Introduction
Adipose tissue is widely distributed throughout the
human body. Thus, lipomas may originate almost anywhere in the body
and represent one of the most common benign neoplasms of the soft
tissues (1). Synovial lipomatosis,
which derives its name from Hoffa's disease, is also known as
villous lipomatous proliferation of the synovium or lipoma
arborescens (2). Synovial lipomatosis
is a rare disorder of the synovium, which results in joint pain,
swelling and effusion, and to date only a small number of cases
have been reported in the literature (3–5). The
disease is generally identified in the knee joints, with a lower
predilection for other joints (4),
such as the elbows, shoulders and wrists (5). However, cases of synovial lipomatosis in
the hindfoot (6) and peroneal tendon
sheaths (7) have been reported. No
cases of synovial lipomatosis in the metatarsophalangeal joints
have been reported thus far. In the present study, a case of
synovial lipomatosis occurring in the metatarsophalangeal joints of
the left hallux is presented, and the results of imaging and
histological examinations are discussed. Written informed consent
was obtained from the patient for the publication of this
study.
Case report
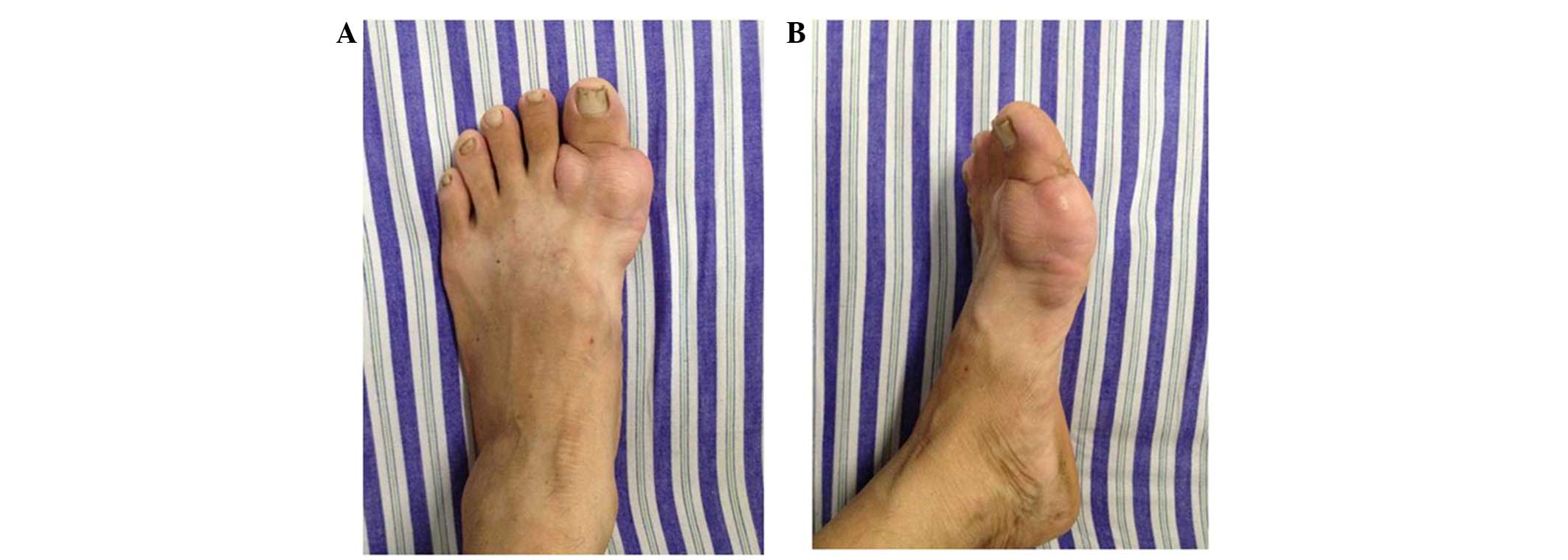
A 44-year-old male presented to The First Affiliated
Hospital of Nanchang University (Nanchang, China) in August 2011
with recurrent swelling of the metatarsophalangeal joints of the
left hallux, which had persisted for ~3 years. The patient had
found a mass surrounding the left hallux 3 years prior to
presentation, which had gradually increased in size. The patient
had no history of joint disorders, trauma or general disease. Upon
physical examination, a non-tender, boggy soft-tissue mass was
palpable on the metatarsophalangeal joints of the left hallux
(Fig. 1). The mass was soft, mobile
and well-defined. No erythema was identified, the area was not hot
to touch and the blood supply to the left foot was normal.
