Introduction
Parathyroid cysts (PCs) were first reported in 1880
in a study by Sandstrom, but PC removal from the neck was first
reported in 1905 in a study by Goris (1,2). PCs
account for 0.6% of all thyroid and parathyroid masses. These
lesions always arise in the posterior neck or anterior mediastinum
(3,4).
PCs may be functional or non-functional, depending on the ability
of the cyst to secrete parathyroid hormone (PTH). In total, 15–57%
of PCs are functional (5–7). In addition, the majority of
non-functional PC lesions are small in size and are occasionally
revealed during imaging procedures or cervical surgery, with only a
minority characterized by a large size and compressive symptoms
(8). The present study describes the
case of a man with a giant non-functional PC extending from the
lower neck to the superior mediastinum, and provides a brief
discussion regarding the associated literature in order to raise
awareness of this diagnosis.
Case report
A 56-year-old man was referred to the Affiliated
Tumor Hospital, Zhengzhou University (Zhengzhou, Henan, China) in
September 2014 with a 10 month history of exertional dyspnea, and
mild dysphagia that had persisted for 3 months. The medical history
of the patient included hypertension and an inguinal hernia repair,
which had occurred 10 years previously.
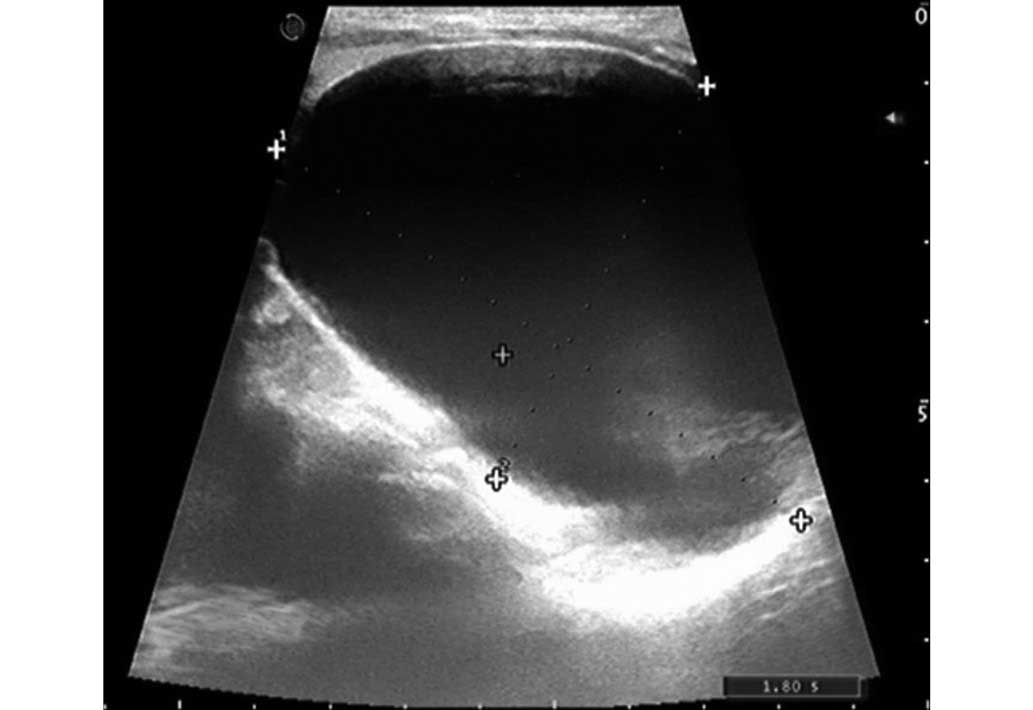
The physical examination revealed a palpable
round-shaped mass in the right thyroid lobe. The ultrasound
(Philips iU22; Philips Healthcare, Andover, MA, USA) showed a
8.4×5.7×3.6-cm cystic mass attached to the right thyroid lobe
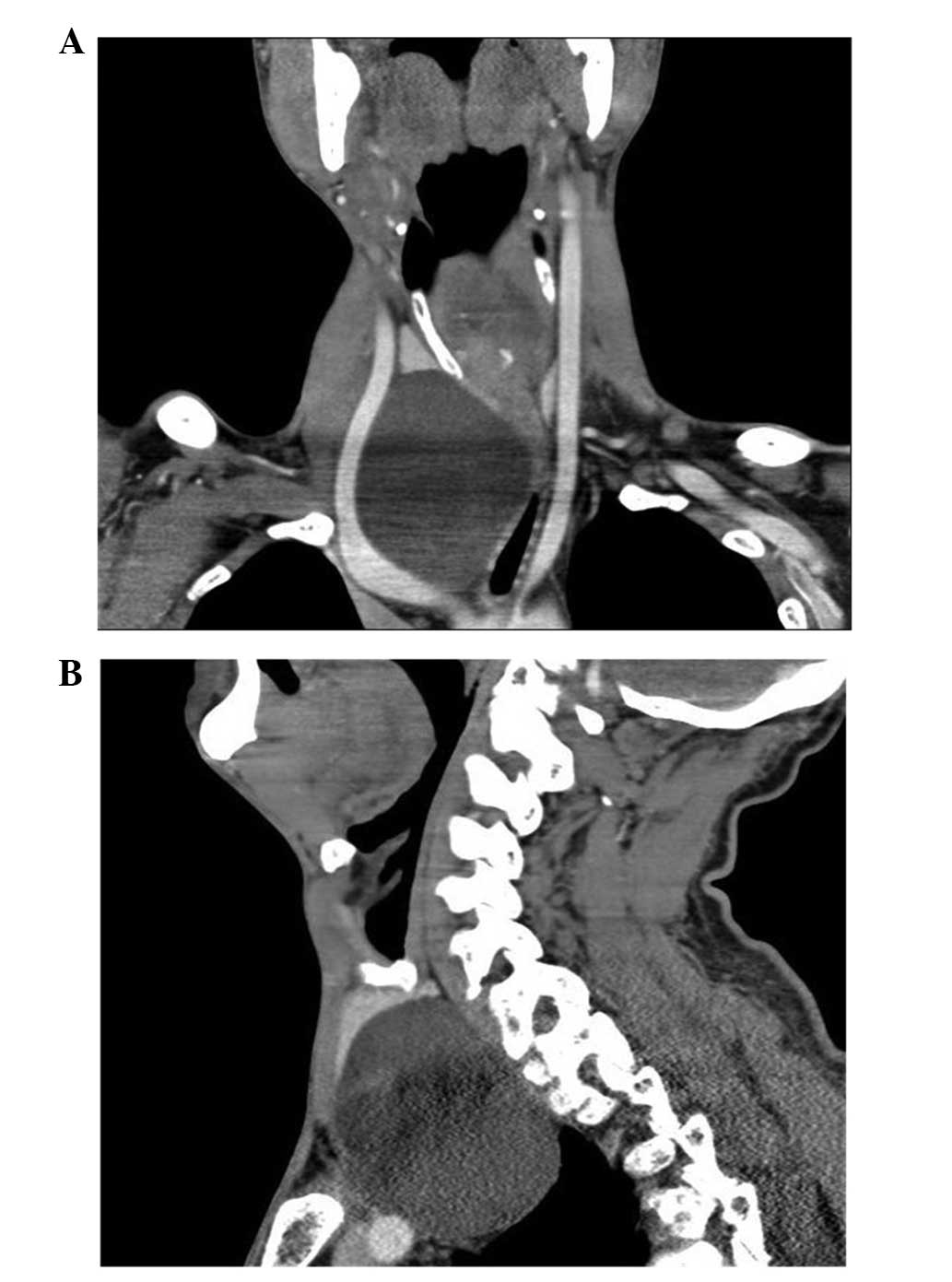
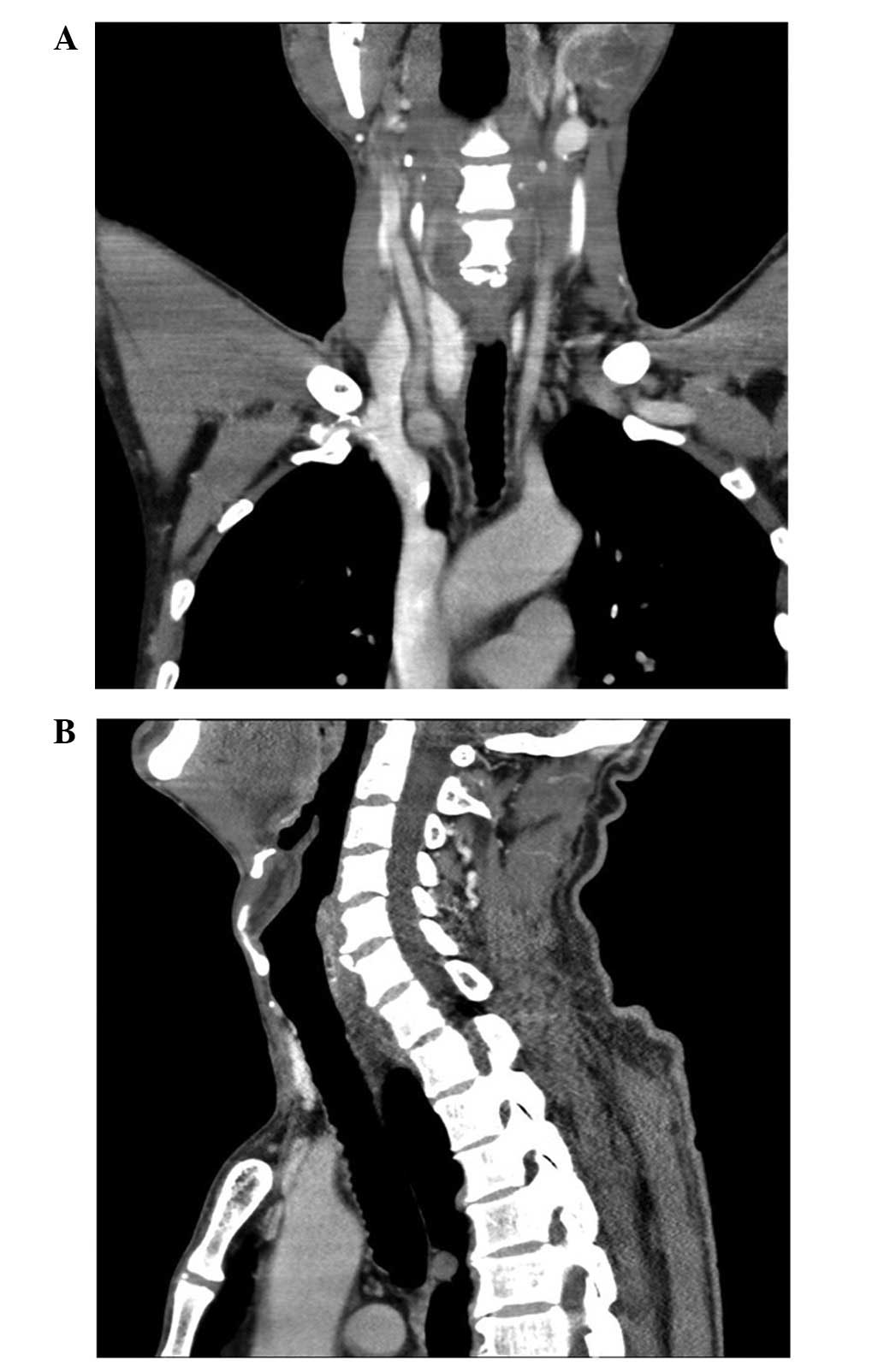
(Fig. 1). A neck and chest computed
tomography (CT; LightSpeed Pro32 spiral scanner with a layer
thickness of 5 mm; GE Healthcare Bio-Sciences, Pittsburgh, PA, USA)
scan was performed with contrast media, which showed the presence
of a large neck and mediastinal mass (9.0×6.0 cm) with no contrast
enhancement, causing right anterolateral displacement of the large
vessels and left anterolateral displacement of the trachea
(Fig. 2). The serum calcium and PTH
concentrations were measured and identified as normal, at 2.26
mmol/l (normal range, 2.03–2.54 mmol/l) and 37.98 pg/ml (normal
range, 15–65 pg/m), respectively. A fine-needle aspiration biopsy
(FNAB) was performed, and the content obtained from the cyst was a
colorless crystal clear fluid, suggesting that the mass was a PC.
The levels of PTH in the aspirated fluid were elevated (308 pg/ml;
normal serum range, 10–65 pg/ml). A cytological examination of the
material that was obtained following centrifugation of the fluid
showed a few epithelial cells that possibly belonged to the
parathyroid tissue. Based on the aforementioned findings, the
diagnosis of the giant cyst was of a non-functional PC.
