Introduction
Kidney squamous cell carcinomas are rare occurrences
in renal malignancies, particularly for kidney parenchyma squamous
cell carcinoma (1–5). To the best of our knowledge, only three
cases of patients with kidney parenchyma cell carcinoma have been
reported since December 2014 (2–5). The three
cases consisted of a 73-year old man (2), a 51-year old man (5) and a 60-year old woman (4). All the patients underwent nephrectomies.
The 73-year old man was followed up 3 months after surgery, the
51-year old man was followed up 6 and 12 months after surgery and
the 60-year old woman was followed up 13 months after surgery; all
patients remained alive with no evidence of disease at the time of
follow-up (2–5). The present study reports a case of
kidney parenchyma squamous cell carcinoma with inflammation
invasion, which mimicked xanthogranulomatous pyelonephritis on
radiological examination; the literature concerning kidney squamous
cell carcinomas is also reviewed.
Case report
A 61-year old man presented to the Second Xiangya
Hospital (Changsha, China) in October 2014 with right lumbago and
gross hematuria that had been present for nearly 2 months. The
patient had right renal parenchyma lithotomy ~14 years ago.
Physical examination demonstrated positive percussion pain on the
right kidney region. Palpation on the kidneys did not reveal any
pathological symptoms.
On admission, routine urine tests demonstrated that
the urine was clearly positive for white blood cells (WBCs) (WBC
count, 1,187.50/µl; normal range, 0–25/µl). C-Reactive protein
measured 72.20 mg/l (normal, <8 mg/l), erythrocyte sedimentation
rate was 81 mm/h (normal, <15 mm/h), procalcitonin was 3.23
ng/ml (normal, <0.05 ng/ml). Renal and liver function tests
results were within the normal ranges. Urine cytology examination