Laboratory routine blood tests were also negative. B-mode
ultrasonography performed at another hospital prior to admission to
The First Affiliated Hospital of Nanchang University showed a
thickened soft-tissue lesion surrounding the metatarsophalangeal
joints, which was diagnosed as chronic synovial hyperplasia.
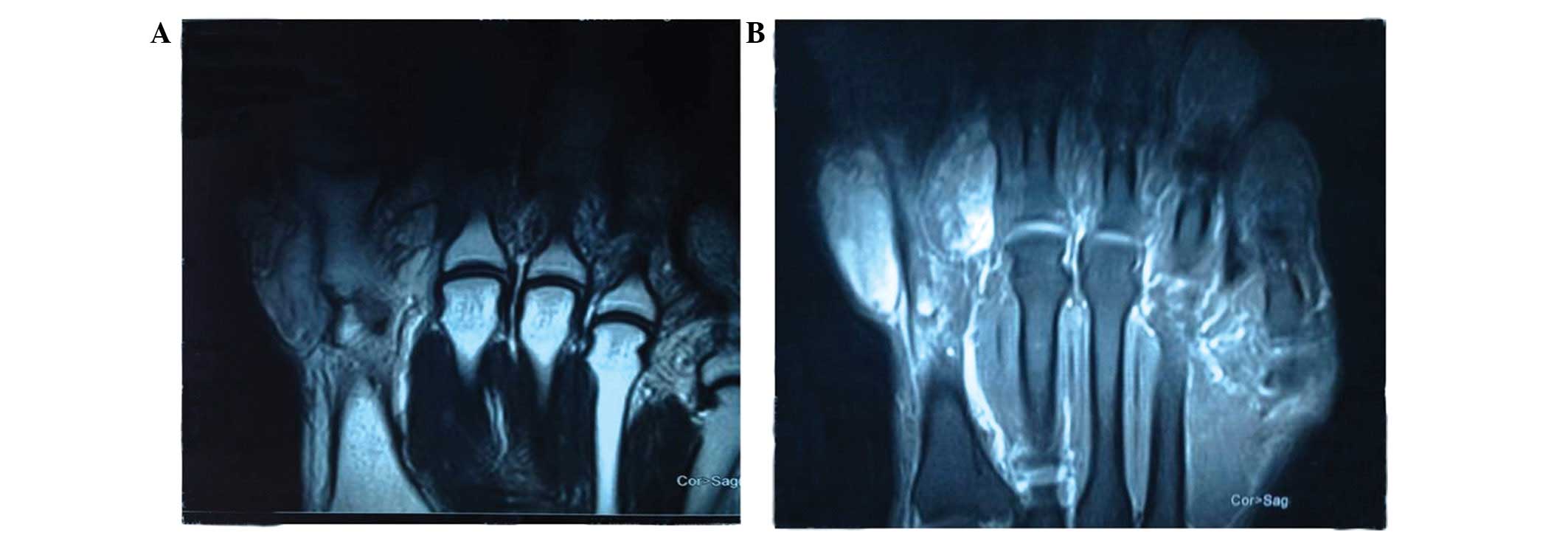
An amorphous tumor surrounding the first metatarsal
bone of the left hallux was identified on magnetic resonance
imaging (MRI) (Fig. 2), which
exhibited intermediate signal intensity on T1-weighted images
(Fig. 2A) and a signal intensity
similar to that of subcutaneous adipose tissue on T2-weighted
images (Fig. 2B). These findings were
consistent with a diagnosis of a giant cell tumor of the tendon
sheath. In addition, no evident abnormalities of left foot bone
signals were identified. The lesion was completely resected and
sent for histopathological examination.