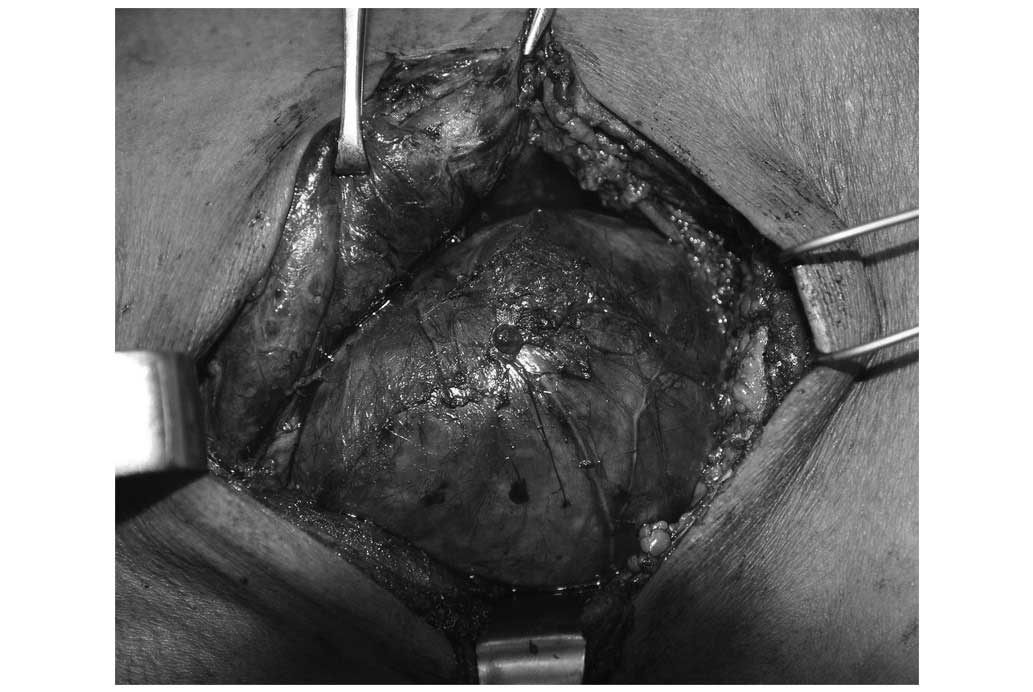
The patient underwent a right thyroid lobectomy and
isthmectomy, with the excision of the cyst. The appearance of the
giant PC was characterized by large cystic lesions with a thin wall
and a watery fluid component (Fig.
3).
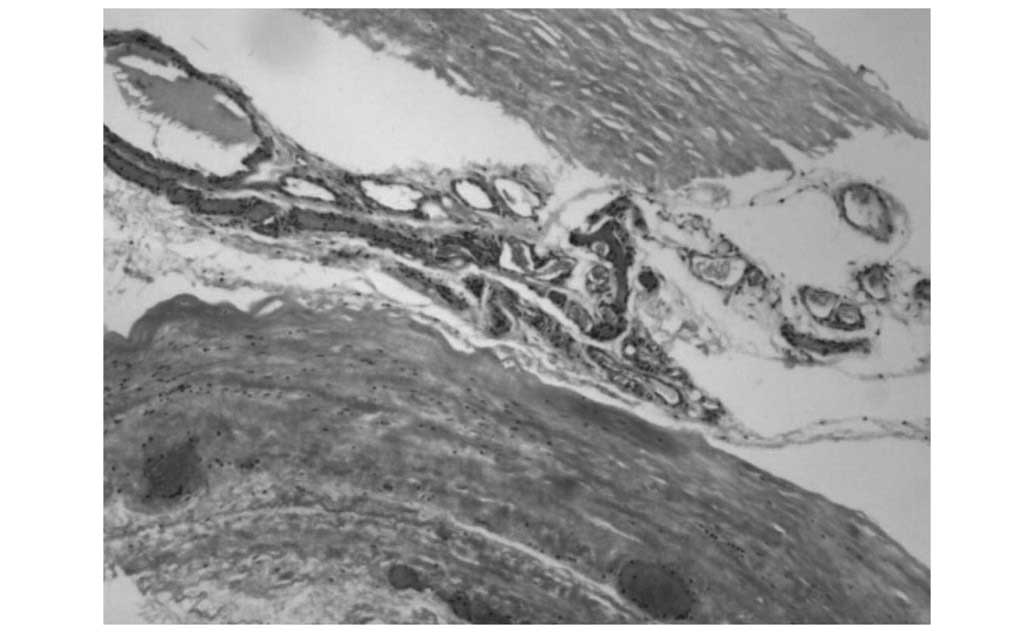
The cystic wall tissue was fixed in 10% formalin,
washed and dehydrated using alcohol and xylene, paraffin-embedded,
and stained with hematoxylin and eosin (Zhuhai Beisuo Biological
Technology Co., Ltd., Zhuhai, China) for examination. The
histological examination confirmed the presence of a giant PC. The
cyst was surrounded by a fibrous wall and possessed the focal
presence of hyperplastic parathyroid cells within the fibrotic
tissue. Neither mitotic figures nor nuclear atypia were observed
(Fig. 4).