demonstrated massive epithelial cells and neutrophils without
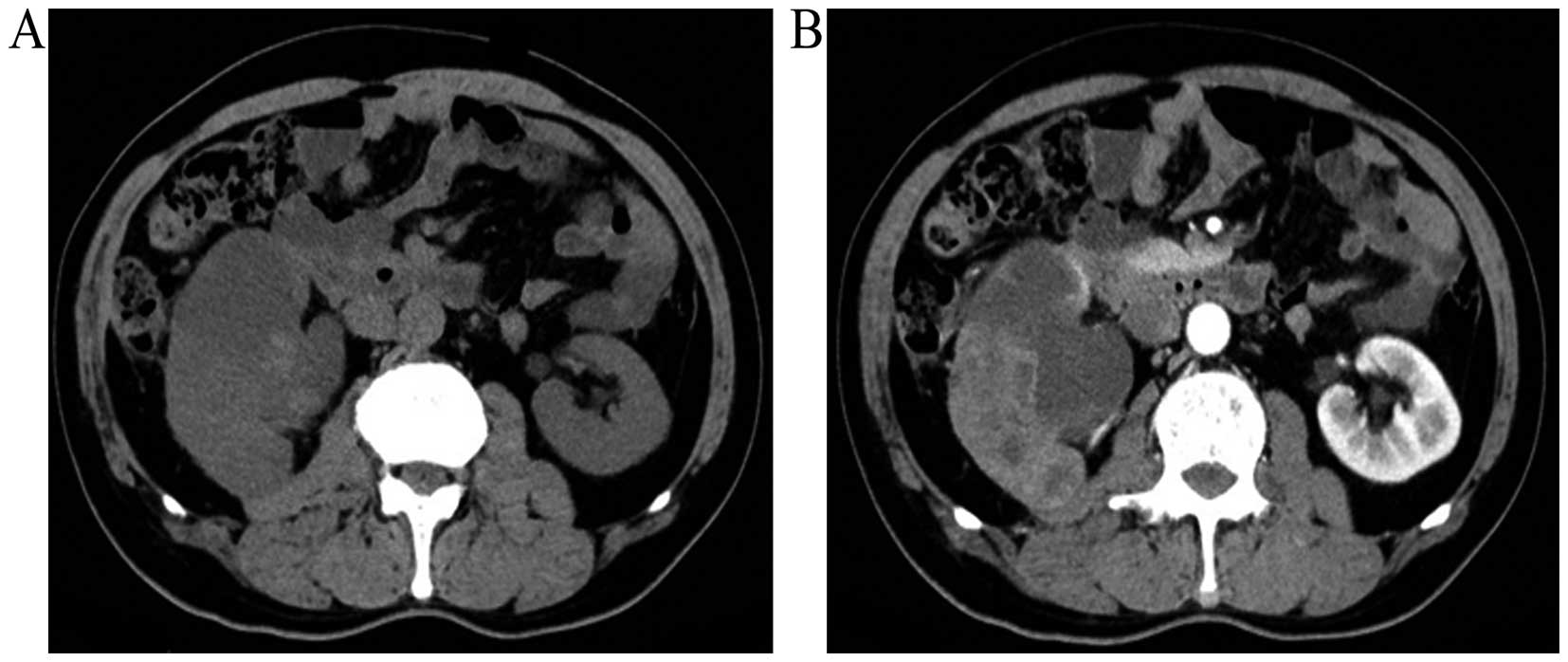
malignancies. Contrast-enhanced computed tomography (CT) was
performed using a SOMATOM Sensation CT scanner (Siemens, Munich,
Germany). It demonstrated enlargement of the right kidney with
abnormal morphology and dilatation of the ureter, multiloculated
cyst-like masses with soft tissues, and perirenal fatty space was
fuzzy (Fig. 1A and B). The lesions
observed on the CT scan were atypical and were considered as
xanthogranulomatous pyelonephritis or tuberculosis; however, the
presence of a rare renal tumor could not be completely excluded.
Tuberculosis tests [purified protein derivative
(PPD)-immunoglobulin (Ig)M, PPD-IgG and MycoDot] were performed and
were negative.
In total, 10 days following admission, the patient
had a fever (highest temperature, 39.6°C) and chills, and blood
rountine tests demonstrated a white blood cell count of
16.94×109 cells/l (normal range,
3.50–9.50×109 cells/l) and a neutrophil percentage of
92.34% (normal range, 40.00–75.00%). Therefore, physicians
hypothesized that the patient had septicemia. Antibiotics were
prescribed (latamoxef for 2 week, 1 g twice a day, intravenous
combined with moxifloxacin for 5 days, 0.4 g once a day,
intravenous), which were adjusted (imipenem cilastatin sodium, 0.5
g every 6 h, intravenous) according to a routine blood test
(procalcitonin and C-reactive protein) and a routine urine
examination, including color, glucose and protein concentration, pH
and white and red blood cell count, urine culture and advice from
clinical pharmacists. After septicemia was controlled in the
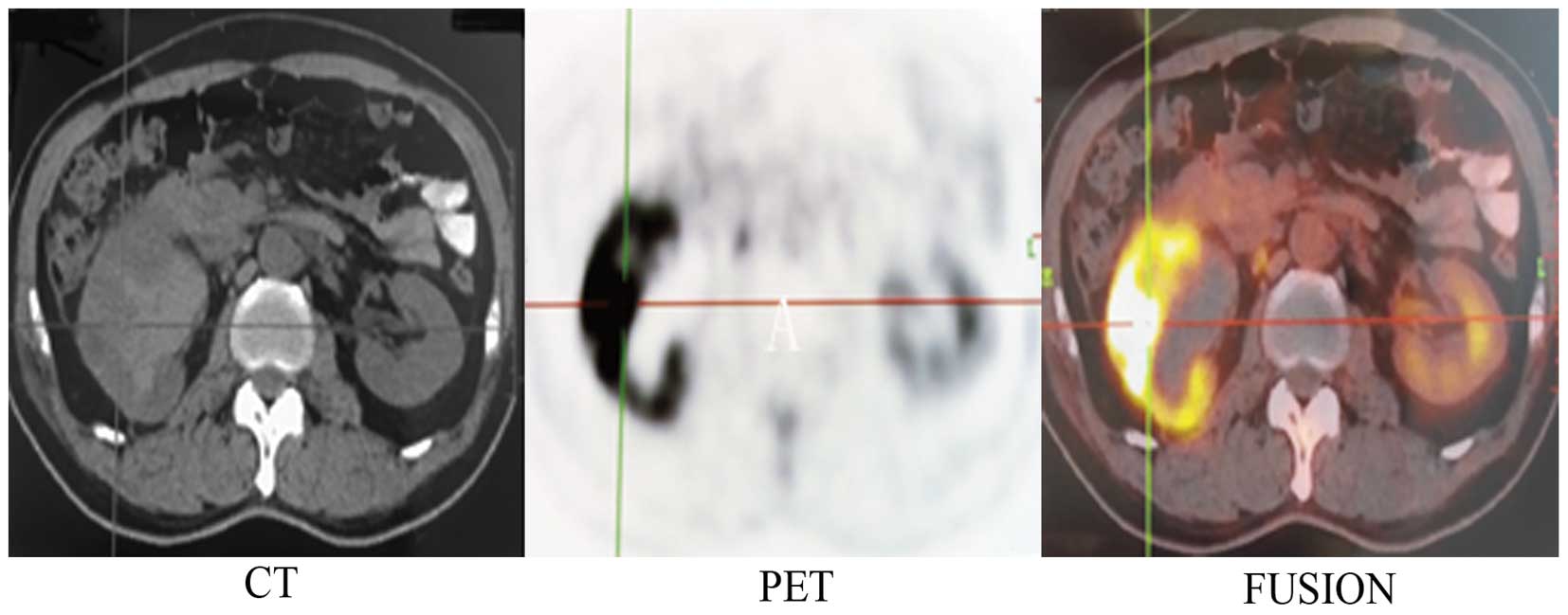
patient, cystoscopy was performed. Fludeoxyglucose-positron
