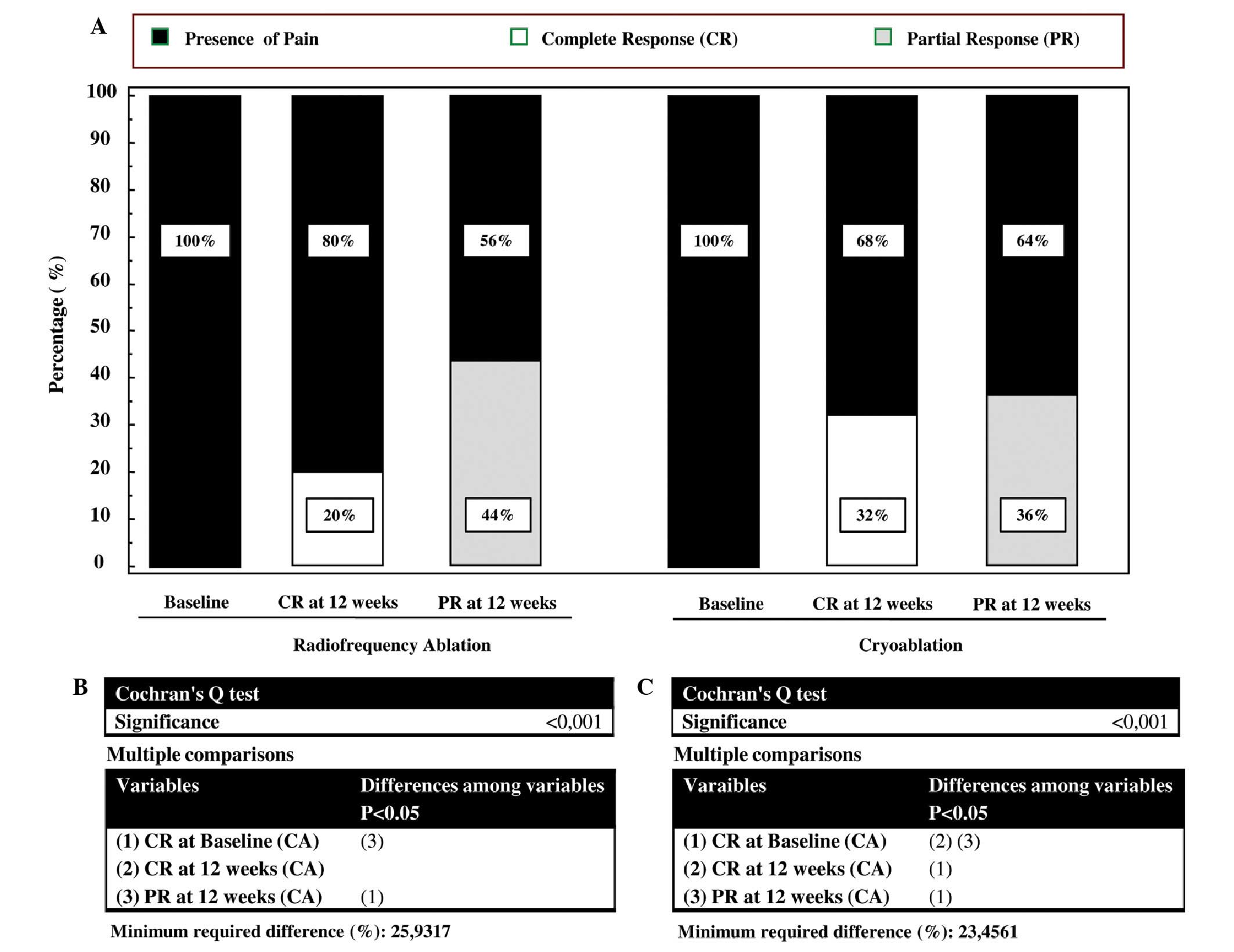
I). Eight out of 25 subjects treated by CA (32%) experienced a
CR at 12 weeks vs. 5 out of 25 patients treated by RFA (20%)
(Fig. 1). Interestingly, when within
analysis was performed by the Cochran's Q test, the rate of CR in
the CA group significantly increased with respect to the baseline
(Fig. 1C). By contrast, this
parameter did not significantly increase with respect to baseline
in the RFA group (Fig. 1B). Nine out
of 25 subjects treated by CA (36%) experienced a PR at 12 weeks vs.
