Introduction
LIM domain only protein (LMO)2 belongs to the LMO
family of transcription factors that contain zinc binding
finger-like motifs, termed LIM domains, which are required in
protein-protein interactions (1).
LMO2, also termed rhombotin-like 1, is a member of a multigene
family that is extremely well-conserved (2). LMO2 encodes a cysteine-rich LIM domain
containing transcription factor, which has been demonstrated to be
required for complete hematopoiesis in mice (3), and has also been identified in key
events in erythropoiesis, angiogenesis and embryogenesis (4,5). LMO2 is
expressed in a number of tissues during fetal life, and its
expression in hematopoietic cells is tightly regulated and varies
at different stages of maturation. In normal B cell differentiation
and maturation, the majority of LMO2 is expressed in the bone
marrow during early lymphopoiesis and in the germinal centers (GC)
of secondary lymphoid organs (6).
In lymphoid and myeloid leukemias there is a
deregulated expression of LMO2 (7–9), and LMO2
is expressed in ~9% of pediatric patients with T-cell acute
lymphoblastic leukemia (T-ALL) (10).
LMO2 activation is a result of chromosomal translocations and
cryptic deletions in the LMO2 negative regulatory domain (11,12).
Previously, it has been demonstrated that LMO2 was insertionally
mutated by retroviral gene therapy vectors in X-linked severe
combined immunodeficiency (SCID-X1) and Wiskott-Aldrich syndrome
(13–15). Notably, transgenic mouse models
revealed that an ectopic expression of LMO2 in T cells leads to the
development of a leukemogenic lesion (16). Overall, these previous studies
indicate that LMO2 may have a role in leukemogenesis.
LMO2 expression has been observed in certain
malignancies, including a subset of acute myeloid leukemia (AML)
(17), and notably, LMO2 protein
expression has been demonstrated to have an effect on the survival
time of patients with chronic myeloid leukemia (CML) treated with
imatinib mesylate (18). In addition,
LMO2 has been suggested as a novel predictive marker for an
improved prognosis in patients with pancreatic cancer (19). It was also clinically relevant in
patients with diffuse large B-cell lymphoma (DLBCL), since its
level of expression was a predictor of patient survival time,
possibly since it identified cases of DLBCL with a germinal-center
cell origin (20). Previously, it was
reported that LMO2 was expressed in a significant proportion of
patients with B-cell acute lymphoblastic leukemia (B-ALL), but was
not prognostic in acute lymphoid leukemia (21). However, a separate study revealed that
LMO2 expression was associated with an improved overall survival
time in patients with normal karyotype B-ALL (22). Therefore, the aim of the present study
was to evaluate the prognostic role of LMO2 in adult patients with
breakpoint cluster region/Abelson murine leukemia viral oncogene
homolog 1 (BCR/ABL) negative B-ALL.
Patients and methods
Patients
LMO2 expression was assessed in a cohort of 85 adult
patients, which consisted of 48 men and 37 women, with BCR/ABL
negative B-ALL. The patients were enrolled between December 2010
and August 2013 at the Oncology Center of Mansoura University
Hospital (Mansoura, Egypt). The present study was approved by the
Institutional Review Board at the Mansoura University Hospital
(approval number, H-01-R-009). Written informed consent was
obtained from each patient. The age of the patients ranged between
19 and 62 years with a median age of 50 years. In total, 32 control
individuals, which consisted of 18 men and 14 women (median age, 49
years; age range, 19–60 years) that were healthy blood donors and
had normal laboratory results (white blood cells, normal range
4.5–11.0 cells/cmm; red blood cells, normal range 3.8–5.8
cells/ccm; hemoglobin, normal range 13–18 gm/dl; platelets, normal
range 150–440 cells/cmm) and no history of malignancies were
selected to closely match the age and gender of the patients with
BCR/ABL negative B-ALL.
A diagnosis of B-ALL was based on morphological,
cytogenetic and immunophenotypic criteria (23–25). Blood
samples of the patients were collected prior to treatment. Briefly,
treatment consisted of 6 weeks of induction, 2 weeks of
consolidation and 120 weeks of continuation therapy. Induction
therapy consisted of vincristine (VCR; 1.5 mg/m2),
daunomycin (45 mg/m2), asparaginase (5000
U/m2), etoposide (VP16; 300 mg/m2), aracytin
(Ara C; 300 mg/m2) in addition to triple intrathecal
(IT) therapy, which consisted of 2 courses of high-dose
methotrexate (MTX; 15 mg), 6-mercaptopurine (6-MP; 40 mg) and
dexamethasone (Dex; 4 mg). Consolidation therapy consisted of
high-dose MTX (500 mg/m2 over 1 h followed by 1500
mg/m2 over 23 h) and triple IT therapy. Continuation
therapy consisted of triple IT therapy and 15 cycles of an 8 week
course of VP16 + cyclophosphamide (300 mg/m2), 6-MP +
MTX (75 and 40 mg/m2), MTX + Ara C (40 and 300
mg/m2), VP16 + Ara C (300 mg/m2), 6-MP + high
dose MTX (75 mg/m2) and prednisone + VCR (40
mg/m2). During continuation therapy re-induction was
administered in the form of VCR, daunomycin, Dex, high dose MTX,
6-MP and triple IT therapy.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Patient bone marrow samples were collected in
heparinized glass tubes and mononuclear cells were isolated by
Ficoll gradient centrifugation using a High Pure RNA Isolation kit
(Roche Diagnostics GmbH, Mannheim, Germany). Total RNA from the
mononuclear bone marrow cells of the patients was extracted using
the High Pure RNA Isolation kit (Roche Diagnostics GmbH), according
to the manufacturer's protocol. RNA quantity and quality were
assessed using spectrophotometric measurements at 260/280 nm (V1000
Visible Spectrophotometer; AOE Instruments (Shanghai) Co., Ltd.,
Shanghai, China). The starting concentration of the RNA was 30 µl.
