Introduction
Cutaneous and systemic plasmacytosis is a rare
condition characterized by an infiltration of mature plasma cells
in various organ systems, which manifests clinically in the form of
red-brown macules, papules and plaques. Since plasmacytosis
regularly occurs at extracutaneous sites, the disorder is thus
currently known as ‘cutaneous and systemic plasmacytosis’ (1). This disorder is usually accompanied by
fever, anemia, polyclonal hypergammaglobulinemia and superficial
lymphadenopathy (2). Cutaneous and
systemic plasmacytosis is an uncommon disorder with <100
patients described in the literature thus far, the majority of whom
are Japanese (3). A previous study
suggested that cutaneous and systemic plasmacytosis has a male to
female ratio of 1.0:0.6, and an age of onset between 20 and 62
years with a mean and median age of 37 years (4). The condition is usually diagnosed via
biopsy; histologically, superficial and deep perivascular and
perineural dermatitis with prominent plasma cells is observed
(5). Overall, the prognosis of the
disorder is favorable, although rare cases have been reported with
a more aggressive clinical course, including the development of
lymphoma (5). Treatment with
immunosuppressive agents of variable potency has been described
with a degree of success; however, there is not a common effective
treatment (2). The present study
reports a case of cutaneous and systemic plasmacytosis on the face
that occurred in a patient of Chinese origin. Written informed
consent was obtained from the patient.
Case report
A 50-year-old female from mainland China presented
to The First Affiliated Hospital of Chongqing Medical University
(Chongqing, China) for evaluation of diffuse, asymptomatic
purplish-red macules that had been present on the face for one
year. The lesions initially started on the upper lip, and then
disseminated to the other areas of the face, nose and forehead,