11 out of 25 of patients treated by RFA (44%) (Fig. 1). In both groups there was a
significant change in the PR with respect to baseline (Fig. 1 C and D). The number of subjects with
stable or progressive pain was 8 out 25 (32%) in the CA group and 9
out of 25 (36%) in the RFA group. Three out of 8 (37.5%) patients
in the RFA group and 2 out of 9 (22%) patients in the CA group with
stable or progressive pain at 12 weeks from treatments, experienced
a 3-point fall in pain within the first 2 weeks following the
procedure. These patients had recurrent pain of intensity equal to
or greater than the worst pain experienced prior to CA or RFA
treatments between the 6th and 10th of follow-up, with no
difference in the temporal trend between the two groups. All
patients received oral narcotic analgesia over the month prior to
treatment with CA or RFA (Table I).
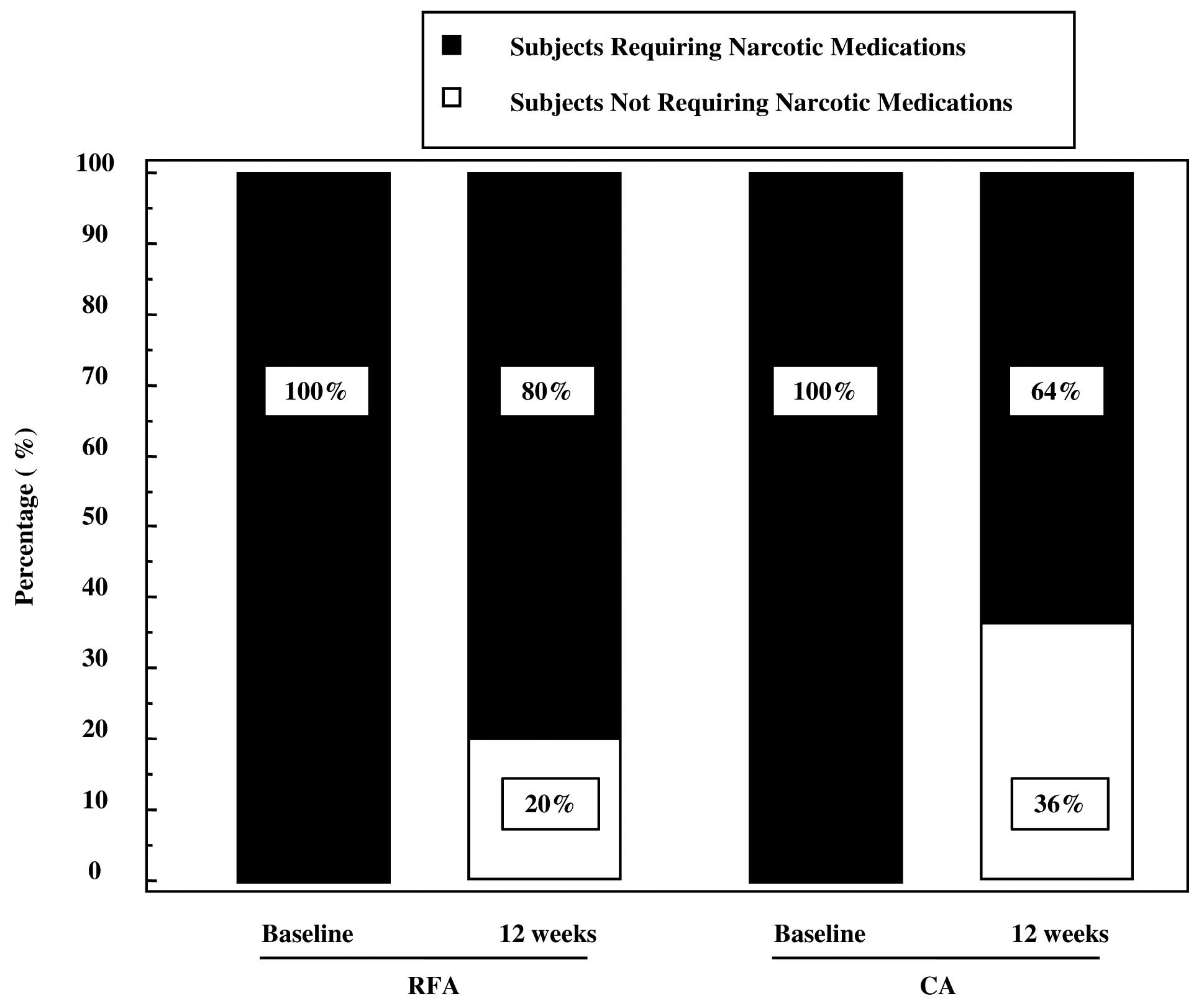