No serious complications occurred subsequent to the
surgery. The calcium and PTH levels of the patient were monitored
post-operatively, and no abnormalities were identified. Symptoms
caused by the cyst were relieved immediately following surgery. The
patient was discharged 7 days after the surgery (Fig. 5). The patient remains asymptomatic,
with no recurrence at 3-month follow-up.
Discussion
PCs are rare, having been reported in just over 300
cases and possessing an incidence ranging between 0.075–3.000%
worldwide, as stated by previous studies (9,10). Giant
PCs that extend between the lower neck and superior mediastinum are
even rarer. McKay et al (11)
reported that in all of the PubMed studies that were published
since 1925, only 107 giant non-functioning PCs had been reported.
The study regarding large parathyroid cystic lesions that was
conducted by Rossi et al (12)
reported a 0.09% incidence over the last 15 years.
PCs may be misinterpreted as thyroid cystic lesions
due to the close spatial association with the thyroid gland.
Current diagnostic tools, including US, technetium-99m sestamibi
scanning, CT and magnetic resonance imaging, may often
differentiate between solid tumors and cystic lesions; however,
differentiating between thyroid cysts and PCs is challenging. FNAB
is a valuable diagnostic tool for the morphological evaluation of
solid or cystic thyroid and parathyroid lesions (13). The typical findings of a watery,
colorless crystal clear fluid are, in the majority of cases,
suggestive of the diagnosis of a non-functional PC. The diagnosis
may be established by elevated levels of PTH in the aspirated fluid
(14).
Clinically, no symptoms are usually associated with
PCs that are located in the parathyroid region and are not
excessively large or causing compression of the adjacent tissue.
Therefore, PCs tend to be large at the initial identification. In
the present study, the cyst caused dyspnea in the patient as a
result of marked tracheal deviation, and dysphagia due to
esophageal deviation.
Controversy exists regarding the treatment of PCs.
Until the 1970s, surgical treatment was considered to be the
optimal scheme (15). Since the
1970s, certain studies have indicated that FNAB is the preferred
management scheme due to the rarity of recurrence of PCs subsequent
to aspiration (16). By contrast, a
study by Sung et al stated that only 33% of non-functioning
lesions were successfully treated by a simple aspiration alone
(17). Similarly, Ujiki et al
reported that the majority of cysts recurred subsequent to
aspiration, and that surgery may be a more beneficial treatment
(18). However, to the best of our
knowledge, the treatment of non-functioning PCs may be considered
in association with the size of the cyst. In the present study, the
giant PC caused compressive symptoms; therefore, managing the PC
with surgical therapy was essential.
For PCs that extend to the mediastinum, common
surgical strategies include video-assisted thoracic surgery (VATS),
a standard posterolateral thoracotomy and the classical cervical
anterior approach. The VATS and posterolateral thoracotomy surgical
strategies were excluded for the present study due to the size of
the cyst and the surgical trauma that would be caused. In our
experience, the classical cervical anterior approach should be used
on PCs that are <10 cm in diameter. In order to reduce the
chance of relapse, the rupture of PCs should be prevented from
occurring intraoperatively. If necessary, a region of the
sternocleidomastoid muscle may be temporarily severed to avoid
rupture.
To the best of our knowledge, no associated
fatalities of treated patients have been documented in the previous
literature and the resection of giant PCs has rarely been
associated with post-operative complications (19).