emission tomography (FDG-PET; Biography mCTx; Siemens) was also
performed following the administration of 9.43 mCi FDG. Cystoscopy
did not reveal the presence of carcinoma in the bladder and
urethra. FDG-PET showed hydronephrosis with a fuzzy perirenal fatty
space, and valid FDG was taken up by cystic-solid mixed masses in
the right kidney (Fig. 2). The
lesions were considered to be renal malignancies, but renal
inflammation diseases could not be excluded completely.
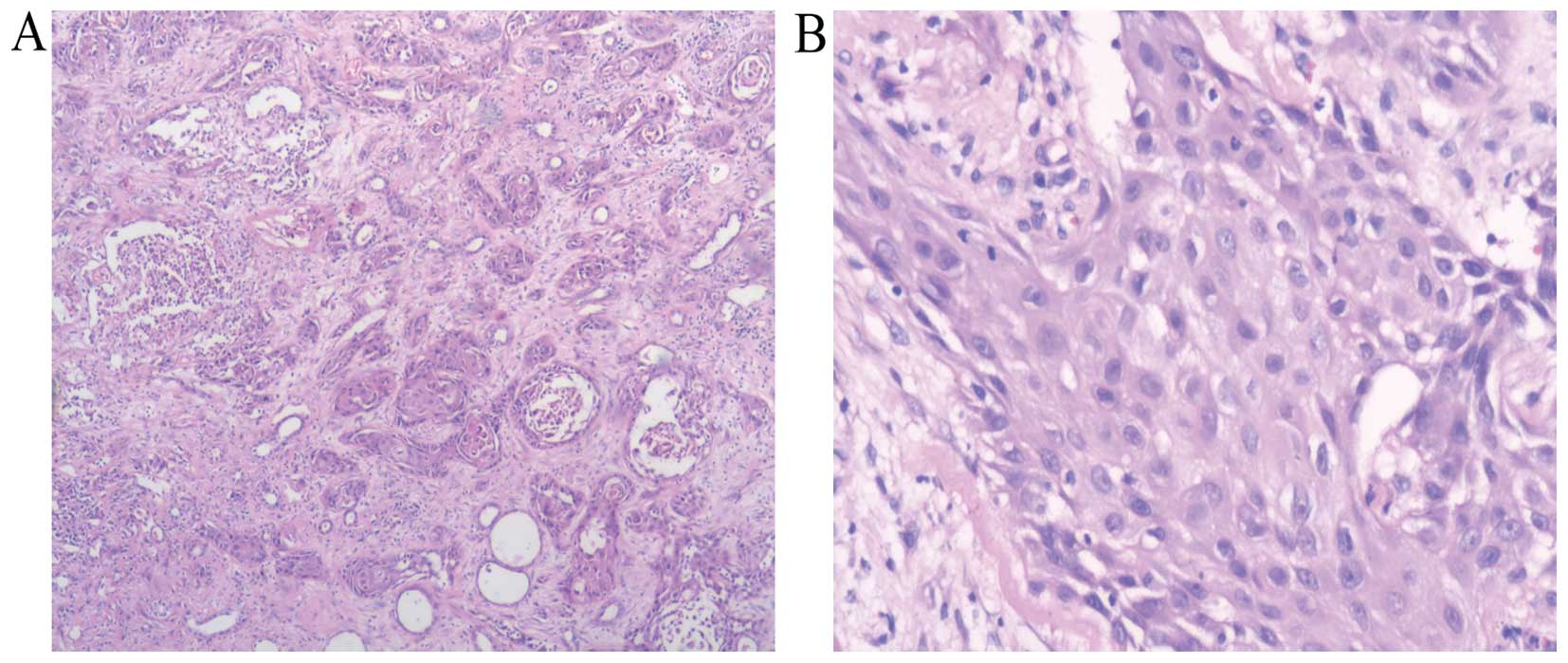
Right radical nephrectomy was performed.
Histological examination using hematoxylin and eosin staining
(Sinopharm Chemical Reagent Co., Ltd., Shanghai China) on
paraffin-embedded tissues under a microscope (BX51TF; Olympus
Corporation, Tokyo, Japan) demonstrated moderate-differentiated
squamous cell carcinoma of the renal parenchyma with a massive
invasion of inflammatory cells (Fig. 3A
and B). The patient was discharged 10 days following surgery.
Follow-up one month after surgery in December 2014 showed that the
patient had no febrile, gross hematuria or abnormal abdominal
signs. Written informed consent was obtained from the patient for
the publication of the present study.
Discussion
Kidney squamous cell carcinomas are rare renal
malignancies, and are classified as renal parenchyma and pelvic
squamous cell carcinomas according to where they arise. Primary
kidney pelvic squamous cell carcinomas account for 0.5–0.8% in
kidney malignancies (1). Renal
parenchyma squamous cell carcinomas are extremely rare; to the best
of our knowledge only 3 cases have been reported until now
(2–5).
Urinary calculi and chronic inflammation are some of
the important factors associated with renal squamous cell
carcinomas (4,5). In the present case, the patient has a