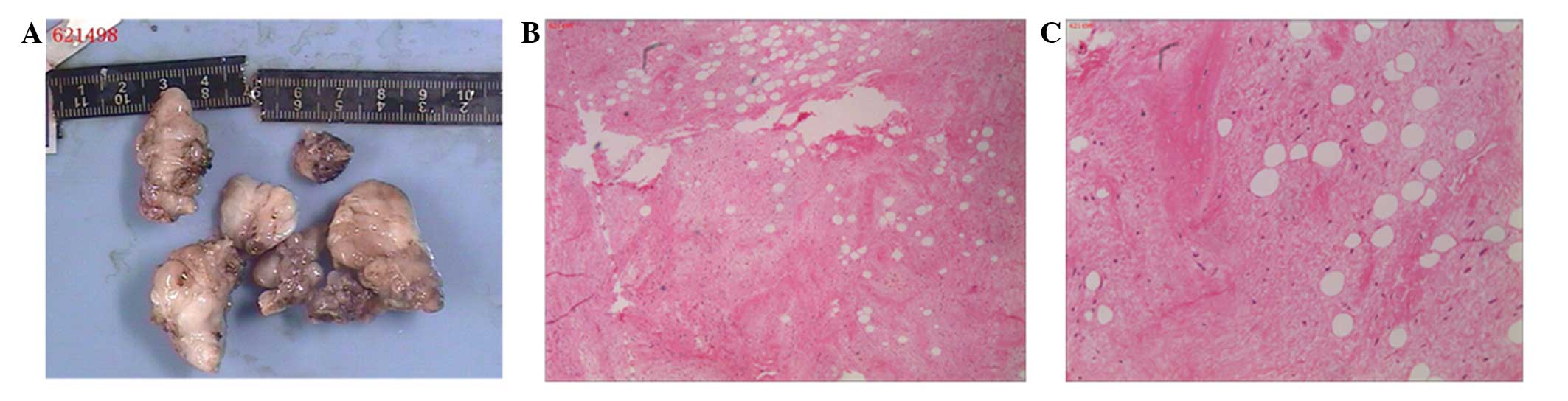
Histopathological analysis of the resected tissue
revealed a hoary, soft, nodular tissue mass, which was 7×5×2 cm in
size (Fig. 3A). Pathological
examination revealed well-defined lobules of mature adipocytes
separated by fibrous septa and covered by synovial lining (Fig. 3B), and extensive proliferation of the
fibrous and adipose tissues, with infiltration of chronic
inflammatory cells (Fig. 3C). The
color of the neoplasm was different to the yellow tissue normally
observed with giant cell tumors of the tendon sheath. Thus, based
on the results of pathological analysis, a final diagnosis of
synovial lipomatosis was established. A follow-up examination two
years after surgery revealed no disease recurrence and the patient
exhibited good hallux function.
Discussion
Lipoma, which exhibits no gender predilection, is a
common tumor-like lesion of the synovium that accounts for ~50% of
soft-tissue tumors (8). According to
the previously published literature, synovial lipomatosis most
commonly occurs in older individuals, with a median age of 50 years
(range, 39–66 years) (9). Although
the etiology of synovial lipomatosis remains unclear, a high body
mass index appears to exhibit a vital role in cases of short bowel
syndrome with synovial lipomatosis in multiple joints (10), and the clinical manifestations are
usually a result of the mass, and include pain, crepitus,
limitation of motion and joint effusion (1). The diagnosis of synovial lipomatosis is
achieved primarily by MRI, using adipose tissue-suppressed
sequences in particular; synovial lipomas and adipose tissue
exhibit similar high signal intensities on T1- and T2-weighted
images (1,11). As their treatment and prognosis
differ, it is important to differentiate synovial lipoma from other
adipose tissue proliferative diseases, including pigmented
villonodular synovitis, synovial chondromatosis, synovial
hemangiomatosis and rheumatoid arthritis (12). Pigmented villonodular synovitis
exhibits diffuse signals of low intensity on T1- and T2-weighted
images. Synovial chondromatosis varies from low to high signal on
T2- and T1-weighted sequences according to the cartilaginous
components of the lesion. Synovial hemangiomas exhibit intermediate
signal intensity on T1- and T2-weighted images, with areas of high
signal intensity due to the presence of fibrous septa between the
vascular channels and adipose tissue in the lesion. Rheumatoid
arthritis exhibits intermediate to low signal intensity on T1- and
T2-weighted images, and is associated with the formation of fibrous
pannus (12).
Surgical treatments for synovial lipomatosis include
arthroscopy and excision (5), and
treatment choice is dependent on the extent of involvement.
Arthroscopy is the preferred treatment choice for cases of synovial
lipomatosis, particularly in larger joints that exhibit low
recurrence rates, as it is minimally invasive with good recovery
rates (5,13). However, in certain cases, more
extensive surgeries, including arthrotomy and synovectomy, may be
required (14,15). The histomorphology of synovial
lipomatosis is associated with adipocyte metaplasia and
inflammation, and fibrosis (16);
thus, synovial lipomatosis can be more accurately described as the
process of overgrowth and infiltration of mature adipose tissue
within the synovium. Occasionally, fibrous septa may be visible
between the vascular channels and adipose tissue within the lesion
(17).