In conclusion, the present study reported the case
of a man with a giant non-functional PC extending from the lower
neck to the superior mediastinum. Giant PCs are uncommon entities
in clinical practice that may manifest with compressive symptoms of
the surrounding tissues. The vast majority of PCs are
non-functioning. The diagnosis of a PC may be confirmed by the
detection of increased levels of PTH in the aspirated fluid, which
in the majority of non-functional PCs is a watery, colorless
crystal clear fluid. Surgery is the treatment of choice for giant
non-functioning PCs, and the classical cervical anterior approach
is recommended for use on PCs that are <10 cm in diameter.
References
|
1
|
Sandstrom I: Whether humans have multiple
thyroid lobes? Ups Lakafor Forhandl. 14:441–471. 1880.(In
Danish).
|
|
2
|
Goris D: Excise the third thyroid lobe.
Ann Soc Belg Chir. 5:394–400. 1905.(In French).
|
|
3
|
Mostafapour SP, True L and Futran ND:
Clinical problem solving: Pathology. Pathology quiz case: 1 Benign
parathyroid cyst. Arch Otolaryngol Head Neck Surg. 128:592–594,
594. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pinney SP and Daly PA: Parathyroid cyst:
An uncommon cause of a palpable neck mass and hypercalcemia. West J
Med. 170:118–120. 1999.PubMed/NCBI
|
|
5
|
Clark OH: Parathyroid cysts. Am J Surg.
135:395–402. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rosenberg J, Orlando R III, Ludwig M and
Pyrtek LJ: Parathyroid cysts. Am J Surg. 143:473–480. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ramos-Gabatin A, Young RL and Schenk D:
Parathyroid cyst: Medical diagnosis and therapy. South Med J.
75:1138–1140. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sen P, Flower N, Papesch M, Davis A and
Spedding AV: A benign parathyroid cyst presenting with hoarse
voice. J Laryngol Otol. 114:147–148. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
McCoy KL, Yim JH, Zuckerbraun BS, Ogilvie
JB, Peel RL and Carty SE: Cystic parathyroid lesions: Functional
and nonfunctional parathyroid cysts. Arch Surg. 144:52–56;
discussion 56. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cappelli C, Rotondi M, Pirola I, De
Martino E, Leporati P, Magri F, Rosei EA, Chiovato L and Castellano
M: Prevalence of parathyroid cysts by neck ultrasound scan in
unselected patients. J Endocrinol Invest. 32:357–359. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
McKay GD, Ng TH, Morgan GJ and Chen RC:
Giant functioning parathyroid cyst presenting as a retrosternal
goitre. ANZ J Surg. 77:297–304. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rossi ED, Revelli L, Giustozzi E, Straccia
P, Stigliano E, Lombardi CP, Pontecorvi A and Fadda G: Large
non-functioning parathyroid cysts: Our institutional experience of
a rare entity and a possible pitfall in thyroid cytology.
Cytopathology. 26:114–121. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fadda G and Rossi ED: Liquid-based
cytology in fine-needle aspiration biopsies of the thyroid gland.
Acta Cytol. 55:389–400. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ihm PS, Dray T, Sofferman RA, Nathan M and
Hardin NJ: Parathyroid cysts: Diagnosis and management.
Laryngoscope. 111:1576–1578. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pacini F, Antonelli A, Lari R, Gasperini
L, Baschieri L and Pinchera A: Unsuspected parathyroid cysts
diagnosed by measurement of thyroglobulin and parathyroid hormone
concentrations in fluid aspirates. Ann Intern Med. 102:793–794.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shi B, Guo H and Tang N: Treatment of
parathyroid cysts with fine-needle aspiration. Ann Intern Med.
131:797–798. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sung JY, Baek JH, Kim KS, Lee D, Ha EJ and
Lee JH: Symptomatic nonfunctioning parathyroid cysts: Role of
simple aspiration and ethanol ablation. Eur J Radiol. 82:316–320.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ujiki MB, Nayar R, Sturgeon C and Angelos
P: Parathyroid cyst: Often mistaken for a thyroid cyst. World J
Surg. 31:60–64. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shields TW and Immerman SC: Mediastinal
parathyroid cysts revisited. Ann Thorac Surg. 67:581–590. 1999.
View Article : Google Scholar : PubMed/NCBI
|