with main dispersal on the lips and perioral area. The patient had
previously been diagnosed with seborrheic dermatitis and treated
with antihistamine drugs, without any improvement.
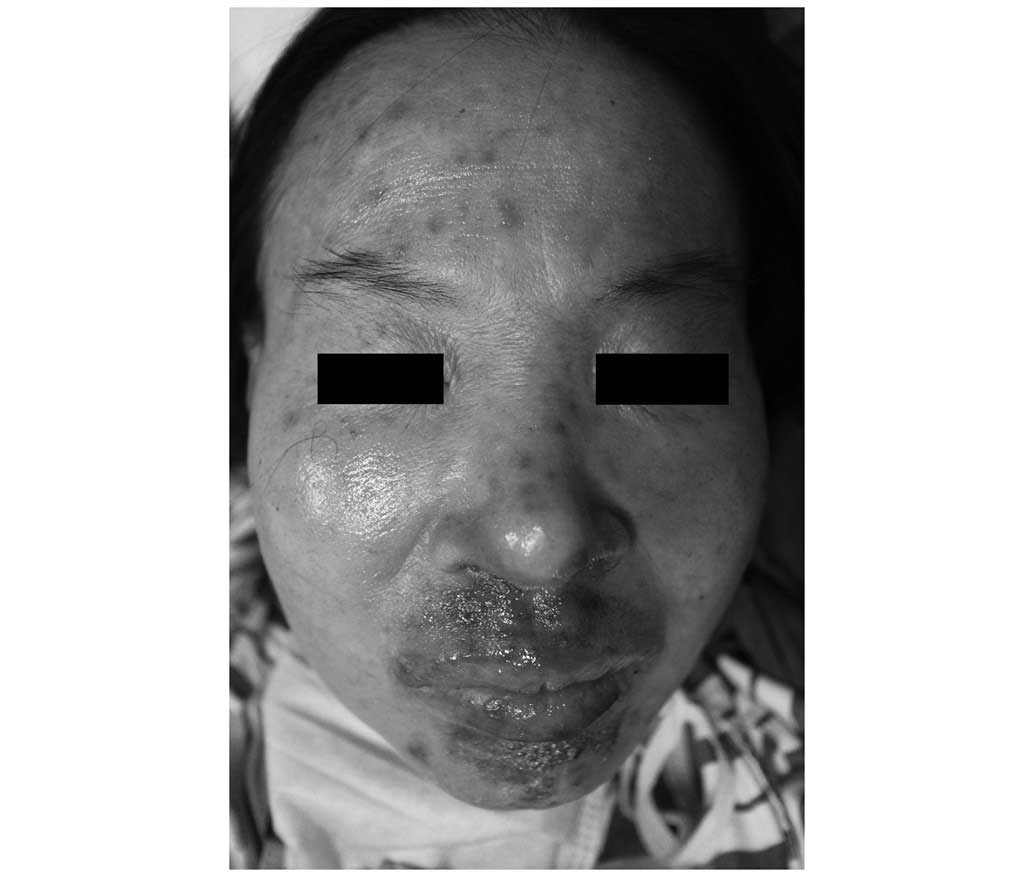
A physical examination revealed multiple
red-brownish macules, plaques and nodules, measuring 1–2 cm in
diameter, distributed symmetrically on the face, particularly the
lips and perioral area where the papules had fused to form plaques
(Fig. 1). In addition, non-tender
peripheral lymphadenopathy was detected in the cervical, axillary
and inguinal regions. No hepatosplenomegaly was revealed. There was
no family history of plasmacytosis and the patient's general
condition was good. Laboratory examinations revealed no
abnormalities in complete blood count, serum human immunodeficiency
virus antibody level, rapid plasma reagin, antinuclear antibody and
extractable nuclear antigen. Urinalysis repeat examinations did not
show any evidence of Bence-Jones protein in the urine. A bone X-ray
showed no signs of myeloma and a bone marrow smear showed no signs
of malignant plasmacytoma. The erythrocyte sedimentation rate was
elevated at 105 mm/h (normal range, 0–15 mm/h). Serum protein
electrophoresis demonstrated polyclonal hypergammaglobulinaemia as
follows: 2,120 mg/dl immunoglobulin (Ig)G (normal range, 751–1,560
mg/dl), 633 mg/dl IgA (range, 82–453 mg/dl) and 311 mg/dl IgM
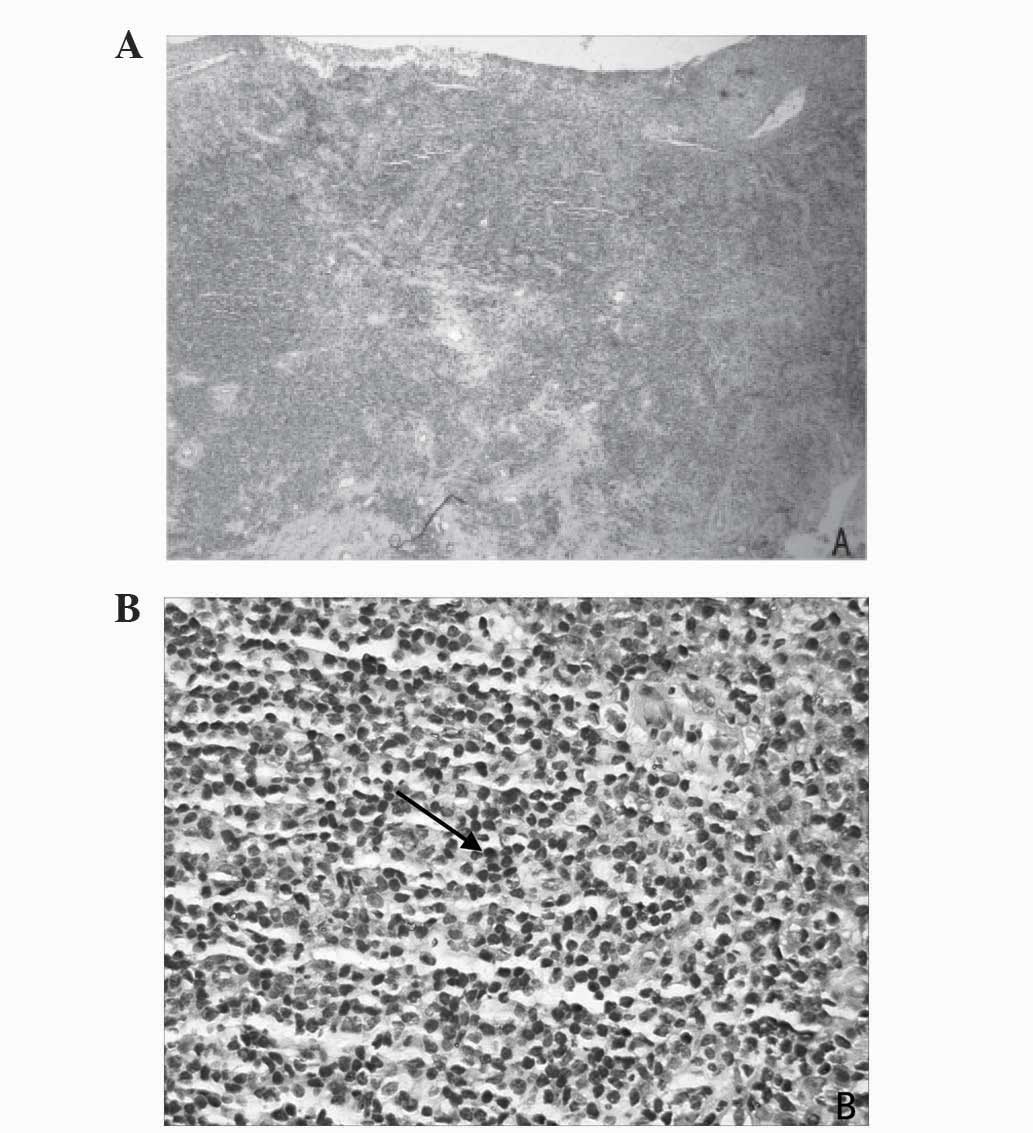
(range, 46–304 mg/dl). A skin biopsy taken from the upper lip and
stained with haematoxylin and eosin showed a dermal periadnexal
diffuse infiltrate, consisting mostly of plasma cells admixed with a
few lymphocytes and histiocytes (Fig.
2).
According to the typical clinical features,
histopathology results and laboratory examination, a diagnosis of
cutaneous and systemic plasmacytosis was made. The patient was
prescribed oral thalidomide (Changzhou Pharmaceutical Factory,