Reverse transcription was performed with 25.0 µl total RNA, 2.5 µl
reverse transcriptase, 5.0 µl reverse transcriptase buffer, 4.0 µl
deoxynucleotides, 5.0 µl random primers and 8.5 µl H2O.
The reaction was incubated at 42°C for 1 h and inactivated by
heating to 95°C for 5 min. qPCR was performed using a MicroAmp
Optical 96-well plate (Thermo Fisher Scientific, Inc., Waltham, MA,
USA) with 10 µl cDNA, 1.0 µl of the forward and reverse primers, 10
µl distilled water, 0.5 µl Taqman probe (Sigma Scientific Services
Co., Cairo, Egypt) and 25 µl universal master mix (Qiagen, Inc.).
The expression levels of LMO2 and glyceraldehyde-3-phosphate
dehydrogenase (GAPDH; reference gene) were quantified using qPCR
analysis on an ABI Prism 7700 sequence detection system (Thermo
Fisher Scientific, Inc.). The PCR program was as follows: 50°C for
2 min, 95°C for 10 min, then 40 cycles of 95°C for 15 sec and 60°C
for 1 min.
The following primers were used for qPCR at a
concentration of 1.0 µl: LMO2, forward 5′GGCGGCGCCTCTACTACA-3′,
reverse 5′-CCAAAAAGCCTGAGATAGTCTCT-3′ and probe
5′-CTGGGCCGGAAGCTCTGCC-3′; GAPDH, forward
5′-GAAGGTGAAGGTCGGAGTC-3′, reverse 5′-GAAGATGGTGATGGGATTTC-3′ and
probe VIC-CAAGCTTCCCGTTCTCAGCC-TAMRA. The relative expression level
of LMO2 was measured using the comparative cycle threshold method
(26). The experiment was performed
twice.
Statistical analysis
SPSS software version 15.0 (SPSS, Inc., Chicago, IL,
USA) was used for statistical analysis. To compare LMO2 expression
between various groups, the Mann-Whitney U-test and the
Kruskal-Wallis H-test were used. Overall survival (OS) time was
defined as the time interval between the date of diagnosis and the
date of that the patient succumbed to the disease or the date of
the last follow-up. Disease-free survival (DFS) was measured
between the date of complete remission to the date of relapse or
the date the patient succumbed to the disease. Cox regression
analysis was performed for all patient variables. All descriptive
statistics and tests were calculated using SPSS. P<0.05 was
considered to indicate a statistically significant difference.
Results
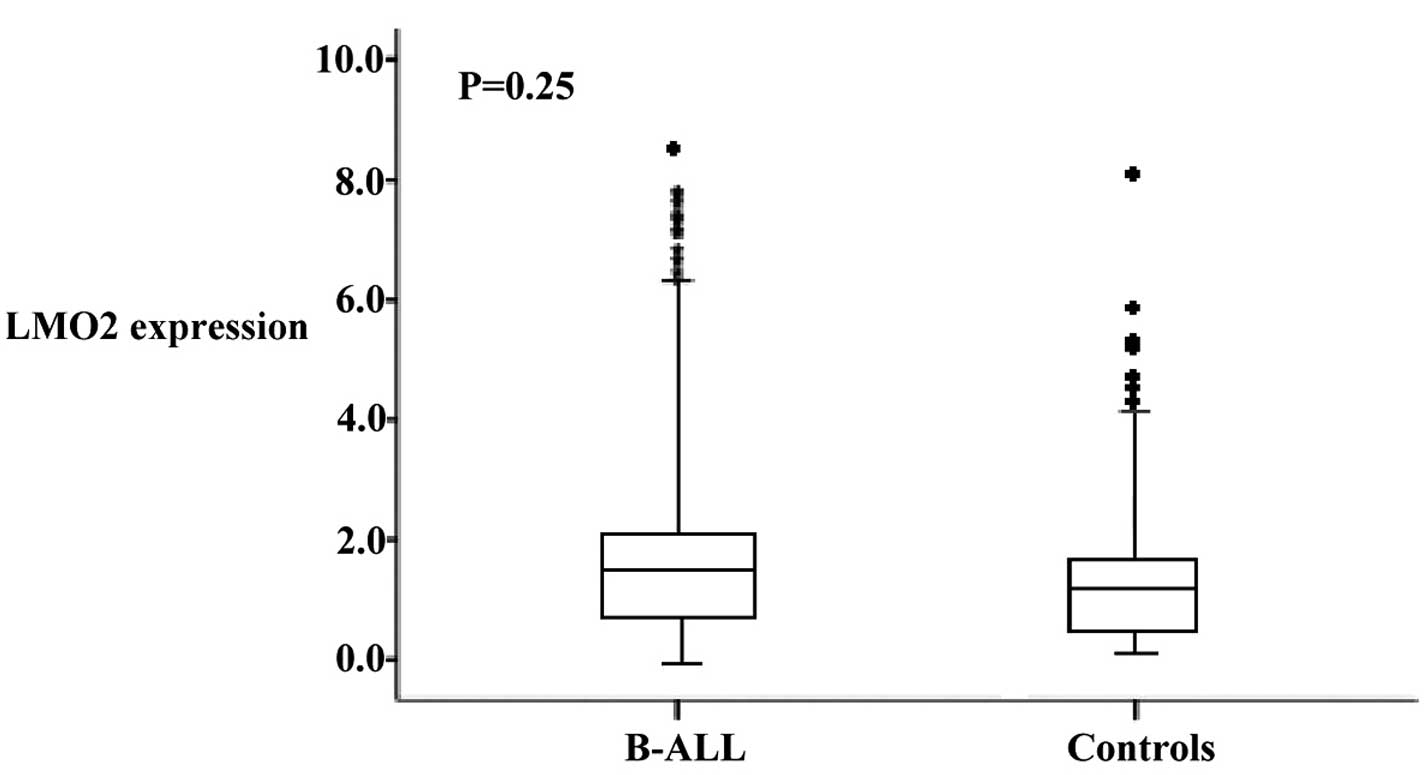
LMO2 expression in BCR/ABL negative
B-ALL patients and control individuals
LMO2 expression was decreased in control individuals
(mean relative expression, 1.75; range, 0.05–8.0) compared with
B-ALL patients (mean, 1.82; range, 0.07–8.2). The difference was
not statistically significant (P=0.25; Fig. 1).
LMO2 expression levels in association
with clinical and molecular variables of patients with B-ALL
