Introduction
The most common kidney cancer is renal cell
carcinoma (RCC), which accounts for 2–3% of all types of cancer
worldwide (1). The prognosis of RCC
varies according to the stage and histological grade of the tumor,
and with genetic profiling and technological improvements, the
classification of RCC has expanded. In the 2004 World Health
Organization classification of renal tumors, RCC associated with
Xp11.2 translocation/transcription factor enhancer 3 (TFE3) fusion
gene (Xp11.2 translocation RCC) is described as a distinct type of
RCC (2). Xp11.2 translocation RCC is
diagnosed primarily in children, where it accounts for 30% of
pediatric RCC cases; however, RCC translocations have recently been
observed in adults, who have a poorer prognosis compared with
children (3). This type of RCC is
characterized by a range of chromosome translocations, each of
which consists of a breakpoint at Xp11.2 and a fusion involving the
TFE3 gene. The current study describes the case of a 14-year-old
boy who presented with chest pain that had persisted for 1 month. A
kidney neoplasm was incidentally located using computed tomography
(CT). The type of RCC may usually be diagnosed according to the
pathology of the tumor, and no unique treatment of RCC,
particularly the Xp11.2 translocation, exists. Therefore, surgical
treatment was used in the present study, based on the
characteristics of the tumor, including its size and adhesion with
the surrounding tissue. The present study also reviewed the
literature concerning Xp11.2 translocation RCC, in order to improve
the diagnosis and treatment of this rare disease.
Case report
A previously healthy 14-year-old male presented to
Department of Urology, Peking University Shenzhen Hospital,
(Shenzhen, China) on July 13, 2014, with chest pain that had
persisted for 1 month. The patient had no significant medical
history, no family history of cancer and did not smoke or drink
alcohol. A physical examination was negative, but a urine occult
blood test was positive. An ultrasound revealed the presence of a
solid mass in the left kidney, with a mean diameter of 6.0×5.4 cm.
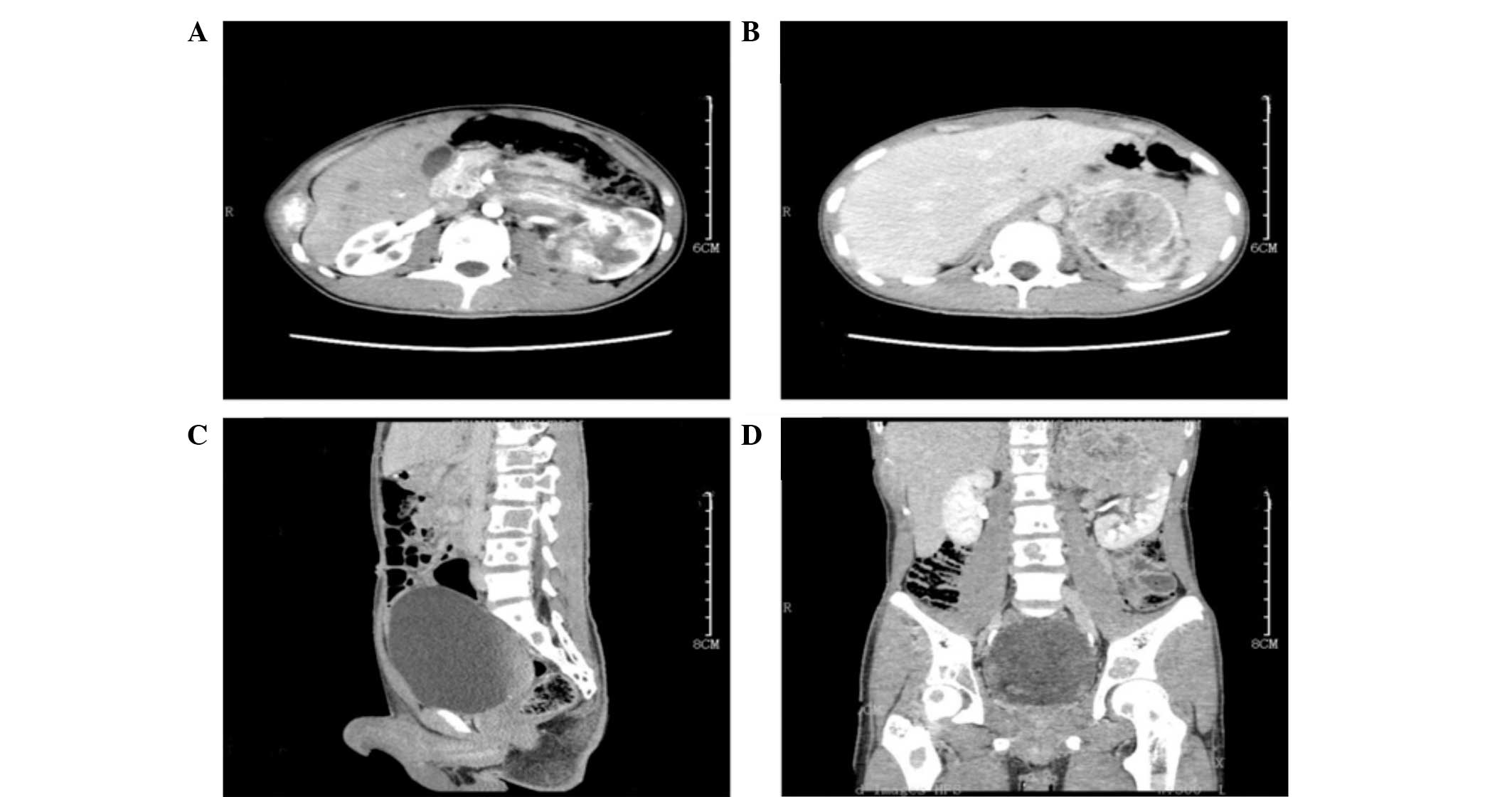
Abdominal contrast-enhanced CT (Sensation 16 MDCT scanner; Siemens
Healthcare, Erlangen, Germany) demonstrated the presence of a solid
mass in the left kidney, with uneven enhancement (Fig. 1A and B). In addition, there was
destruction of multiple bones, including the vertebrae, pelvis and
bilateral femoral head (Fig. 1C and
D). A left radical nephrectomy and partial ureterectomy were
performed.
Intraoperatively, the left kidney was clearly