At 12 weeks, 20% of patients (5/25) in the RFA group and 36% of
patients (9/25) in the CA group did not require narcotic medication
(Fig. 2). For data on the complete
and partial response, the McNemar test indicated that the reduction
in narcotic medication requirements was significantly reduced in
the CA group (P=0.0039), whereas in the RFA group, there was a
trend toward a lower rate of narcotic used that did not reach
statistical significance (P=0.062). The higher rate of CR and PR
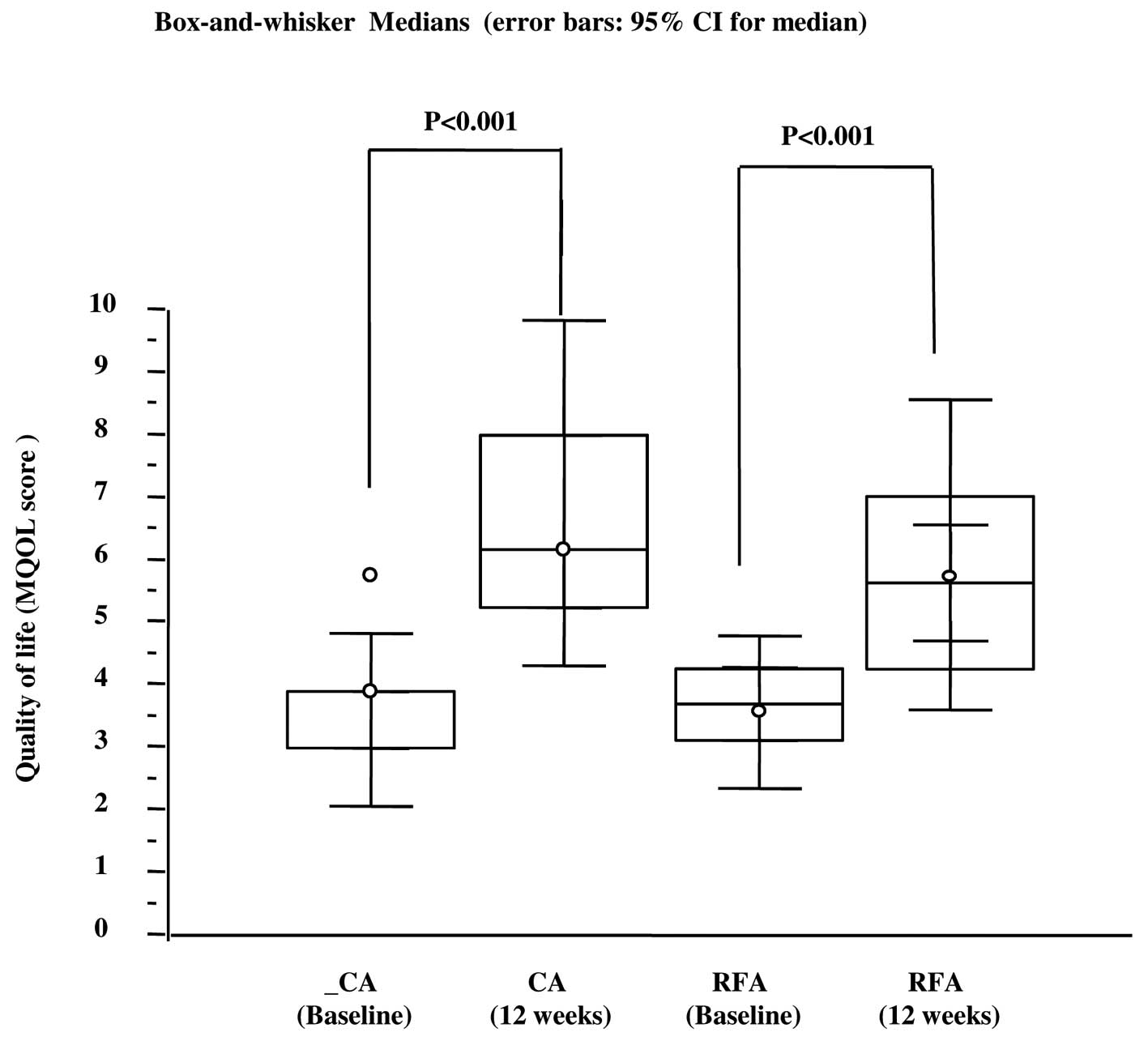
observed in patients treated with CA or RFA correlated with an
improved self-rated QoL (Fig. 3). At
12 weeks, patients treated by CA or RFA reported a significant
improvement in self-rated QoL. In the group treated by CA, the MQOL
score increased from 3.9 [interquartile range (IRQ) 3–4] to 6.1
(IRQ 5.2–8) whereas in the group treated by RFA the score increased
from 3.6 (IRQ 3.1–4.2) to 5.6 (IRQ 4.3–7) (Fig. 3). Overall, patients tolerated the CA
and RFA treatment. Two transient nerve injuries occurred, one in
the RFA group and one in the CA group, neither of which prolonged
the length of hospitalization. These injuries appeared 6 and 11
days after the CA and RFA treatments, respectively, with
improvement within 10 days following administration of a systemic
steroid.
 | Table I.Clinical characteristics according to
propensity score |
Table I.
Clinical characteristics according to
propensity score
| Characteristics | RFA (n=25) | CA (n=25) | P-value |
|---|
| Age, years
(range) |
66 (59–70) |
67.5
(64.4 to 70.6) | 0.678a |
| VAS scale
(range) | 7
(5–7) | 7.5
(5–7.6) | 0.822a |
| Sex, no. (%) |
|
|
|
| Male | 11 (44) | 12 (48) | 1.0c |
|
Female | 14 (56) | 13 (52) |
|
| KPS, no. (%) |
|
|
|
|
91–100 | 10 (40) | 11 (44) | 1.0b |
|
70–89 | 15 (60) | 14 (56) |
|
| Tumor size, cm |
4 (4–5) |
4
(3.4–6) | 0.456a |
| Primary tumors, no.
