Introduction
Radioactive rays are known to damage the human body,
causing conditions such as malignant tumours. Studies have
demonstrated that the exposure of healthy tissue to harmful
radiation during radiation therapy may lead to an acute radiation
reaction or cancer, particularly leukaemia (1). Clear evidence of a dose-dependent risk
of chronic myeloid leukaemia (CML), especially in people exposed to
radiation at a young age, has been reported (2), and numerous studies on the association
between radiotherapy and CML have been published (3–5).
CML is characterized by the nonrandom, recurrent
Philadelphia chromosome (6), which is
present in ~90% of patients with CML (7). Philadelphia chromosome carries the
breakpoint cluster/Abelson murine leukemia viral oncogene homolog 1
fusion gene, which has been demonstrated to play a major role in
CML pathogenesis (8,9). The incidence of CML is ~0.36 out of
every 100,000 individuals in China (10). In recent years, more effective
techniques have been introduced as therapy for patients with CML,
including the use of interferon-α, allogeneic stem cell
transplantation and tyrosine kinase inhibitors (11). Currently, the prognosis of patients
CML is markedly improved compared to previous years. A previous
study, which used imatinib as a first-line treatment for newly
diagnosed patients with chronic phase CML, demonstrated that the
likelihood of succumbing to CML was almost equivalent to the
probability of succumbing to other diseases (12).
It is unclear, however, whether diagnostic radiation
increases the risk of CML, the incidence of which is ~0.36 out of
every 100,00 individuals in China. Case-control and retrospective
studies that have investigated the risk of developing CML in
patients exposed to diagnostic radiation have resulted in
contradictory data (13–15). The reported odds ratios for diagnostic
radiation-induced CML vary greatly, possibly due to the different
dosages of radiation exposure used in the different studies. To the
best of our knowledge, only one case of possible diagnostic
radiation-induced CML exists in the literature (13). Thus, robust evidence to support the
association between diagnostic radiation and CML is still lacking.
The present study reports the case of a patient who developed CML
subsequent to undergoing several diagnostic imaging tests for
recurrent pneumothorax.
Case report
On 6 May 2013, a 26-year-old man presented to the
Zhejiang Provincial Hospital of Traditional Chinese Medicine
(Hangzhou, China) with pneumothorax. The patient eventually
recovered from the condition on 3 June 2013; however, between 6 May
2013 and 3 June 2013, the patient was admitted as an in-patient to
the Zhejiang Provincial Hospital of Traditional Chinese Medicine
(Hangzhou, China) and the Linyi People's Hospital (Linyi, China) on
three occasions due to recurrent pneumothorax. He was treated with
closed thoracic drainage and underwent thoracoscopic surgery and
Bullae resection due to a relapse. Routine blood tests, bowel and
urine output, liver and kidney function, and tumour markers were
all normal. Viral hepatitis and human immunodeficiency virus
infection were also ruled out during the hospital visit.
During the first month of treatment (from the day of
the first occurrence of pneumothorax to the date of discharge
subsequent to surgery), the patient was exposed to eight chest
radiography examinations, comprising eight exposures in the
anteroposterior and two in the posteroanterior position.
Additionally, three chest computed tomography (CT) scans of the
entire body were performed at various hospitals. The effective
radiation dose of these imaging tests reached 9.6 mSv (16). Within the next 8 months, the patient
underwent two more chest radiography procedures (two exposures in
the anteroposterior and one in the posteroanterior position) and
one CT scan due to a cough and other discomfort. These added an
additional radiation dose of 2.1 mSv, yielding a total effective
dose of 11.7 mSv.
The patient was an employee of a large-scale
bookstore and lived in a normal environment, which had no serious
pollution, abnormal background radiation or other anomalies. He
denied exposure to toxic substances or contaminated water, alcohol
abuse or exposure to venereal disease. The patient's family
histories were normal, and none of his immediate family members had
cancer. The patient was slim and had a body mass index of 20.2
kg/m2. Physical examination revealed no remarkable
findings.