In the present case, the pre-operative clinical
manifestation and clinical examination indicated a diagnosis of a
giant cell tumor of tendon sheath. However, the resected surgical
specimens were gray, whereas the sheaths of giant cell tumors are
usually pale yellow, and thus, based on the results of MRI and the
pathological examination, the tumor was diagnosed as a synovial
lipoma.
In conclusion, synovial lipomatosis is an extremely
rare lesion of the synovium that is considered to occur as a result
of inappropriate adipose tissue deposition and degenerative
articular diseases of the joints. In this study, a rare case of
synovial lipomatosis involving the metatarsophalangeal joints was
presented. Increased understanding with regard to the
characteristic MRI features and distinct histomorphology of
synovial lipomatosis may lead to advances in the diagnosis of this
rare disease.
Acknowledgements
This study was supported by the Gan-Po Talents
Project 555 of Jiangxi Province.
References
|
1
|
Zhu W, Wang W, Chen Y and Xiao T: Synovial
lipoma in intra-patellar fat pad of the knee joint. Pak J Med Sci.
28:228–230. 2012.
|
|
2
|
Saddik D, McNally EG and Richardson M: MRI
of Hoffa's fat pad. Skeletal Radiol. 33:433–444. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pudlowski RM, Gilula LA and Kyriakos M:
Intraarticular lipoma with osseous metaplasia:
Radiographic-pathologic correlation. AJR Am J Roentgenol.
132:471–473. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bejia I, Younes M, Moussa A, Said M, Touzi
M and Bergaoui N: Lipoma arborescens affecting multiple joints.
Skeletal Radiol. 34:536–538. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yildiz C, Deveci MS, Ozcan A, Saraçoğlu
HI, Erler K and Basbozkurt M: Lipoma arborescens (diffuse articular
lipomatosis). J South Orthop Assoc. 12:163–166. 2003.PubMed/NCBI
|
|
6
|
Jowett C, Mitra P, O'Donnell P and Singh
DS: Synovial lipomatosis of hindfoot tendon sheaths: Case reports
and literature review. Foot Ankle Int. 29:752–755. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vinson EN, Dodd LG, Merian M and Martinez
S: Synovial lipomatosis arborescens of the peroneal tendon sheath.
Skeletal Radiol. 37:947–950. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Samarjit K, Budhiraja S,
Chandramouleeswari K and Anita S: Knee locking in osteoarthritis
due to synovial lipoma: A case report. J Clin Diagn Res.
7:1708–1709. 2013.PubMed/NCBI
|
|
9
|
Kakkar N, Vasishta RK and Anand H:
Pathological case of the month. Synovial lipomatosis. Arch Pediatr
Adolesc Med. 153:203–204. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Siva C, Brasington R, Totty W, Sotelo A
and Atkinson J: Synovial lipomatosis (lipoma arborescens) affecting
multiple joints in a patient with congenital short bowel syndrome.
J Rheumatol. 29:1088–1092. 2002.PubMed/NCBI
|
|
11
|
Ku JH, Cho HL, Park JT, Wang TH and Yang
HS: Intra-articular synovial lipoma in the posteromedial
compartment of the knee. Arthrosc Orthop Sports Med. 1:54–58. 2014.
View Article : Google Scholar
|
|
12
|
Vilanova JC, Barceló J, Villalón M, Aldomà
J, Delgado E and Zapater I: MR imaging of lipoma arborescens and
the associated lesions. Skeletal Radiol. 32:504–509. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hirano K, Deguchi M and Kanamono T:
Intra-articular synovial lipoma of the knee joint (located in the
lateral recess): A case report and review of the literature. Knee.
14:63–67. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ren F and Li Z: Diagnosis and therapy of
synovial lipomatosis of the knee joint. Chin J Orthop. 29:539–543.
2009.
|
|
15
|
Haasbeek JF and Alvillar RE: Childhood
lipoma arborescens presenting as bilateral suprapatellar masses. J
Rheumatol. 26:683–686. 1999.PubMed/NCBI
|
|
16
|
Franco M, Puch JM, Carayon MJ, Bortolotti
D, Albano L and Lallemand A: Lipoma arborescens of the knee: Report
of a case managed by arthroscopic synovectomy. Joint Bone Spine.
71:73–75. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rao S, Rajkumar A, Elizabeth MJ, Ganesan V
and Kuruvilla S: Pathology of synovial lipomatosis and its clinical
significance. J Lab Physicians. 3:84–88. 2011. View Article : Google Scholar : PubMed/NCBI
|