The present study divided the patients into two
subgroups with high or low levels of LMO2 expression using the
median LMO2 expression (median, 1.82) value of the whole cohort as
a cut-off value. Table I reveals that
among subgroups, pro-B exhibited the highest LMO2 expression while
B-ALL with common-cluster of differentiation (CD)10+
immunophenotype, pre-B-ALL and mature B-ALL had a lower expression
(P=0.01). Pro-B immunophenotype occurred more commonly in patients
with a high LMO2 expression compared with patients with low LMO2
expression (36.9 vs. 15.3%). Common CD10+ and pre-B
immunophenotypes were more commonly observed in patients with low
LMO2 expression levels. However, no significant differences were
observed between patients with high and low LMO2 expression levels
for age, gender and total white blood cell count (TWBC).
 | Table I.Clinical and molecular characteristics
at diagnosis in adult patients with B-cell acute lymphoblastic
leukemia, according to LMO2 expression. |
Table I.
Clinical and molecular characteristics
at diagnosis in adult patients with B-cell acute lymphoblastic
leukemia, according to LMO2 expression.
| Characteristic | Total, value | High LMO2 expression,
value | Low LMO2 expression,
value | P-value |
|---|
| Total, n (%) | 85 (100.0) | 46 (46.0) | 39 (39.0) |
| Age, years |
|
|
|
|
|
Median | 52 | 50 | 52 | 0.64 |
|
Range | 19–62 | 19–60 | 19–61 |
|
| Gender, n (%) |
|
|
|
|
|
Male | 48 | 26 (56.5) | 22 (56.4) | 0.60 |
|
Female | 37 | 20 (43.5) | 17 (43.6) |
|
| TWBC, n (%) |
|
|
|
|
|
>50×109
cells/l | 34 | 18 (39.1) | 16 (41.0) | 0.32 |
|
<50×109
cells/l | 51 | 29 (63.0) | 22 (56.4) |
|
| Immunophenotype, n
(%) |
|
|
|
|
|
Pro-B | 25 | 17 (37.0) | 6
(15.4) | 0.01 |
| Common
(CD10+) | 51 | 27 (58.7) | 26 (66.6) |
|
|
Pre-B | 8 | 2 (4.3) | 6
(15.4) |
|
Mature | 1 | 0 (0.0) | 1 (2.6) |
Prognostic significance of LMO2
expression in adult patients with BCR/ABL negative B-ALL
Table II showed that
the complete remission (CR) rate of patients following induction
therapy was 72.9%. The CR rate was 82.6% in patients with high LMO2
expression and 61.5% in patients with low LMO2 expression (P=0.03).
The relapse rate was significantly different between the high and
low LMO2 expression groups (high vs. low, 17.3 vs. 43.5%; P=0.01).
Patients with high LMO2 expression demonstrated a lower induction
mortality rate compared with patients with low LMO2 expression
(high vs. low, 4.3% vs. 23.0%; P=0.03).
| Table II.Clinical outcome in adult patients
with B-cell acute lymphoblastic leukemia, according to LMO2
expression. |
Table II.