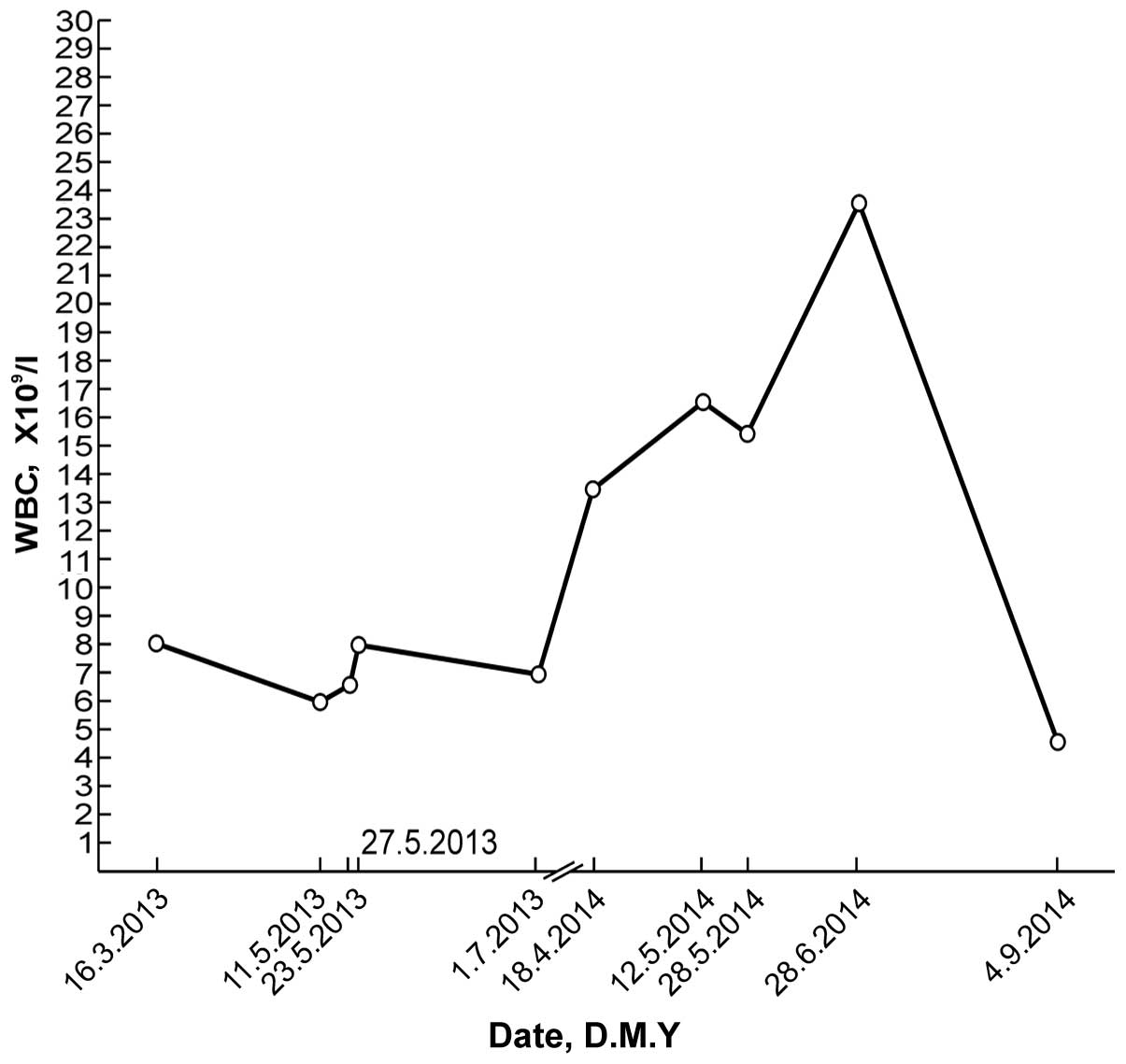
A routine blood test on 18 April 2014, during a
general health examination, revealed a white blood cell (WBC) count
of 13.9×109/l (normal range, 4–10×109/l) with
66.9% neutrophils (normal range, 50–70%), a red blood cell (RBC)
count of 5.25×1012/l (normal range,
4.5–5.5×1012/l) and a platelet (PLT) count of
335×109/l (normal range, 100–300×109/l). The
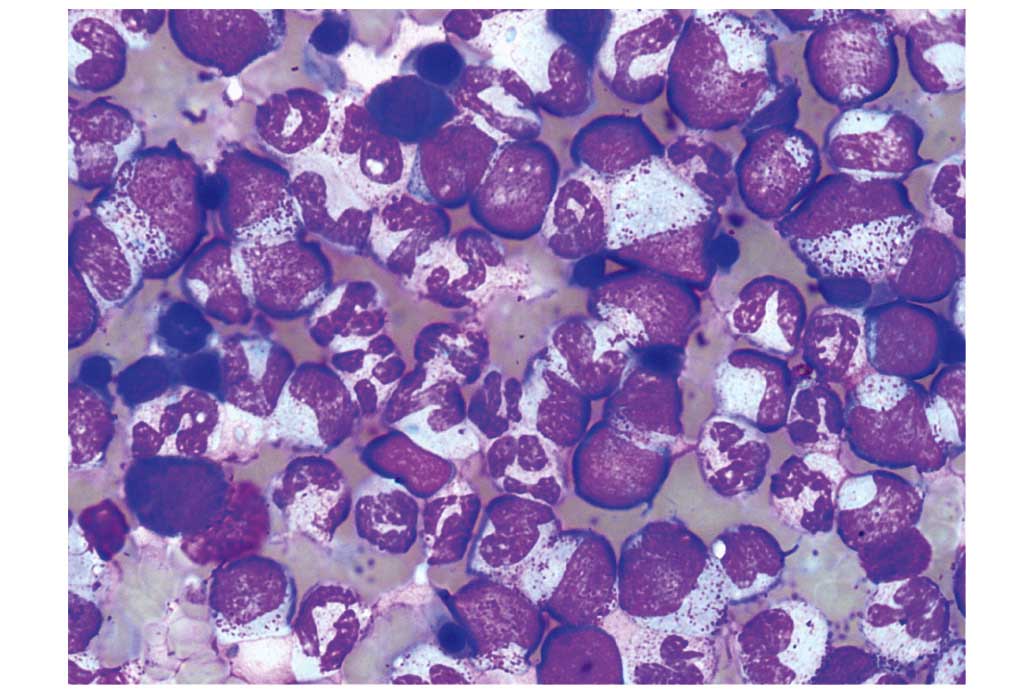
patient's WBC count subsequently increased significantly (Fig. 1). A bone marrow smear test, stained
with Wright-Giemsa (Zhuhai Baso Biotechnology Co., Ltd., Zhuhai,
China), was performed on 13 June 2014 and revealed bone marrow
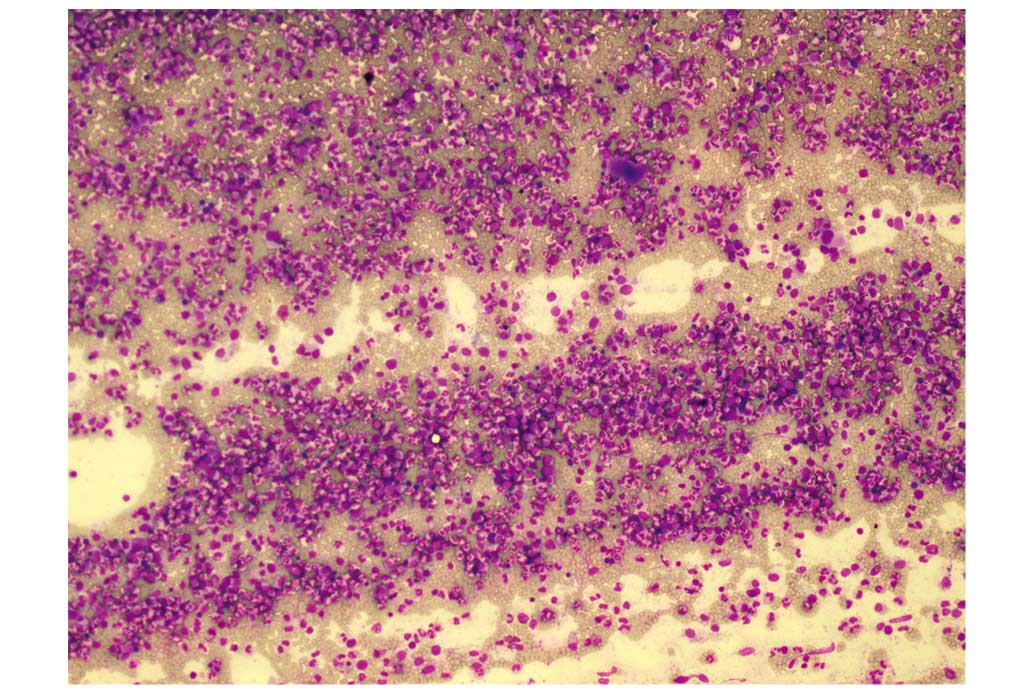