history of kidney calculi for >14 years and surgery was
performed to remove the stone. The patient exhibited chronic
urinary inflammation and antibiotics were intermittently
prescribed. These are two predisposing factors associated with the
development of squamous cell carcinomas (4–5).
Ultrasound and CT are important tools to evaluate
masses in renal malignancies. Xanthogranulomatous pyelonephritis,
secondary malignancies should be taken into account in order to
achieve a differential diagnosis for renal masses (1). In the present case, contrast-enhanced CT
revealed the presence of lesions in the right kidney. According to
the patient's history and primary blood and urine tests,
xanthogranulomatous pyelonephritis was one of the most consistent
diagnosis. Difficulties exist in evaluating primary renal masses
and achieving differential diagnosis in radiological examinations
prior to surgery due to the nonspecific features of these lesions
(6).
FDG-PET/CT has been verified as an effective tool in
diagnosis, preoperative and prognosis evaluation in renal tumors
(7,8).
A meta-analysis previously demonstrated that the sensitivity and
specificity of FDG-PET for renal lesions are 62 and 88%,
respectively; however, sensitivity and specificity increase to 84
and 91% for extra-renal lesions (9).
FDG-PET is reportedly more consistent in detecting extra-renal
lesions than renal lesions (9). In
the present case, FDG-PET/CT was performed prior to surgery. Since
the kidney has an abnormal structure and if invasive inflammation
has occurred, it is difficult to make a definite diagnosis prior to
surgery. Sometimes renal benign diseases resemble renal
malignancies, such as acute pyelonephritis, xanthogranulomatous
pyelonephritis or inflammatory pseudotumors on FDG-PET/CT (10–12).