(%) |
|
|
|
| Lung
cancer | 7
(28) | 7 (28) |
|
| Prostate
cancer | 2 (8) | 3 (12) |
|
| Renal
cancer | 3
(12) | 4 (16) | 0.79b |
|
Colorectal cancer | 4
(16) | 2 (8) |
|
| Breast
cancer | 14 (56) | 9 (36) |
|
| Metastasis location,
no. (%) |
|
|
|
|
Pelvis | 10 (40) | 8 (32) |
|
|
Sacrum | 6
(24) | 7 (28) |
|
| Rib | 2 (8) | 2 (8) | 0.99b |
|
Vertebrae | 3
(12) | 4 (16) |
|
|
Humerus | 2 (8) | 2 (8) |
|
|
Femur | 2 (8) | 2 (8) |
|
| Medical systemic
treatments, no. (%)d |
|
|
|
|
Bisphosphonates | 5
(20) | 8 (32) | 0.52c |
| Narcotic
analgesics | 25
(100) | 25 (100) | 1.0b |
|
Hormonal therapy | 9
(36) | 8 (32) | 1.0c |
|
Chemotherapy | 18 (72) | 15 (60) | 0.55b |
|
Immunotherapy | 2 (8) | 4 (12) | 0.67c |
Discussion
Interventional radiologists have developed a number
of ablative techniques for the management of a range of different
clinical presentations, including bone metastatic disease, with
outstanding results in terms of their efficacy. A relatively
limited number of studies have investigated the RFA in the
management of metastatic bone lesions. In a previous study, RFA
produced a significant reduction in pain, and a significant
improvement in the relief felt and in mood, when assessed at one
and three months following treatment (16). Another feasibility study confirmed the
analgesic efficacy of RFA in absence of serious complication
(15). A multicentre trial conducted
on 43 patients with painful, refractory, pelvic or sacral lesions
evaluated RFA (13). At 4, 12 and 24
weeks following RFA, 95% of treated patients reported pain relief
(a fall of at least two points in the most intense pain) with a
reduction in the provision of analgesics observed at 8 and 12
weeks. Complications included cutaneous burn, transitory faecal and
urinary incontinence following treatment of a sacral location, and
an acetabular fracture. CA is a common ablative technique that
creates an ‘ice-ball’ deep in bone by using miniaturized argon-gas
devices. This method is associated with reduced peri- and
post-procedural pain. Recently Callstrom et al (24,25)
performed clinical trials in which percutaneous CA was used for the
palliation of painful metastatic lesions, and the results
demonstrated that CA was safe and effective at reducing the pain
associated with metastatic lesions. To date, the precise mechanisms
through which CA followed by RT can relieve symptomatic pain
remains to be elucidated fully. Pain experienced by patients
suffering from bone metastases may have several pathophysiological
mechanisms. These include: (i) Microfractures by direct metastatic
bone invasion; (ii) periosteum distortion resulting from increased
pressure on the endosteum; (iii) nerve-root compression or muscle
spasm; and (iv) release of chemical mediators involved in the
conduction of nociceptive signals towards the central nervous
system (2,3). Reduced cancer cell burden within bone
tissue is associated with endosteal pressure reduction. The release
and modulation of pain-related chemical mediators with combination
treatment may significantly affect the perception of pain
intensity.
The current study performed a comparative analysis
of the effects that CA or RFA (two well-known interventional
ablative approaches) have in relieving cancer pain related to bone
metastasis. To the best of our knowledge, this is the first report
that analyzes the clinical performances of both RFA and CA in
patients with bone metastatic lesions. Of note, the response
criteria were defined according to the endpoint criteria of the
International Bone Metastases Working Party guidelines on
palliative radiotherapy endpoints for future clinical trials. Thus,
the results of the present study are comparable with the literature
that used the same criteria. Furthermore, the response criteria
included changes in narcotic medication use and self-rated QoL
data. Our retrospective study design was based on estimates of
propensity scores, which can facilitate the generation of unbiased
treatment effect estimates. This powerful statistical approach was
coupled with the use of a pre- and post-test experimental design.
This experimental design is an attractive model for the assessment
of clinical efficacy before and following a treatment, as the
comparisons were made ‘within subjects’ rather than ‘between
subjects’. An important consequence of this experimental strategy
is that the study power is greatly improved compared to other
research designs.