Changzhou, China) at a dose of 25 mg three times per day (75
mg/day). One and a half months after the start of the therapy, the
skin lesions had improved as the cutaneous plaques had decreased in
size. Three months after the start of the therapy, the skin lesions
had mostly cleared (Fig. 3). The
patient did not experience any adverse effects. Baseline sensory
nerve conduction studies were performed during the therapy as part
of the monitoring process for thalidomide-induced peripheral
neuropathy. In a recent telephone follow-up, the patient confirmed
that the condition continues to improve.
Discussion
Cutaneous and systemic plasmacytosis was first
reported by Yashiro (6) in a study
titled ‘A kind of plasmocytosis: Primary cutaneous plasmacytoma?’
in 1976 and its description was further refined in the 1980s by
Kitamura et al (7). To date,
the majority of cutaneous and systemic plasmacytosis cases have
been observed in Asian populations, and more specifically in
Japanese populations; all 41 patients reported by Uhara et
al (8) were Japanese. In
addition, isolated cases have been reported in Chinese, Korean and
Thai populations (9,10). Worldwide, cutaneous and systemic
plasmacytosis has only been reported in ~10 Caucasian patients
(11). The typical skin lesions are
asymptomatic, brownish, irregularly-shaped macules or plaques,
which are mostly disseminated on the trunk. The lesions also can
additionally involve the face or limbs. However, the presentation
of the current patient was slightly different in that the lesions
were just limited to the face. Aside from the compulsory cutaneous
manifestation, polyclonal hypergammaglobulinemia and
lymphadenopathy are the most frequent symptoms of the disease
(9). The majority of patients are
asymptomatic, although individuals with systemic involvement may
present with constitutional symptoms, including weight loss and
fatigue (3).