Clinical outcome in adult patients
with B-cell acute lymphoblastic leukemia, according to LMO2
expression.
| Clinical
outcome | Total, n (%) | High LMO2
expression, n (%) | Low LMO2
expression, n (%) | P-value |
|---|
| Total | 85 (100.0) | 46
(46.0) | 39 (39.0) |
|
| Complete
remission | 62 (72.9) | 38
(82.6) | 24 (61.5) | 0.03 |
| Refractory
disease | 12 (14.1) | 6
(13.0) | 6
(15.3) | 0.87 |
| Mortality
induction | 11 (12.9) | 2 (4.3) | 9
(23.0) | 0.03 |
| Relapse risk | 25 (29.4) | 8
(17.3) | 17 (43.5) | 0.01 |
Multivariate analysis of LMO2
expression is associated with the clinical outcome of patients
Multivariate analyses demonstrated that in patients
with BCR/ABL negative B-ALL, an increased expression of LMO2 was an
independent predictor for an improved OS rate [P=0.010; hazards
ratio (HR), 0.60; 95% confidence interval (CI), 0.32–0.85] and DFS
(P=0.020; HR, 0.56; 95% CI, 0.24–0.90) (Table III).
| Table III.Multivariate analysis of LMO2
expression for clinical outcome of adult patients with B-cell acute
lymphoblastic leukemia. |
Table III.
Multivariate analysis of LMO2
expression for clinical outcome of adult patients with B-cell acute
lymphoblastic leukemia.
|
| Overall survival
time | Disease-free
survival |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI for relative
risk | P-value | HR | 95% CI for relative
risk | P-value |
|---|
| LMO2
expression | 0.60 | 0.32–0.85 | 0.010 | 0.56 | 0.24–0.90 | 0.020 |
| Age | 0.80 | 0.55–0.95 | 0.425 | 0.85 | 0.49–0.98 | 0.456 |
| Gender | 0.78 | 0.32–1.05 | 0.892 | 0.94 | 0.60–1.05 | 0.680 |
|
Immunophenotype | 1.00 | 0.87–1.24 | 0.576 | 1.02 | 0.76–1.24 | 0.605 |