The present study demonstrated that CA significantly
improved both CR and PR with respect to baseline at 12 weeks
following ablation. By contrast, only PR significantly improved
with respect to baseline following RFA treatment. These data were
in line with the improvement of self-rated QoL observed in patients
treated by CA or by RFA. When self-rated QoL was assessed from
baseline to 12 weeks, the patients treated by the two ablative
techniques experienced improved QoL, and this difference was
statistically significant. These data are also paralleled with the
results demonstrating that 20% of subjects treated by RFA and 32%
of patients treated by CA reported no opioid analgesic use at 12
weeks. Interestingly, in terms of medical adjunctive treatment, all
subjects took narcotic medications prior to treatment. The data
concerning the percentage of patients who did not use analgesic
medication are in agreement with a study by Callstrom et al
(24), who reported that 4 of 19
studied patients were not administered opioid analgesic following
CA. Notably, and in agreement with literature, the rate of
complications was 4% following both treatments.
The present study has several limitations, the major
ones being the non-randomized study design and limited sample size.
Large, randomized controlled clinical trials have provided strong
evidence for the efficacy of therapeutic procedures or treatments.
Any bias in these studies has been controlled by using a strategy
based on propensity score analysis, which can generate groups of
patients, randomized post-hoc for important clinical
characteristics. The results of the present study have fewer
methodological biases from using comparative analysis by
propensity-matched pairs, rather than other common statistical
methods.
In conclusion, the results of the present study
suggest for the first time that CA, in contrast to RFA,
significantly improves the rate of CR and decreases the requirement
of narcotic medications. Both CA and RFA improve PR and the
self-rated QoL of patients following the treatments. However, our
data should be considered as preliminary and to serve as a
framework around which to design future trials.
References
|
1
|
Suva LJ, Washam C, Nicholas RW and Griffin
RJ: Bone metastasis: Mechanisms and therapeutic opportunities. Nat
Rev Endocrinol. 7:208–218. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Roodman GD: Mechanisms of bone metastasis.
N Engl J Med. 350:1655–1664. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Suva LJ, Griffin RJ and Makhoul I:
Mechanisms of bone metastases of breast cancer. Endocr Relat
Cancer. 16:703–713. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Coleman RE: Clinical features of
metastatic bone disease and risk of skeletal morbidity. Clin Cancer
Res. 12:6243s–6249s. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Coleman RE: Metastatic bone disease:
Clinical features, pathophysiology and treatment strategies. Cancer
Treat Rev. 27:165–176. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Harvey HA and Cream LV: Biology of bone
metastases: Causes and consequences. Clin Breast Cancer. 7(Suppl
1): S7–S13. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Smith HS: Painful osseous metastases. Pain
Physician. 14:E373–E403. 2011.PubMed/NCBI
|
|
8
|
Tharmalingam S, Chow E, Harris K, Hird A
and Sinclair E: Quality of life measurement in bone metastases: A
literature review. J Pain Res. 1:49–58. 2008.PubMed/NCBI
|
|
9
|
Yu HH, Tsai YY and Hoffe SE: Overview of
diagnosis and management of metastatic disease to bone. Cancer
Control. 19:84–91. 2012.PubMed/NCBI
|
|
10
|
Lutz S, Berk L, Chang E, Chow E, Hahn C,
Hoskin P, Howell D, Konski A, Kachnic L, Lo S, et al: American
Society for Radiation Oncology (ASTRO). Palliative radiotherapy for
bone metastases: An ASTRO evidence-based guideline. Int J Radiat
Oncol Biol Phys. 79:965–76. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Andrade RS, Proctor JW, Slack R, Marlowe
U, Ashby KR and Schenken LL: A simple and effective daily pain
management method for patients receiving radiation therapy for
painful bone metastases. Int J Radiat Oncol Biol Phys. 78:855–859.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Widmann G, Bodner G and Bale R: Tumour
ablation: Technical aspects. Cancer Imaging. 9:63–67. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Goetz MP, Callstrom MR, Charboneau JW,
Farrell MA, Maus TP, Welch TJ, Wong GY, Sloan JA, Novotny PJ,
Petersen IA, et al: Percutaneous image-guided radiofrequency
ablation of painful metastases involving bone: A multicenter study.