Given the rarity of cutaneous and systemic
plasmacytosis, no controlled therapeutic trials have thus far been
conducted, and a commonly effective treatment has not been
reported. Generally, the therapy for cutaneous and systemic
plasmacytosis has been quite disappointing until now. Studies have
shown that the most commonly used topical or intralesional
therapies performed with corticosteroids result in no, slight or an
only transient improvement (12,13).
Tacrolimus and pimecrolimus have been applied as treatment with
different effects. Ma et al (10) and Miura et al (14) reported that there was no or only
slight benefit when treated with tacrolimus, whereas Hafner et
al (15) recorded effective
treatment with pimecrolimus in one case. Other available topical
treatments for cutaneous plasmacytosis include radiotherapy,
photodynamic therapy and psoralen combined with ultraviolet A
(16). In individual cases, patient
have been treated with cyclophosphamide, vincristine, prednisone
and rituximab chemotherapy with only partial, transient resolution
of the lesions (17). Lee et
al (18) showed that systemic
plasmacytosis was improved with melphalan treatment.
To the best of our knowledge, the present study
reports the first case of an effective treatment of cutaneous and
systemic plasmacytosis with thalidomide. The main adverse effects
of thalidomide are sedation, fatigue, constipation, peripheral
neuropathy and thromboembolic phenomena; however, thalidomide
treatment was well tolerated in the present patient (19).
Cutaneous and systemic plasmacytosis is rare with an
unknown etiology. Multiple theories have been proposed, including
the elevation of interleukin (IL)-6 (13). The variability of humans
geographically or IL-6 genetic polymorphisms may possibly explain
the frequency of cutaneous and systemic plasmacytosis in individual
regions. Furthermore, Haque et al (20) hypothesized that due to the local
production of IL-6, long-lived plasma cells originate and survive
in the environment of the skin, and that such patients may
therefore respond to agents able to interfere with the activity of
IL-6. Thalidomide stimulates the cytotoxic functions of T
lymphocytes, thus limiting the immunosuppressive function of
regulatory T cells and significantly altering the immunological
profile by inhibiting the release of TNFα and IL-6 (21). We hypothesized that through decreased
secretion of IL-6, thalidomide may affect the growth of plasma
cells, which could be beneficial for the treatment of cutaneous and
systemic plasmacytosis.
Overall, the present study showed that systemic
thalidomide was effective in the treatment of cutaneous and
systemic plasmacytosis. The exact mechanism of action is unknown,
but the drug may act directly on plasma cells or alter the
immunological profile. However, further studies, including
randomized controlled trials, are required to confirm the benefit of
this association. Although the present study achieved great
improvements with low-dose thalidomide at 75 mg/day, individual
dosages may be different. The addition of other agents, such as
dexamethasone, may also improve the response rates. With monitoring
of nerve conduction studies, we believe that thalidomide and
topical tacrolimus could be considered as a safe therapeutic option
for patients with cutaneous and systemic plasmacytosis.
References
|
1
|
Tada Y, Komine M, Suzuki S, Kikuchi K,
Sasaki M, Kaneko N and Tamaki K: Plasmacytosis: Systemic or
cutaneous, are they distinct? Acta Derm Venereol. 80:233–235. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Carey WP, Rico MJ, Nierodzik M and Sidhu
G: Systemic plasmacytosis with cutaneous manifestations in a white
man: Successful therapy with cyclophosphamide/prednisone. J Am Acad
Dermatol. 38:629–631. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Honda R, Cerroni L, Tanikawa A, Ebihara T,
Amagai M and Ishiko A: Cutaneous plasmacytosis: Report of 6 cases
with or without systemic involvement. J Am Acad Dermatol.