enlarged and severe adhesions were observed. The surrounding fat
tissues were easily identified. Macroscopically, the ill-defined
tumor was located in the upper pole of the resected kidney and
measured 7.0×7.0×4.5 cm in size. There were several sporadic tumor
nodules, with a mean diameter of 3.0 mm, which were all
well-circumscribed. The gross appearance of the tumor was yellow,
hemorrhagic and necrotic, which is similar to the appearance of
conventional RCC (4).
The formalin-fixed, paraffin-embedded tissue (4 µm
pathological section) was used for immunohistochemical analysis
with the primary antibody TFE3 (clone P-16; goat anti-human
polyclonal antibody; cat. no. sc-5958; Santa Cruz Biotechnology,
Santa Cruz, CA, USA), according to the manufacturer's overnight
incubation methodology. The tumor was stained with hematoxylin and
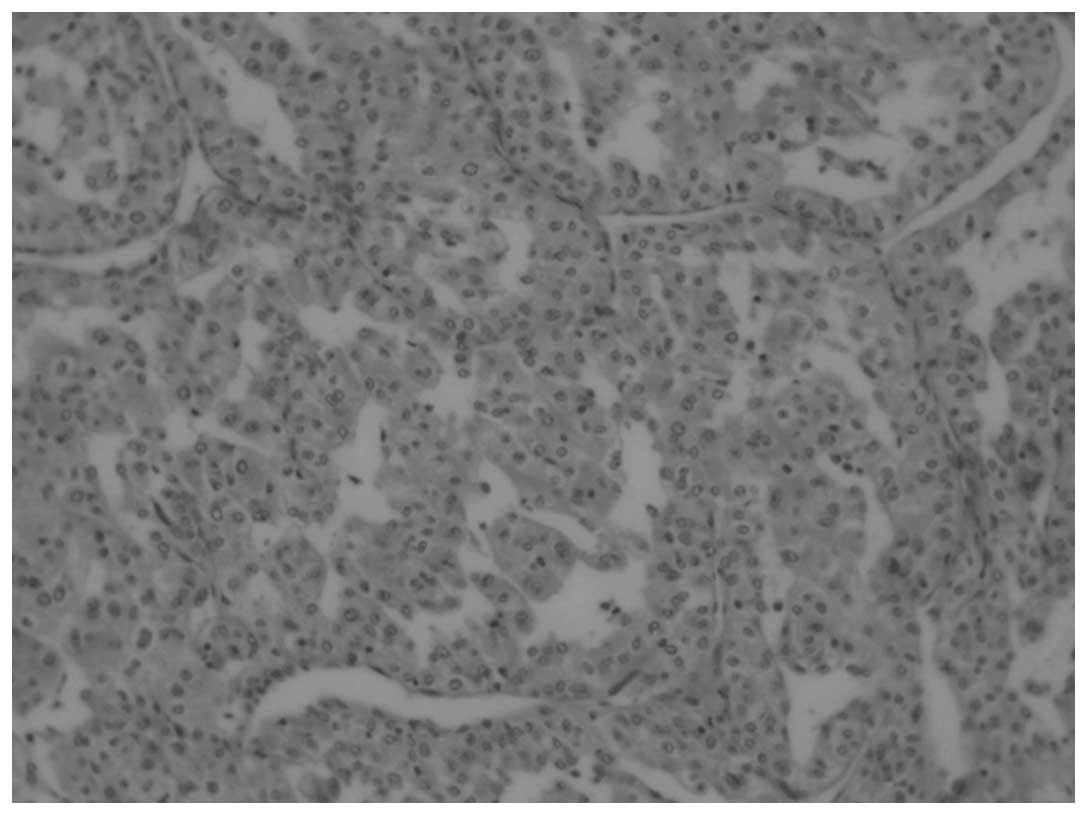
eosin. Microscopically, the tumor was composed of cells arranged in
primarily papillary patterns, with abundant clear to eosinophilic
cytoplasm and prominent nucleoli (Fig.
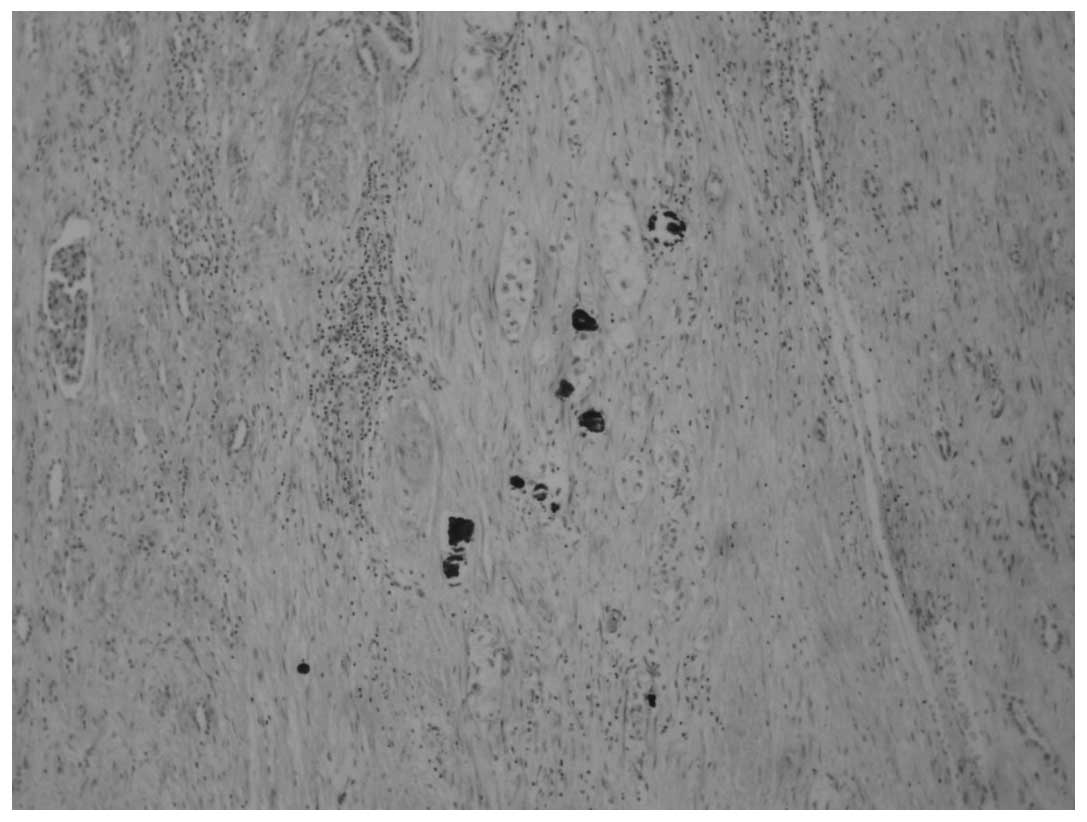
2). Psammoma bodies were frequently observed (Fig. 3). Hemorrhage, necrosis and multifocal
calcifications were also clearly observed in the tumor. None of the
hilar lymph nodes exhibited neoplastic infiltration.