| WBC
>50×109 cells/l | 0.93 | 0.69–1.06 | 0.357 | 0.82 | 0.62–1.18 | 0.822 |
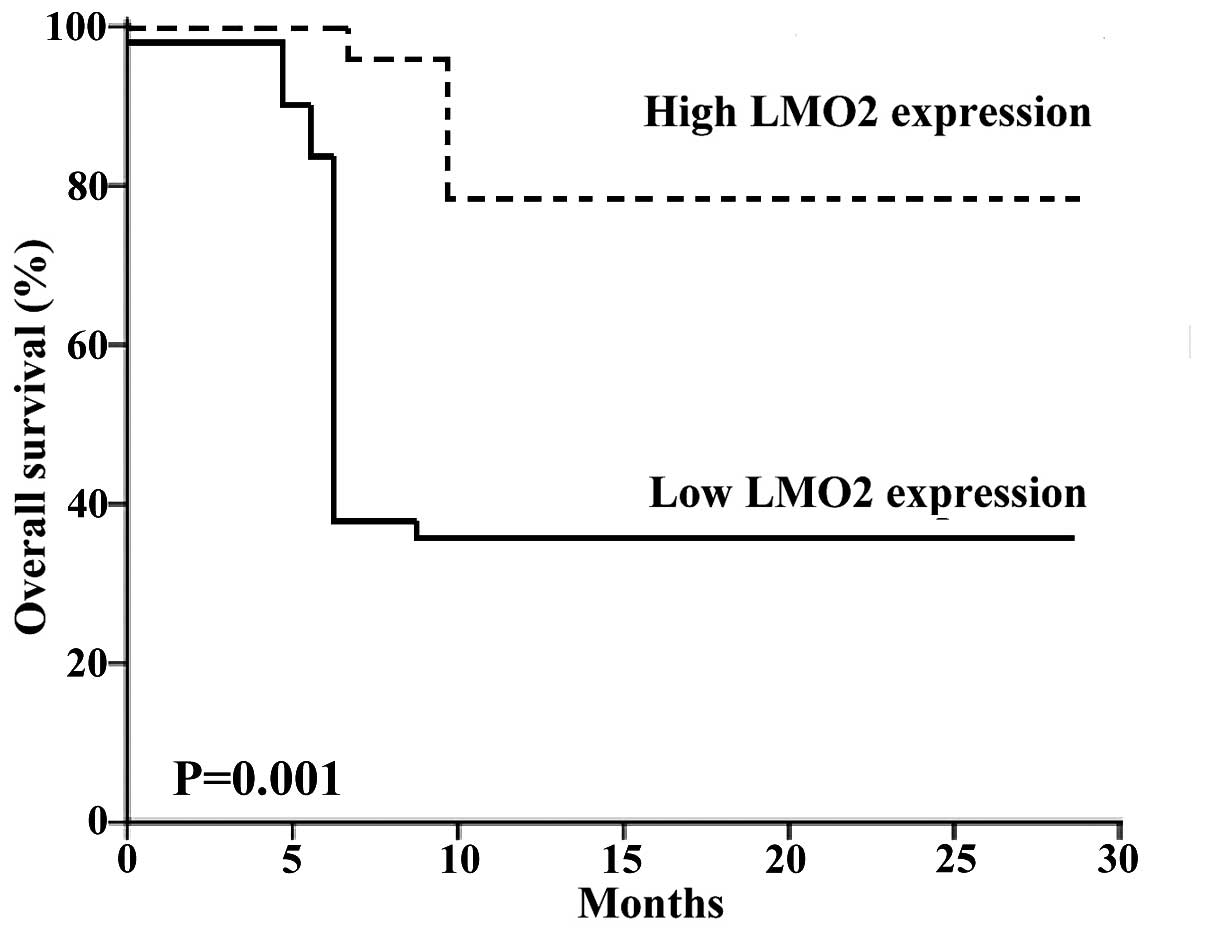
Patient outcome is associated with
LMO2 expression
The overall survival rate was significantly
increased in BCR/ABL negative B-ALL patients that were identified
as having high levels of LMO2 expression in comparison to those
patients with low levels of LMO2 expression (OS rate high LMO2,
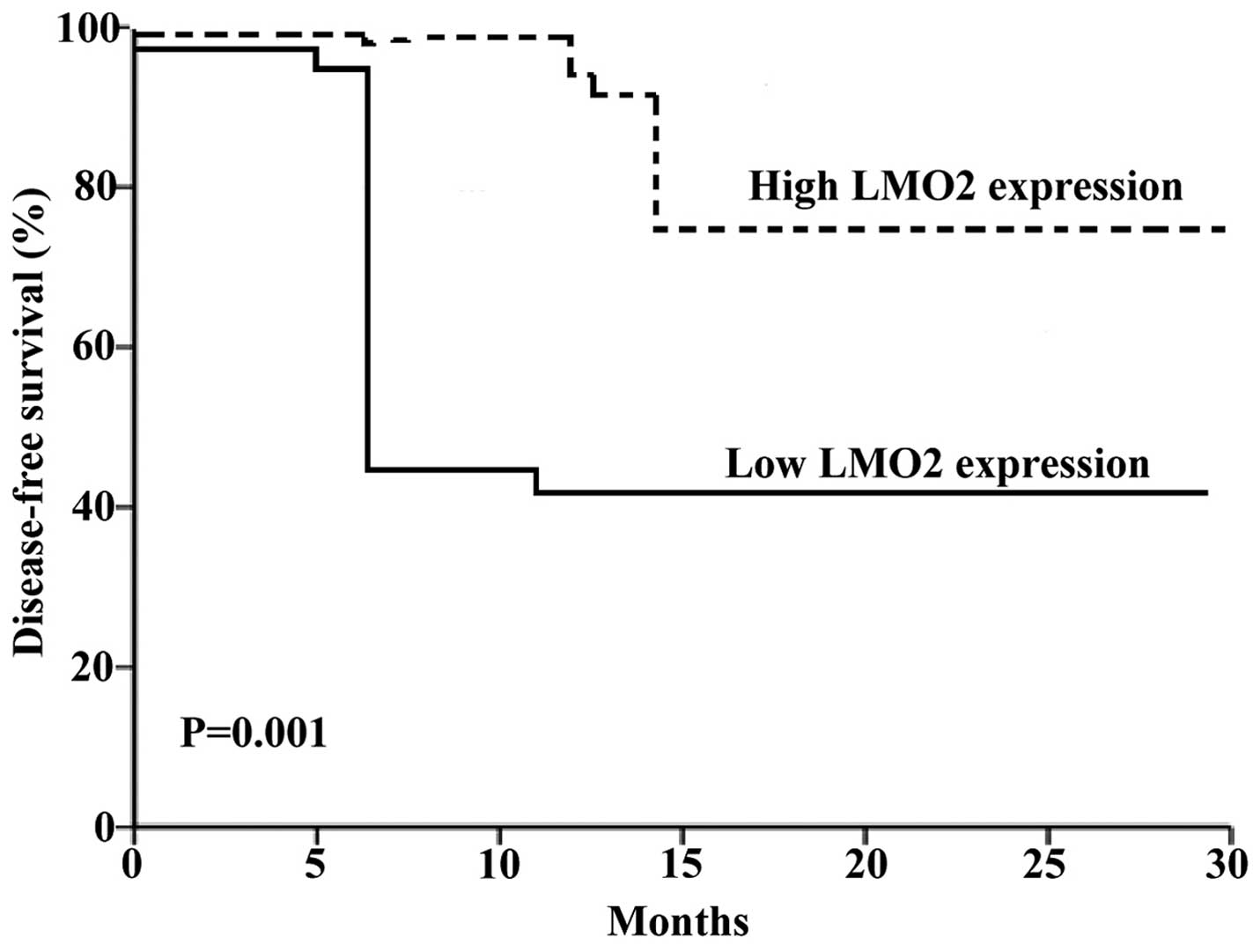
78.6%; OS rate low LMO2, 37.2%; P=0.001; Fig. 2). In addition, DFS was improved in
patients with high LMO2 expression compared with patients with low
LMO2 expression (high vs. low, 72.4 vs. 41.1%; P=0.001; Fig. 3).
Discussion
The identification of prognostic markers in
precursor B-ALL is required for the development of novel molecular
therapies that may improve risk-adapted treatment stratification
for patients with B-ALL. LMO2 is a key regulator of hematopoiesis
and vascular development (27). In
hematopoietic cells, it is observed to have a role as an
intranuclear bridging molecule, which aids in the formation of
protein-protein interactions in multiprotein complexes that are
required for the specification of cell lineage and differentiation
(28). It has been previously
reported that increased levels of LMO2 transcripts were observed in
CD34+ stem cells, and LMO2 protein expression was
clearly observed in endothelia, GC B cells and B-cell lymphoma
(29,30). In addition, activation of LMO2 has
been demonstrated in T-ALL, as a result of gene translocations and
deletions (31,32), and LMO1/2 is transcriptionally
deregulated in the majority of patients with acute T-ALL (33).