68:978–985. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Leonard AL, Meehan SA, Ramsey D, Brown L
and Sen F: Cutaneous and systemic plasmacytosis. J Am Acad
Dermatol. 56(Suppl): S38–S40. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jayaraman AG, Cesca C and Kohler S:
Cutaneous plasmacytosis: A report of five cases with
immunohistochemical evaluation for HHV-8 expression. Am J
Dermatopathol. 28:93–98. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yashiro A: A kind of plasmacytosis:
Primary cutaneous plasmacytoma? Jpn J Dermatol. 86:9101976.
|
|
7
|
Kitamura K, Tamura N, Hatano H, Toyama K,
Mikata A and Watanabe S: A case of plasmacytosis with multiple
peculiar eruptions. J Dermatol. 7:341–349. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Uhara H, Saida T, Ikegawa S, Yamazaki Y,
Mikoshiba H, Nijoh S, Kitano K and Koh CS: Primary cutaneous
plasmacytosis: Report of three cases and review of the literature.
Dermatology. 189:251–2551994. View Article : Google Scholar
|
|
9
|
Wagner G, Rose C, Klapper W and Sachse MM:
Cutaneous and systemic plasmocytosis. J Dtsch Dermatol Ges.
11:1161–1167. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ma HJ, Liu W, Li Y, Zhao G, Meng RS and Li
DG: Cutaneous and systemic plasmacytosis: A Chinese case. J
Dermatol. 35:536–540. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
González-López MA, González-Vela MC,
Blanco R, Fernández-Llaca H and Val-Bernal JF: Cutaneous
plasmacytosis limited to the extremities in a white patient: An
unusual clinical picture. Cutis. 86:143–147. 2010.PubMed/NCBI
|
|
12
|
Ahn JJ, Yang YS, Shin MK, Lee SW and Kim
NI: Case of isolated benign primary cutaneous plasmacytosis in a
child. J Dermatol. 38:364–367. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yamamoto T, Katayama I and Nishioka K:
Increased plasma interleukin-6 in cutaneous plasmacytoma: The
effect of intralesional steroid therapy. Br J Dermatol.
137:631–636. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Miura H, Itami S and Yoshikawa K:
Treatment of facial lesion of cutaneous plasmacytosis with
tacrolimus ointment. J Am Acad Dermatol. 49:1195–1196. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hafner C, Hohenleutner U, Babilas P,
Landthaler M and Vogt T: Targeting T cells to hit B cells:
Successful treatment of cutaneous plasmacytosis with topical
pimecrolimus. Dermatology. 213:163–165. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tzung TY, Wu KH, Wu JC and Tseng HH:
Primary cutaneous plasmacytosis successfully treated with topical
photodynamic therapy. Acta Derm Venereol. 85:542–543.
2005.PubMed/NCBI
|
|
17
|
Amin HM, McLaughlin P, Rutherford CJ,
Abruzzo LV and Jones D: Cutaneous and systemic plasmacytosis in a
patient of Asian descent living in the United States. Am J
Dermatopathol. 24:241–245. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee DW, Choi SW, Park JW and Cho BK:
Systemic plasmacytosis: A case which improved with melphalan. J
Dermatol. 22:205–209. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Berrebi A, Feldberg E, Spivak I and
Shvidel L: Mini-dose of thalidomide for treatment of primary
myelofibrosis. Report of a case with complete reversal of bone
marrow fibrosis and splenomegaly. Haematologica:. 92:e15–e16. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Haque M, Hou JS, Hisamichi K, Tamada K,
Cusack CA, Abdelmalek M, Brown RE and Vonderheid EC: Cutaneous and
systemic plasmacytosis vs. cutaneous plasmacytic castleman disease:
Review and speculations about pathogenesis. Clin Lymphoma Myeloma
Leuk. 11:453–4561. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Semeraro M, Vacchelli E, Eggermont A,
Galon J, Zitvogel L, Kroemer G and Galluzzi L: Trial Watch:
Lenalidomide-based immunochemotherapy. Oncoimmunology.
2:e264942013. View Article : Google Scholar : PubMed/NCBI
|