hematopoietic hyperactivity primarily with neutrophils (Fig. 2) and an abnormal increase in bone
marrow nucleated cells (Fig. 3). Bone
marrow biopsy core from the patient was fixed using Bouins fixative
solution (Sigma-Aldrich, St. Louis, MO, USA), dehydrated using
ethanol, plastic embedded (Hemapun 959; Beijing Xinxing Braim
Technology Co., Ltd., Beijing, China), sectioned (3-µm)using a
microtome (Microm HM340E; Microm International GmbH, Walldorf,
Germany) and stained with hematoxylin and eosin,
hematoxylin-Giemsa-fuchsin, Giemsa, improved toluidine blue,
periodic acid Schiff reagent and Gomori silver impregnation to
identify reticulin and collagen fibers (Zhuhai Baso Biotechnology
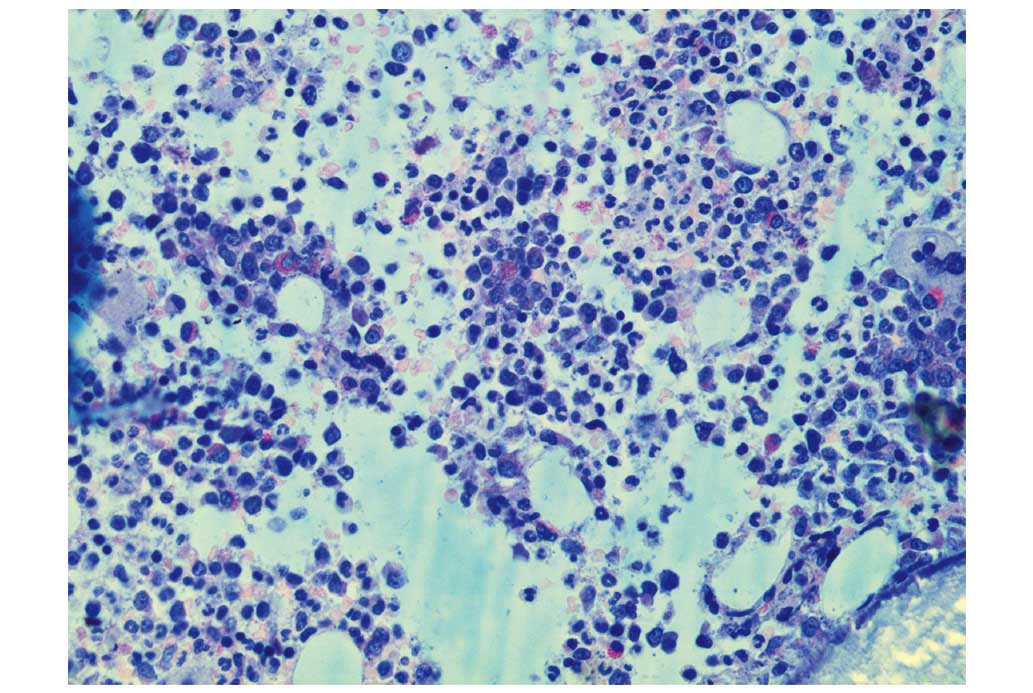
Co., Ltd.). Histological examination of the bone marrow using
toluidine blue staining demonstrated an increased number of
positively-stained basophils (Fig.
4), and a blood smear test revealed multiple circulating
immature granulocytes. A chromosome karyotype analysis (19 June
2014) revealed the following results: 46,XY,t(9;22)(q34;q11.2). The
qualitative breakpoint cluster region (BCR)/Abelson (ABL) gene test
revealed positive results for BCR/ABL p210 and negative results for
BCR/ABL p230. The negative control group yielded negative results
and the positive and internal control groups showed positive
results. All these results suggested CML. Hence, a diagnosis of CML
was made.