J Clin Oncol. 22:300–306. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Silverman SG, Tuncali K, Adams DF,
vanSonnenberg E, Zou KH, Kacher DF, Morrison PR and Jolesz FA: MR
imaging-guided percutaneous cryotherapy of liver tumors: Initial
experience. Radiology. 217:657–664. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Callstrom MR, Charboneau JW, Goetz MP,
Rubin J, Wong GY, Sloan JA, Novotny PJ, Lewis BD, Welch TJ, Farrell
MA, et al: Painful metastases involving bone: Feasibility of
percutaneous CT- and US-guided radio-frequency ablation. Radiology.
224:87–97. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dupuy DE, Liu D, Hartfeil D, Hanna L,
Blume JD, Ahrar K, Lopez R, Safran H and DiPetrillo T: Percutaneous
radiofrequency ablation of painful osseous metastases: A
multicenter American College of Radiology Imaging Network trial.
Cancer. 116:989–997. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rosenthal D and Callstrom MR: Critical
review and state of the art in interventional oncology: Benign and
metastatic disease involving bone. Radiology. 262:765–80. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Grieco CA, Simon CJ, Mayo-Smith WW,
Dipetrillo TA, Ready NE and Dupuy DE: Image-guided percutaneous
thermal ablation for the palliative treatment of chest wall masses.
Am J Clin Oncol. 30:361–367. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Di Staso M, Zugaro L, Gravina GL, Bonfili
P, Marampon F, Di Nicola L, Conchiglia A, Ventura L, Franzese P,
Gallucci M, et al: A feasibility study of percutaneous
Radiofrequency Ablation followed by Radiotherapy in the management
of painful osteolytic bone metastases. Eur Radiol. 21:2004–2010.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Di Staso M, Zugaro L, Gravina GL, Bonfili
P, Marampon F, Di Nicola L, Conchiglia A, Franzese P, Gallucci M,
Masciocchi C, et al: Can radiotherapy be combined with
radiofrequency ablation in the management of symptomatic osteolytic
skeletal metastasis? Clin Oncol (R Coll Radiol). 23:65–66. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cohen SR, Mount BM, Strobel MG and Bui F:
The McGill Quality of Life Questionnaire: A measure of quality of
life appropriate for people with advanced disease. A preliminary
study of validity and acceptability. Palliat Med. 9:207–219. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sacks D, McClenny TE, Cardella JF and
Lewis CA: Society of Interventional Radiology clinical practice
guidelines. J Vasc Interv Radiol. 14:S199–S202. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chow E, Wu JS, Hoskin P, Coia LR, Bentzen
SM and Blitzer PH: International consensus on palliative
radiotherapy endpoints for future clinical trials in bone
metastases. Radiother Oncol. 64:275–280. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Callstrom MR, Dupuy DE, Solomon SB, Beres
RA, Littrup PJ, Davis KW, Paz-Fumagalli R, Hoffman C, Atwell TD,
Charboneau JW, et al: Percutaneous image-guided cryoablation of
painful metastases involving bone: Multicenter trial. Cancer.
119:1033–1041. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Callstrom MR, Atwell TD, Charboneau JW,
Farrell MA, Goetz MP, Rubin J, Sloan JA, Novotny PJ, Welch TJ, Maus
TP, et al: Painful metastases involving bone: Percutaneous
image-guided cryoablation-prospective trial interim analysis.
Radiology. 241:572–580. 2006. View Article : Google Scholar : PubMed/NCBI
|