Maximum standardized uptake value
(SUVmax) in FDG-PET/CT is a potential measurement that
may be used to evaluate patients' survival in renal cell carcinoma
(8). For the patient in the present
case, the SUVmax of the early image was 19.9, and 33.8
in the delayed image. According to Ferda et al (8) 12 month-mortality rate may be as high as
62.5%. Follow-up for the patient is therefore extremely
important.
Primary kidney parenchyma squamous cell carcinoma is
rare. The present study introduces a case of primary kidney
parenchyma squamous cell carcinoma in a 61-year old man, which was
initially diagnosed as xanthogranulomatous pyelonephritis on CT. In
addition, FDG-PET/CT did not distinguish renal inflammation
diseases from various types of tumors in the present case. Right
radical nephrectomy was performed, and histological diagnosis
determined a case of kidney parenchyma squamous cell carcinoma with
inflammation invasion. The 1 year mortality for this case may reach
as high as 62.5% according to the SUVmax. In conclusion,
FDG-PET/CT is critical in assisting with the diagnosis and
prognosis evaluation in kidney malignancies.
References
|
1
|
Kalayci OT, Bozdag Z, Sonmezgoz F and
Sahin N: Squamous cell carcinoma of the renal pelvis associated
with kidney stones: Radiologic imaging features with gross and
histopathological correlation. J Clin Imaging Sci. 3:142013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Terada T: Synchronous squamous cell
carcinoma of the kidney, squamous cell carcinoma of the ureter and
sarcomatoid carcinoma of the urinary bladder: A case report. Pathol
Res Pract. 206:379–383. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pusiol T, Zorzi MG and Morini A: Comment
on: Primary squamous cell carcinoma of the renal parenchyma. Indian
J Pathol Microbiol. 56:702013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kulshreshtha P, Kannan N, Bhardwaj R and
Batra S: Primary squamous cell carcinoma of the renal parenchyma.
Indian J Pathol Microbiol. 55:370–371. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ghosh P and Saha K: Primary
intraparenchymal squamous cell carcinoma of the kidney: A rare and
unique entity. Case Rep Pathol. 2014:2568132014.PubMed/NCBI
|
|
6
|
Bhaijee F: Squamous cell carcinoma of the
renal pelvis. Ann Diagn Pathol. 16:124–127. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Oyama N, Ito H, Takahara N, Miwa Y, Akino
H, Kudo T, Okazawa H, Fujibayashi Y, Komatsu K, Tsukahara K and
Yokoyama O: Diagnosis of complex renal cystic masses and solid
renal lesions using PET imaging: Comparison of 11C-acetate and
18F-FDG PET imaging. Clin Nucl Med. 39:e208–e214. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ferda J, Ferdova E, Hora M, Hes O, Finek
J, Topolcan O and Kreuzberg B: 18F-FDG-PET/CT in potentially
advanced renal cell carcinoma: A role in treatment decisions and
prognosis estimation. Anticancer Res. 33:2665–2672. 2013.PubMed/NCBI
|
|
9
|
Wang HY, Ding HJ, Chen JH, Chao CH, Lu YY,
Lin WY and Kao CH: Meta-analysis of the diagnostic performance of
[18F]FDG-PET and PET/CT in renal cell carcinoma. Cancer Imaging.
12:464–474. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
McCammack KC, Hawkes NC, Silverman ED and
Paz DA: PET/CT appearance of acute pyelonephritis. Clin Nucl Med.
38:e299–e301. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cheng G, Torigian DA and Alavi A: FDG
PET/CT and MRI findings in a patient with focal xanthogranulomatous
pyelonephritis mimicking cystic renal malignancy. Clin Nephrol.
76:484–486. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lee JH, Lee KG, Park HK, Song SY, Kim JY,
Kim YH, Choi YY, Jang KS and Park MH: Inflammatory pseudotumor of
the kidney mimicking malignancy on 18F-FDG PET/CT in a patient with
diabetes and hepatocellular carcinoma. Clin Nucl Med. 37:699–701.
2012. View Article : Google Scholar : PubMed/NCBI
|