A repeat routine blood test (28 June 2014) revealed
a WBC count of 23.8×109/l with 73.8% neutrophils, an RBC
count of 4.89×1012/l and a PLT count of
507×109/l. Following the administration of oral imatinib
mesylate (400 mg/d for 68 days), the patient's leukocyte percentage
decreased to normal levels. Another repeat routine blood test (4
September 2014) revealed a WBC count of 4.6×109/l with
45.5% neutrophils, an RBC count of 3.72×1012/l and a PLT
count of 212×109/l. Changes in the patient's WBC values
over time are depicted in Fig. 1. The
patient continued to take imatinib mesylate until January 2015, and
experienced no obvious discomfort. The patient remains in
follow-up, and will undergo bone marrow cytology and chromosome
examination.
The institutional ethics committee of the Zhejiang
Provincial Hospital of Traditional Chinese Medicine approved the
current study.
Discussion
The current study reports a case of CML occurring in
a patient who had undergone repeated exposure to diagnostic chest
radiography and CT for pneumothorax. The patient appeared irritable
and slightly anxious during hospital visits. He had been a patient
of the hospital three times within one month due to his
pneumothorax. Irrespective of how he felt, he requested a
radiological examination (chest radiography or CT). Furthermore,
the patient always appeared to be in a hurry and was anxious to
achieve recovery in order to be discharged from the hospital. These
factors contributed to the decision of the doctors to perform
multiple chest radiography inspections in a fairly short space of
time.
The International Commission on Radiological
Protection (ICRP) recommends an effective maximum dose of
occupational X-ray exposure (in planned exposure situations) of 20
mSv/year when averaged over defined 5-year periods (100 mSv in 5
years) (17). Additionally, the
effective dose should not exceed 50 mSv in any single year.
However, the ICRP guidelines should not be applied to individual
patients, as they may reduce the effectiveness of the patient's
diagnosis or treatment, and should only be applied to personnel
engaged in radiation-associated industries (16). In consideration of a patient's anxiety
levels and to determine the causes and courses of their illnesses,
physicians often order numerous chest radiography and CT
procedures, as per the ICRP recommendation cited above. As a
result, patients frequently have repeated exposure to diagnostic
chest X-rays and CT radiation. The dose the present patient
received was <20 mSv; however, the patient was diagnosed with
CML. Therefore, even though the guidelines of the ICRP recommends
not to exceed 50 mSv, occasionally a lower dose may cause harm,
which radiologists must be made aware.
Although a number of case-control and retrospective
studies have investigated the risk of CML in patients exposed to
diagnostic radiation, their results have been contradictory
(13–15). One limitation of previous case-control
studies of leukaemia and its association with diagnostic
radiography was the lack of dosimetry. Evans et al (18) applied dose-response models to new data
on population exposure to radiographic procedures during a 1-year
period, and concluded that 1% of all leukaemia cases were caused by
diagnostic radiography. However, this study had limited information
on repeat examinations. To the best of our knowledge, only a single
case report presenting a possible cases of diagnostic
radiation-induced CML exists (13).
One report stated that a 19-year-old man with Ollier's disease who
underwent multiple orthopaedic procedures for leg length
discrepancy developed CML presenting with intramuscular haematoma.
In this case, the cumulative X-ray exposure of repeated surgeries
between the ages of 7 and 12 years was estimated to be around 16
mSv, which approximately equals the radiation dose of 720 chest
radiography procedures. The authors speculated that the repeated
radiation exposure, particularly due to the patient's young age and
the exposure of the marrow tissue of the long bones to radiation,
may have been an important pathogenetic factor for CML (13). The current case is different from this
case in numerous aspects. Firstly, although the patients were both
male, the patient in the present report was exposed to radiation as
an adult and within a shorter time frame. Additionally, the
radiation dosage in the current patient was lower, and the chest
was exposed to radiation, rather than the long bones as in the
previous case. The patient in the case report by Au et al
(13) possessed a Philadelphia
translocation, t(9;22;13)(q34;q11.2;q12), with a predominance of
neutrophil elastase (ela2) BCR/ABL splicing and deletion of the
reciprocal der(9) ABL/BCR locus. In
the present case, the qualitative BCR/ABL fusion gene (major
breakpoint) test performed on 19 June 2014 revealed positive
results for BCR/ABL p210 and negative results for BCR/ABL p230.