Previous studies have reported the potential role
for increased LMO2 expression in leukemia besides T-ALL. A previous
study demonstrated that LMO2 upregulation had a role in the
development of leukemia stem cell activity and disease in a mouse
model of AML (34). Furthermore,
studies revealed that there was an association between increased
LMO2 levels at diagnosis with patient outcome (35). LMO2 was also demonstrated to be
overexpressed in GC-type DLBCL (36),
and an association between LMO2 expression and tumor progression
was reported in patients with prostatic carcinoma (37).
Other studies have revealed that LMO2 was a
favorable prognostic factor in patients with CML and pancreatic
cancer (18,19), and its expression in patients with
DLBCL has been associated with a favorable outcome (38). The present study evaluated the
prognostic role of the LMO2 gene in adult patients with BCR/ABL
negative B-ALL and demonstrated that LMO2 was expressed in patients
with B-ALL. This has also been demonstrated by previous studies
(6,22).
Previously it was observed in SCID-X1 patients that
the introduction of a retrovirus vector into the LMO2 gene promoter
induced aberrant LMO2 expression, which resulted in the development
of T-ALL (39). In addition, LMO2 was
demonstrated to act as an oncogene in patients with T-ALL. However,
this possibly does not occur in patients with B-ALL. Previous
studies have reported that no LMO2 gene translocations have been
identified in B-ALL, and other genetic alterations, which involve
the LMO2 locus, are extremely rare among patients with B-ALL.
Furthermore, in a genome-wide analysis only 1 out of 192 B-ALL
samples revealed a 155 kb deletion upstream of the LMO2 gene locus;
by contrast, 8% of T-ALL samples exhibited this alteration
(40). In addition, it was
demonstrated that B cells induce LMO2 expression during the immune
response in the GC reaction, and this expression reaches levels
similar to that exhibited by pro-B cells (22). Therefore, these results suggest that
LMO2 does not act as an oncogene in B-ALL in contrast to T-ALL. In
the present study, pro-B-ALL was more common in patients with a
high LMO2 expression, which is in agreement with a previous study
that revealed that there was an association between the pro-B
immunophenotype and a high LMO2 expression (22).
The present study demonstrated that high LMO2
expression independently predicts an increased OS time in patients
with BCR/ABL negative B-ALL in comparison to patients with low LMO2
expression. This was in agreement with Malumbres et al
(22), who demonstrated that there
was an improved OS rate of patients with normal karyotype B-ALL
that had a high LMO2 transcript expression. This observation was
also observed in patients with CML (18) and DLBCL (38). The present study observed that a high
LMO2 expression was associated with improved DFS in patients with
BCR/ABL negative B-ALL; however, Malumbres et al (22) did not identify any association between
LMO2 expression and DFS in the subgroup of patients with a normal
karyotype B-ALL, possibly due to the low number of relapses in this
subgroup. The association between high LMO2 expression and
increased OS time and improved DFS was additionally confirmed in
multivariable analyses performed by the present study that adjusted
for the most important clinical and molecular prognosis
characteristics in ALL, including age, gender, immunophenotype and
TWBC of >50,000/mm3. The present results were in
agreement with a previous study that demonstrated that a high LMO2
expression was as an independent favorable prognostic factor for OS
rate in patients with normal karyotype B-ALL (22).
Previously LMO2 protein expression did not predict
patient survival in 22 patients with B-ALL, which was evaluated
using immunohistochemistry (21).
This may be due to the low number of patients with B-ALL enrolled
in that study, as well as the lack of immunophenotype
stratification. Therefore, LMO2 expression may be used to
additionally refine risk stratification for patients with BCR/ABL
negative B-ALL. However, additional studies with large and
molecularly well-characterized cohorts are required to develop and
confirm this improved risk classification system for B-ALL.
In summary, the present study provides evidence that
a high LMO2 expression is associated with favorable outcomes in
adult patients with B-ALL, even following adjustment for known
clinical and molecular risk factors.
References
|
1
|
Van Vlierberghe P, van Grotel M, Beverloo
HB, Lee C, Helgason T, Buijs-Gladdines J, Passier M, van Wering ER,
Veerman AJ, Kamps WA, et al: The cryptic chromosomal deletion
del(11)(p12p13) as a new activation mechanism of LMO2 in pediatric
T-cell acute lymphoblastic leukemia. Blood. 108:3520–3529. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Boehm T, Foroni L, Kaneko Y, Perutz MF and
Rabbitts TH: The rhombotin family of cysteine-rich LIM-domain
oncogenes: Distinct members are involved in T-cell translocations
to human chromosomes 11p15 and 11p13. Proc Natl Acad Sci USA.
88:4367–4371. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yamada Y, Warren AJ, Dobson C, Forster A,
Pannell R and Rabbitts TH: The T cell leukemia LIM protein Lmo2 is
necessary for adult mouse hematopoiesis. Proc Natl Acad Sci USA.