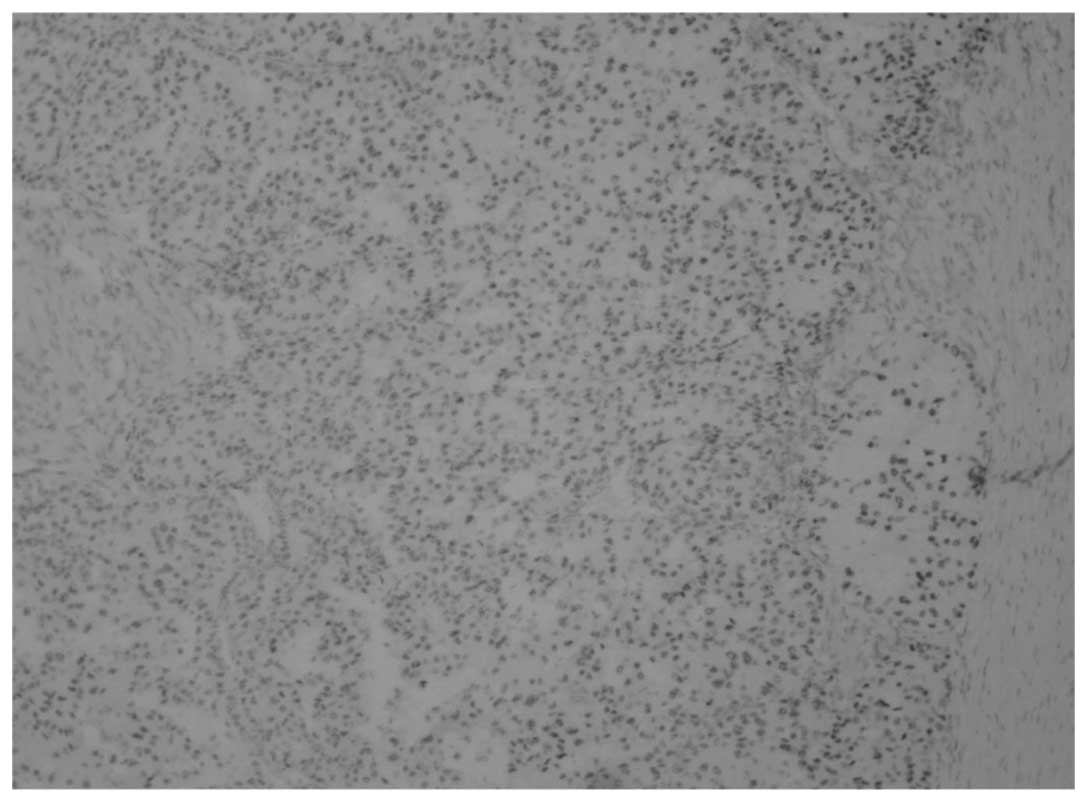
Immunohistochemistry demonstrated that the
neoplastic cells clearly and diffusely expressed TFE3 (Fig. 4) and cluster of differentiation 10,
and focally expressed P504S, pan-cytokeratin, vimentin, carbonic
anhydrase IX and kidney-specific cadherin. The patient was
diagnosed with Xp11.2 translocation RCC and multiple bone
metastases.