Collectively, these findings make the current case unique.
Cases of leukaemia occurring following the receipt
of radiological examinations have rarely been reported. A survey by
Sodickson et al (19)
conducted on 31,462 patients receiving CT examinations during 2007
assessed the lifetime attributable risks of radiation-induced
cancer from the cumulative radiation dosage using the reported
biological effect of ionizing radiation, based on the gender and
age of the study participants. The results revealed that CT
radiation dosage that accumulated over time could raise the
baseline for cancer risk in this patient population. The majority
of patients, however, exhibited a low risk of being diagnosed with
a radiation-induced tumour, and only a small number of patients
were at a potentially higher risk for cancer due to frequent CT
scans (19). It has been suggested
that this discrepancy could be associated with the patients'
individual differences in susceptibility to radiation. Indeed, the
ICRP has suggested that patients who are carriers of cancer genes
may be at risk of developing tumours as a result of radiation
therapy. In particular, in those who are already suffering from
cancer, radiation therapy may risk triggering a secondary tumour
(20). As stated on page 143 of the
ICRP Publication 103 (17),
‘including genetic susceptibility of strongly expressed genes to
radiation-induced cancer that are considered to be rare, which is
unlikely to cause any significant distortion to risk assessment of
the population; and the potential impact of the often seen weakly
expressed genes is still unknown’. Furthermore, the authors state
that ‘strongly expressed, highly susceptible cancer genes are
rarely seen. On this part, the report made the low dose radiation
cancer risk assessment based on population as a whole, which should
not be enough to cause significant distortions’ (16).
Other studies have demonstrated that the repair
capacity or fidelity of DNA and radiation sensitivity are
associated with racial diversity in humans (21). Studies have also reported that
radiation susceptibility causing increased cancer risk is polygenic
in nature. Radiation susceptibility- and normal tissue
toxicity-related genes and pathways include those for sensing DNA
damage, cell cycle checkpoints, intermediate protein recruitment,
repair pathways (base excision, homologous recombination and
non-homologous end joining), apoptosis, inflammatory cytokines,
fibrosis proteins, extracellular matrix, antioxidant enzymes,
cytokines, and growth factors (22).
However, it is still unknown whether individual sensitivity to
cancer caused by radiation actually exists, and if there is a
causal relationship between diagnostic radiation and cancer
(21). The issue of individual
susceptibility to genetic damage caused by diagnostic radiation is
a cause for concern and worthy of further discussion.
In clinical practice, making a diagnosis commonly
requires multiple radiological examinations or treatments. Although
it is not possible to be sure what role the current patient's
radiological examination played in his CML diagnosis, the case data
presented in this report are intended to increase awareness of the
potential harm of diagnostic radiation. Future in-depth studies
aimed at understanding individual susceptibility to the effects of
diagnostic radiation damage are warranted.
Acknowledgements
The authors wish to thank Editage (www.editage.cn/) for English language editing, and the
National Natural Science Foundation of China (Beijing, China; grant
no., 81400107) for supporting the present study.
References
|
1
|
Hall EJ and Giaccia AJ: Radiobiology for
the Radiologist (7th). Philadelphia: Wolters Kluwer
Health/Lippincott Williams & Wilkins. 273–302. 2012.
|
|
2
|
Tsushima H, Iwanaga M and Miyazaki Y: Late
effect of atomic bomb radiation on myeloid disorders: Leukemia and
myelodysplastic syndromes. Int J Hematol. 95:232–238. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ural AU, Beyzadeoglu M, Avcu F and Nevruz
O: Chronic myeloid leukemia following radiotherapy for carcinoma of
the cervix: Report of a case and brief review of the literature. Am
J Hematol. 82:415–416. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shimon I, Kneller A and Olchovsky D:
Chronic myeloid leukaemia following 131I treatment for thyroid
carcinoma: A report of two cases and review of the literature. Clin
Endocrinol (Oxf). 43:651–654. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Aguiar RC: Therapy-related chronic myeloid
leukemia: An epidemiological, clinical and pathogenetic appraisal.