95:3890–3895. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yamada Y, Pannell R, Forster A and
Rabbitts TH: The oncogenic LIM-only transcription factor Lmo2
regulates angiogenesis but not vasculogenesis in mice. Proc Natl
Acad Sci USA. 97:320–324. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nam CH and Rabbitts TH: Role of LMO2 in
the development and in T cell leukemia after chromosomal
translocation or retroviral insertion. Mol Ther. 13:15–25. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Natkunam Y, Zhao S, Mason DY, Chen J,
Taidi B, Jones M, Hammer AS, Dutoit Hamilton S, Lossos IS and Levy
R: The oncoprotein LMO2 is expressed in normal germinal center B
cells and in human B-cell lymphomas. Blood. 109:1636–1642. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Royer-Pokora B, Loos U and Ludwig WD:
TTG-2, a new gene encoding a cysteine-rich protein with the LIM
motif, is overexpressed in acute T-cell leukaemia with the
t(11;14)(p13;q11). Oncogene. 6:1887–1893. 1991.PubMed/NCBI
|
|
8
|
McCormack MP and Rabbitts TH: Activation
of the T-cell oncogene LMO2 after gene therapy for X-linked severe
combined immunodeficiency. N Engl J Med. 350:913–922. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dong WF, Billia F, Atkins HL, Iscove NN
and Minden MD: Expression of rhombotin 2 in normal and leukaemic
haemopoietic cells. Br J Haematol. 93:280–286. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ferrando AA, Neuberg DS, Staunton J, Loh
ML, Huard C, Raimondi SC, Behm FG, Pui CH, Downing JR, Gilliland
DG, et al: Gene expression signatures define novel oncogenic
pathways in T cell acute lymphoblastic leukemia. Cancer Cell.
1:75–87. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Royer-Pokora B, Rogers M, Zhu TH,
Schneider S, Loos U and Bölitz U: The TTG-2⁄RBTN2 T cell oncogene
encodes two alternative transcripts from two promoters: The distal
promoter is removed by most 11p13 translocations in acute T cell
leukaemia's (T-ALL). Oncogene. 10:1353–1360. 1995.PubMed/NCBI
|
|
12
|
Hammond SM, Crable SC and Anderson KP:
Negative regulatory elements are present in the human LMO2 oncogene
and may contribute to its expression in leukemia. Leuk Res.
29:89–97. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hacein-Bey-Abina S, Von Kalle C, Schmidt
M, McCormack MP, Wulffraat N, Leboulch P, Lim A, Osborne CS,
Pawliuk R, Morillon E, et al: LMO2-associated clonal T cell
proliferation in two patients after gene therapy for SCID-X1.
Science. 302:415–419. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Howe SJ, Mansour MR, Schwarzwaelder K,
Bartholomae C, Hubank M, Kempski H, Brugman MH, Pike-Overzet K,
Chatters SJ, de Ridder D, et al: Insertional mutagenesis combined
with acquired somatic mutations causes leukemogenesis following
gene therapy of SCID-X1 patients. J Clin Invest. 118:3143–3150.
2008. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wu C and Dunbar CE: Stem cell gene
therapy: The risks of insertional mutagenesis and approaches to
minimize genotoxicity. Front Med. 5:356–371. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fisch P, Boehm T, Lavenir I, Larson T,
Arno J, Forster A and Rabbitts TH: T-cell acute lymphoblastic
lymphoma induced in transgenic mice by the RBTN1 and RBTN2
LIM-domain genes. Oncogene. 7:2389–2397. 1992.PubMed/NCBI
|
|
17
|
Patel JL, Pournazari P, Haggstrom SJ,
Kosari F, Shabani-Rad MT, Natkunam Y and Mansoor A: LMO2 (LIM
domain only 2) is expressed in a subset of acute myeloid leukaemia
and correlates with normal Karyotype. Histopathology. 64:226–233.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sonmez M, Akagun T, Cobanoglu U, Topbas M,
Erkut N, Yilmaz M, Ovali E and Omay SB: Effect of LMO2 protein
expression on survival in chronic myeloid leukemia patients treated
with imatinib mesylate. Hematology. 14:220–223. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nakata K, Ohuchida K, Nagai E, Hayashi A,
Miyasaka Y, Kayashima T, Yu J, Aishima S, Oda Y, Mizumoto K, et al:
LMO2 is a novel predictive marker for a better prognosis in
pancreatic cancer. Neoplasia. 11:712–719. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lossos IS, Czerwinski DK, Alizadeh AA,
Wechser MA, Tibshirani R, Botstein D and Levy R: Prediction of
survival in diffuse large-B-cell lymphoma based on the expression
of six genes. N Engl J Med. 350:1828–1837. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cobanoglu U, Sonmez M, Ozbas HM, Erkut N
and Can G: The expression of LMO2 protein in acute B-cell and
myeloid leukemia. Hematology. 15:132–134. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Malumbres R, Fresquet V, Roman-Gomez J,
Bobadilla M, Robles EF, Altobelli GG, Calasanz MJ, Smeland EB,
Aznar MA, Agirre X, et al: LMO2 expression reflects the different
stages of blast maturation and genetic features in B-cell acute
lymphoblastic leukemia and predicts clinical outcome. Hematologica.