Following the surgery, the patient was transfered to
another hospital to receive further treatment, the detail of which
is unknown. However, the patient's family informed the Department
of Urology, Peking University Shenzhen Hospital, that the patient
succumbed 6 months later.
Discussion
Xp11.2 translocation RCC is characterized by several
translocations that involve the TFE3 gene, which is located on
chromosome Xp11.2, and leads to genic fusions. There are 5 gene
partners of TFE3, including papillary renal cell carcinoma
(translocation-associated) (PRCC), alveolar soft part sarcoma
chromosome region, candidate 1 (ASPL), splicing factor
proline/glutamine-rich (PSF), non-POU domain containing,
octamer-binding and clathrin, heavy chain, which are located on
1q21, 17q25, 1p34, Xq12 and 17q23, respectively. The most common
translocations are t(X;17)(p11.2;q25), t(X;1)(p11.2;p34) and
t(X;1)(p11.2;q21), which result in gene fusions of TFE3 with ASPL,
PSF and PRCC, respectively (3,5,6).
Macroscopically, Xp11.2 translocation RCC is
heterogeneous. The tumors are usually tan-yellow or grey-white,
necrotic and hemorrhagic, which is similar to the appearance of
classic RCC. The most distinctive histopathological appearance is
the papillary and nested architecture that is composed of a
voluminous clear to eosinophilic cytoplasm, prominent nucleoli,
vesicular chromatin, discrete cell borders, scattered hyaline
nodules and psammoma bodies (7–9). Tumors of
the PRCC-TFE3 fusion gene are usually composed of
intermediate-sized cells and exhibit few psammoma bodies. By
contrast, tumors of the ASPL-TFE3 fusion gene exhibit voluminous
cells that are often dyscohesive and have an alveolar and
pseudopapillary architecture, hyaline nodules and extensive
psammoma bodies, which is similar to the characteristics observed
in the present case (6–8,10).
Diagnosing Xp11.2 translocation RCC from other types
of RCC that are often observed in patients, such as clear cell RCC
and papillary RCC, is relatively uncomplicated due to several
important defining characteristics. First, the majority of Xp11.2
translocation RCC cases occur in children. While RCC accounts for
5% of pediatric renal tumors, Xp11.2 translocation RCC may account
for >33%. Therefore, the presence of RCC in a child or young
adult may indicate Xp11.2 translocation RCC (11). Although Xp11.2 translocation RCC has
been recently reported in adults, it remains uncommon, which may
lead to these tumors being misdiagnosed as clear cell or papillary
RCC. Second, the histological characteristics observed with Xp11.2
translocation RCC may differentiate the tumor from non-classical
RCC, including tumor cells with a voluminous cytoplasm in a
papillary arrangement. Third, using anti-TFE3 antibodies in
immunohistochemistry may lead to the correct diagnosis; XP11.5
translocation RCC is confirmed by the detection of chromosome
translocation involving the TFE3 gene at Xp11.2 using various
methods.
In the current case, the patient possessed with an
aggressive tumor. The patient originally presented with a long-term
history of chest pain, and a solid mass was detected in the kidney,
with multiple bone destruction, by CT. Therefore, we hypothesize
that the tumors developed when the patient was younger or in
childhood, and were not observed until the masses become large and
were at an advanced stage. The treatment of the patient was
primarily surgical. Chemotherapy should be a treatment of choice;
however, its affect in advanced-stage Xp11.2 translocation RCC is
poor. In addition, Kmetec and Jeruc (9) reported the case of a patient with
recurrent tumors following surgery for Xp11.2 translocation RCC.
The patient was administered with sunitinib and everolimus (a
mechanistic target of rapamycin inhibitor), but no effective
response resulted. Furthermore, certain studies have demonstrated
that prior administration of chemotherapy may be a risk factor for
developing translocation carcinomas (12). Therefore, the advantages and
disadvantages of chemotherapy in patients with Xp11.2 translocation
RCC should be evaluated prior to administration.