Leuk Lymphoma. 29:17–26. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nowell PC and Hungerford DAS: A minute
chromosome in human chronic granulocytic leukemia. Science.
132:1497–1501. 1960.
|
|
7
|
Hochhaus A: Detection and quantification
of leukemia-specific rearrangements. Methods in Molecular Medicine™
Molecular Analysis of Cancer. Boultwood J and Fidler C: Humana
Press. (Totowa, NJ). 67–96. 2001. View Article : Google Scholar
|
|
8
|
Konopka JB, Watanabe SM, Singer JW,
Collins SJ and Witte ON: Cell lines and clinical isolates derived
from Ph1-positive chronic myelogenous leukemia patients express
c-abl proteins with a common structural alteration. Proc Natl Acad
Sci USA. 82:1810–1814. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Davis RL, Konopka JB and Witte ON:
Activation of the c-abl oncogene by viral transduction or
chromosomal translocation generates altered c-abl proteins with
similar in vitro kinase properties. Mol Cell Biol. 5:204–213. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang JY, Liao EY and Hu PJ: Leukemia.
Internal Medicine. People's Medical Publishing House. (Bejing).
756–757. 2005.(In Chinese).
|
|
11
|
Hughes T, Deininger M, Hochhaus A,
Branford S, Radich J, Kaeda J, Baccarani M, Cortes J, Cross NC,
Druker BJ, et al: Monitoring CML patients respongding to treatment
with tyrosine kinase inhibitors:review and recommendations for
harmonizing current methodology for detecting BCR-ABL transcripts
and kinase domain mutations and for expressing results. Blood.
108:28–37. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shah NP: Front-line TKI therapy for
chronic-phase CML: The luxury of choice. Oncology (Williston Park).
26:908, 910, 9122012.PubMed/NCBI
|
|
13
|
Au WY, Ooi GC, Ma SK, Wan TS and Kwong YL:
Chronic myeloid leukemia in an adolescent with Ollier's disease
after intensive X-ray exposure. Leuk Lymphoma. 45:613–616. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yuasa H, Hamajima N, Ueda R, Ohno R, Asou
N, Utsunomiya A, Ogura M, Takigawa N, Ueda T, Hiraoka A, et al:
Case-control study of leukemia and diagnostic radiation exposure.
Int J Hematol. 65:251–261. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Preston-Martin S, Thomas DC, Yu MC and
Henderson BE: Diagnostic radiography as a risk factor for chronic
myeloid and monocytic leukaemia (CML). Br J Cancer. 59:639–644.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
United Nations Scientific Committee on the
Effects of Atomic Radiation: Effects of ionizing radiation. UNSCEAR
2006 report. Report to the general assembly, with scientific
annexes. Annex A: Epidemiological studies of radiation and cancer.
United Nations. (New York). 13:3222006.
|
|
17
|
ICRP: The 2007 Recommendations of the
International Commission on Radiological Protection. ICRP
Publication 103. Ann ICRP. 37(2-4)2007.
|
|
18
|
Evans JS, Wennberg JE and McNeil BJ: The
influence of diagnostic radiography on the incidence of breast
cancer and leukemia. N Eng J Med. 315:810–815. 1986. View Article : Google Scholar
|
|
19
|
Sodickson A, Baeyens PF, Andriole KP,
Prevedello LM, Nawfel RD, Hanson R and Khorasani R: Recurrent CT,
cumulative radiation exposure, and associated radiation-induced
cancer risks from CT of adults. Radiology. 251:175–184. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
United Nations Scientific Committee on the
Effects of Atomic Radiation. Sources and effects of ionizing
radiation. UNSCEAR 1993 report. Report to the general assembly,
with scientific annexes. Annex F: Influence of dose and dose rate
on stochastic effects of radiation. (New York). United Nations.
619–728. 1993.
|
|
21
|
Sigurdson AJ and Stram DO: Genetic
predisposition to radiation-related cancer and potential
implications for risk assessment. Ann ICRP. 41:108–116. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Barnett GC, West CM, Dunning AM, Elliott
RM, Coles CE, Pharoah PD and Burnet NG: Normal tissue reactions to
radiotherapy: Towards tailoring treatment dose by genotype. Nat Rev
Cancer. 9:134–142. 2009. View
Article : Google Scholar : PubMed/NCBI
|