96:980–986. 2011. View Article : Google Scholar
|
|
23
|
Swerdlow SH, Campo E, Harris NL, Jaffe ES,
Pileri SA, Stein H, Thiele J and Vardiman JW: WHO Classification of
Tumors of Haematopoietic and Lymphoid Tissues. 2:(4th). Lyon,
France: IARC. 2008.
|
|
24
|
Ludwig WD, Rieder H, Bartram CR, Heinze B,
Schwartz S, Gassmann W, Löffler H, Hossfeld D, Heil G, Handt S, et
al: Immunophenotypic and genotypic features, clinical
characteristics, and treatment outcome of adult pro-B acute
lymphoblastic leukaemia: Results of the German multicenter trials
GMALL 03/87 and 04/89. Blood. 92:1898–1909. 1998.PubMed/NCBI
|
|
25
|
Schwartz S, Rieder H, Schläger B,
Burmeister T, Fischer L and Thiel E: Expression of the human
homologue of rat NG2 in adult acute lymphoblastic leukemia: Close
association with MLL rearrangement and a
CD10(−)/CD24(−)/CD65s(+)/CD15(+) B-cell phenotype. Leukemia.
17:1589–1595. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Meijeerink J, Mandigers C, Van de Locht L,
Tönnissen E, Goodsaid F and Raemaekers J: A novel method to
compensate for different amplification efficiencies between patient
DNA samples in quantitative real time PCR. J Mol Diagn. 3:55–61.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Omari K, Hoosdally SJ, Tuladhar K, Karia
D, Vyas P, Patient R, Porche C and Mancini EJ: Structure of the
leukemia oncogene LMO2: Implications for the assembly of a
hematopoietic transcription factor complex. Blood. 117:2146–2156.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bach I: The LIM domain: Regulation by
association. Mech Dev. 91:5–17. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gratzinger D, Zhao S, West R, Rouse RV,
Vogel H, Gil EC, Levy R, Lossos IS and Natkunam Y: The
transcription factor LMO2 is a robust marker of vascular
endothelium and vascular neoplasms and selected other entities. Am
J Clin Pathol. 131:264–278. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Pike-Overzet K, de Ridder D, Weerkamp F,
Baert MR, Verstegen MM, Brugman MH, Howe SJ, Reinders MJ, Thrasher
AJ, Wagemaker G, et al: Ectopic retroviral expression of LMO2, but
not IL2Rgamma, blocks human T-cell development from
CD34+ cells: Implications for leukemogenesis in gene
therapy. Leukemia. 21:754–763. 2007.PubMed/NCBI
|
|
31
|
Van Vlierberghe P, van Grotel M, Beverloo
HB, Lee C, Helgason T, Buijs-Gladdines J, Passier M, van Wering ER,
Veerman AJ, Kamps WA, et al: The cryptic chromosomal deletion
del(11)(p12p13) as a new activation mechanism of LMO2 in pediatric
T-cell acute lymphoblastic leukemia. Blood. 108:3520–3529. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Van Vlierberghe P, Beverloo HB,
Buijs-Gladdines J, van Wering ER, Horstmann M, Pieters R and
Meijerink JP: Monoallelic or biallelic LMO2 expression in relation
to the LMO2 rearrangement status in pediatric T-cell acute
lymphoblastic leukemia. Leukemia. 22:1434–1437. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nam CH and Rabbitts TH: The role of LMO2
in development and in T cell leukemia after chromosomal
translocation or retroviral insertion. Mol Ther. 13:15–25. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kvinlaug BT, Chan WI, Bullinger L,
Ramaswami M, Sears C, Foster D, Lazic SE, Okabe R, Benner A, Lee
BH, et al: Common and overlapping oncogenic pathways contribute to
the evolution of acute myeloid leukemias. Cancer Res. 71:4117–4129.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Calero-Nieto FJ, Joshil A, Bonadies N,
Kinston S, Chan WI, Gudgin1 E, Pridans C, Landry JR, Kikuchi J,
Huntly BJ and Gottgens B: HOX-mediated LMO2 expression in embryonic
mesoderm is recapitulated in acute leukemia. Oncogene.
32:5471–5480. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Alizadeh AA, Eisen MB, Davis RE, Ma C,
Lossos IS, Rosenwald A, Boldrick JC, Sabet H, Tran T, Yu X, et al:
Distinct types of diffuse large B-cell lymphoma identified by gene
expression profiling. Nature. 403:503–511. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ma S, Guan XY, Beh PS, Wong KY, Chan YP,
Yuen HF, Vielkind J and Chan KW: The significance of LMO2
expression in the progression of prostate cancer. J Pathol.
211:278–285. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Natkunam Y, Farinha P, Hsi ED, Hans CP,
Tibshirani R, Sehn LH, Connors JM, Gratzinger D, Rosado M, Zhao S,
et al: LMO2 protein expression predicts survival in patients with
diffuse large B-cell lymphoma treated with anthracycline-based
chemotherapy with and without rituximab. J Clin Oncol. 26:447–454.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hacein-Bey-Abina S, Garrigue A, Wang GP,
Soulier J, Lim A, Morillon E, Clappier E, Caccavelli L, Delabesse
E, Beldjord K, et al: Insertional oncogenesis in 4 patients after
retrovirus-mediated gene therapy of SCID-X1. J Clin Invest.
118:3132–3142. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
40
|
Mullighan CG, Goorha S, Radtke I, Miller
CB, Coustan-Smith E, Dalton JD, Girtman K, Mathew S, Ma J, Pounds
SB, et al: Genome-wide analysis of genetic alterations in acute
lymphoblastic leukaemia. Nature. 446:758–764. 2007. View Article : Google Scholar : PubMed/NCBI
|