To relieve the severe clinical outcome that is
associated with Xp11.2 RCC, early detection, accurate diagnosis and
close follow-up are required. Prior to the development of radical
nephrectomy there was no effective surveillance method for Xp11.2
translocation RCC. Klaassen et al (13) recommended aggressive follow-up with
regular physical examination, laboratory tests, and chest and
abdominal CT, for up to 10 years duration. Furthermore, since
Xp11.2 translocation RCC is often diagnosed in young adults, the
study proposed lifelong follow-up with a yearly physical
examination, laboratory tests, and chest and abdominal imaging
subsequent to the completion of the 10-year follow-up.
Xp11.2 translocation RCC is a newly described, but
rarely encountered subtype of RCC. It normally presents with
specific morphogenetic characteristics and biological behavior. The
detection of TFE3 expression using immunohistochemistry appears to
be an easy and useful technique to identify this type of tumor.
However, genetic analysis is required to elucidate the type of gene
fusion.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81101922) and the
Science and Technology Development Fund Project of Shenzhen (grant
nos. JCYJ20130402114702124 and JCYJ20150403091443329).
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lopez-Beltran A, Scarpelli M, Montironi R
and Kirkali Z: 2004 WHO classification of the renal tumors of the
adults. Eur Urol. 49:798–805. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Argani P and Ladanyi M: Translocation
carcinomas of the kidney. Clin Lab Med. 25:363–378. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ross H, Martignoni G and Argani P: Renal
cell carcinoma with clear cell and papillary features. Arch Pathol
Lab Med. 136:391–399. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Armah HB and Parwani AV: Xp11.2
translocation renal cell carcinoma. Arch Pathol Lab Med.
134:124–129. 2010.PubMed/NCBI
|
|
6
|
Argani P and Ladanyi M: Renal carcinomas
associated with Xp11.2 translocations/TFE3 gene fusions. In: World
Health Organization Classification of Tumours. Pathology and
Genetics of Tumours of the Urinary System and Male Genital Organs.
Eble JN, Sauter G, Epstein JI and Sesterhenn IA: (Lyon). IARC
Press. 37–38. 2004.
|
|
7
|
Argani P, Antonescu CR, Illei PB, Lui MY,
Timmons CF, Newbury R, Reuter VE, Garvin AJ, Perez-Atayde AR,
Fletcher JA, et al: Primary renal neoplasms with the ASPL-TFE3 gene
fusion of alveolar soft part sarcoma: A distinctive tumor entity
previously included among renal cell carcinomas of children and
adolescents. Am J Pathol. 159:179–192. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Argani P, Lal P, Hutchinson B, Lui MY,
Reuter VE and Ladanyi M: Aberrant nuclear immunoreactivity for TFE3
in neoplasms with TFE3 gene fusions: A sensitive and specific
immunohistochemical assay. Am J Surg Pathol. 27:750–761. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kmetec A and Jeruc J: Xp 11.2
translocation renal carcinoma in young adults; recently classified
distinct subtype. Radiol Oncol. 48:197–202. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Argani P, Antonescu CR, Couturier J,
Fournet JC, Sciot R, Debiec-Rychter M, Hutchinson B, Reuter VE,
Boccon-Gibod L, Timmons C, et al: PRCC-TFE3 renal carcinomas:
Morphologic, immunohistochemical, ultrastructural and molecular
analysis of an entity associated with the t(X;1)(p11.2;q21). Am J
Surg Pathol. 26:1553–1566. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schinstine M, Filie AC, Torres-Cabala C,
Abati A, Linehan WM and Merino M: Fine-needle aspiration of a
Xp11.2 translocation/TFE3 fusion renal cell carcinoma metastatic to
the lung: Report of a case and review of the literature. Diagn
Cytopathol. 34:751–756. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Argani P, Laé M, Ballard ET, Amin M,
Manivel C, Hutchinson B, Reuter VE and Ladanyi M: Translocation
carcinomas of the kidney after chemotherapy in childhood. J Clin
Oncol. 24:1529–1534. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Klaassen Z, Tatem A, Burnette JO, Donohoe
JM and Terris MK: Adult Xp11 translocation associated renal cell
carcinoma: Time to recognize. Urology. 80:965–968. 2012. View Article : Google Scholar : PubMed/NCBI
|