Introduction
Extragonadal choriocarcinoma is a rare malignancy
that occurs mainly in men, and accounts for 1–5% of all germ cell
malignancies (1,2). Chemotherapy, radiotherapy and surgery
are the primary therapeutic strategies for treating this disease;
however, a large number of patients rapidly succumb to the illness
(3–5).
A recent study stated that following surgery and chemotherapy the
median survival time of 13 male patients with extragonadal
choriocarcinoma was 54 months, which was higher than previously
expected (6). The most common primary
site is the mediastinum (7). The
majority of cases are characterized by multiple metastases at the
time of diagnosis, poor response to therapy and short survival
times (2,8,9). The
pathogenesis of extragonadal choriocarcinoma has long been debated
and is now focused on two hypotheses (2). One is that the tumor arises from
retained primordial germ cells that migrate abnormally during
embryogenesis (10). The other is
that the lesion originates from the transformation of a
nontrophoblastic neoplasm (11).
Serum β-human chorionic gonadotropin (β-HCG) is a
classic trophoblastic marker (12).
The levels of β-HCG, as assessed prior to chemotherapy, have been
integrated into the germ cell tumor classification (13). Normalization of high β-HCG levels is
generally associated with a good response to therapy (14). The present study describes the case of
a man with metastatic mediastinal choriocarcinoma, in which
biochemical remission was achieved by the combination of
chemotherapy and radiotherapy.
Case report
A 25-year-old man was admitted to the Department of
Medical Oncology, Hubei Cancer Hospital (Wuhan, Hubei, China) in
August 2013 with a month-long history of vomiting, heart
palpitations, chest pain and progressing dyspnea. The computed
tomography (CT) scan (SOMATOM Definition AS; Siemens AG, Munich,
Germany) of the thorax showed a large anterior mediastinal mass and
bilateral multiple rounded intrapulmonary lesions, which are
characteristic of metastatic tumors. The physical examination was
normal, with the exception of bilateral hypermastia. The testicles
were equal in size and without nodules or masses. In order to
elucidate the feature and distribution of the lesions, a
fluoro-2-deoxy-D-glucose (FDG) positron emission tomography
(PET)/CT scan (Discovery 16STE; GE Healthcare Life Sciences,
Chalfont, UK) was performed. The scan revealed increased FDG uptake
in the anterior mediastinal and lung lesions, with a maximal
standard uptake value of 8.4 and no extra lesions.
Laboratory data revealed a normal complete blood
cell count, and normal hepatic and renal function. However, the
levels of the serum tumor markers were elevated, with the exception
of carcinoembryonic antigen (1.20 µg/l), as follows: Serum β-HCG,
10883.2 IU/l (normal, <5 IU/l); α-fetoprotein (AFP), 23.1 ng/ml
(normal, <7 ng/ml); and lactate dehydrogenase (LDH), 462 U/l
(normal, <240 U/l). To avoid the risks associated with
mediastinal biopsy, including hemorrhage and rupture, an
ultrasonography-guided biopsy of the left lung mass was performed,
which revealed histological features of a cluster of atypical cells
near a small number of squamous epithelium cells, and muscle and
alveolar tissue, with the presence of cytotrophoblasts and
syncytiotrophoblasts.
Immunohistochemically, the tumor cells were positive
for HCG, pan-cytokeratin (CK) and CK7, and did not express cluster
of differentiation 117, prostatic acid phosphatase, CK5/6,
vimentin, leukocyte common antigen or thyroid transcription
factor-1. Based on these findings, a diagnosis of primary
mediastinal choriocarcinoma with diffuse lung metastasis was made.
The patient completed 8 cycles of standard combination chemotherapy
that consisted of etoposide [100 mg/m2, intravenous (IV)
drip d1-3], cisplatin (20 mg/m2, IV drip d1-5) and
bleomycin (20 mg/m2 intramuscular injection d1, d8, d15,
Q21d) (BEP) between September 2013 and April 2014, without
experiencing notable toxicity. Neutropenia grade I–III, according
to the National Cancer Institute-Common Terminology Criteria for
Adverse Events v3.0 (15), was the
main adverse effect experienced by the patient. During the
treatment period, the AFP level decreased to 2.36 ng/ml, which was
in the normal range, and β-HCG markedly decreased to 8.69 IU/l,
which was slightly higher than the normal upper limit. LDH
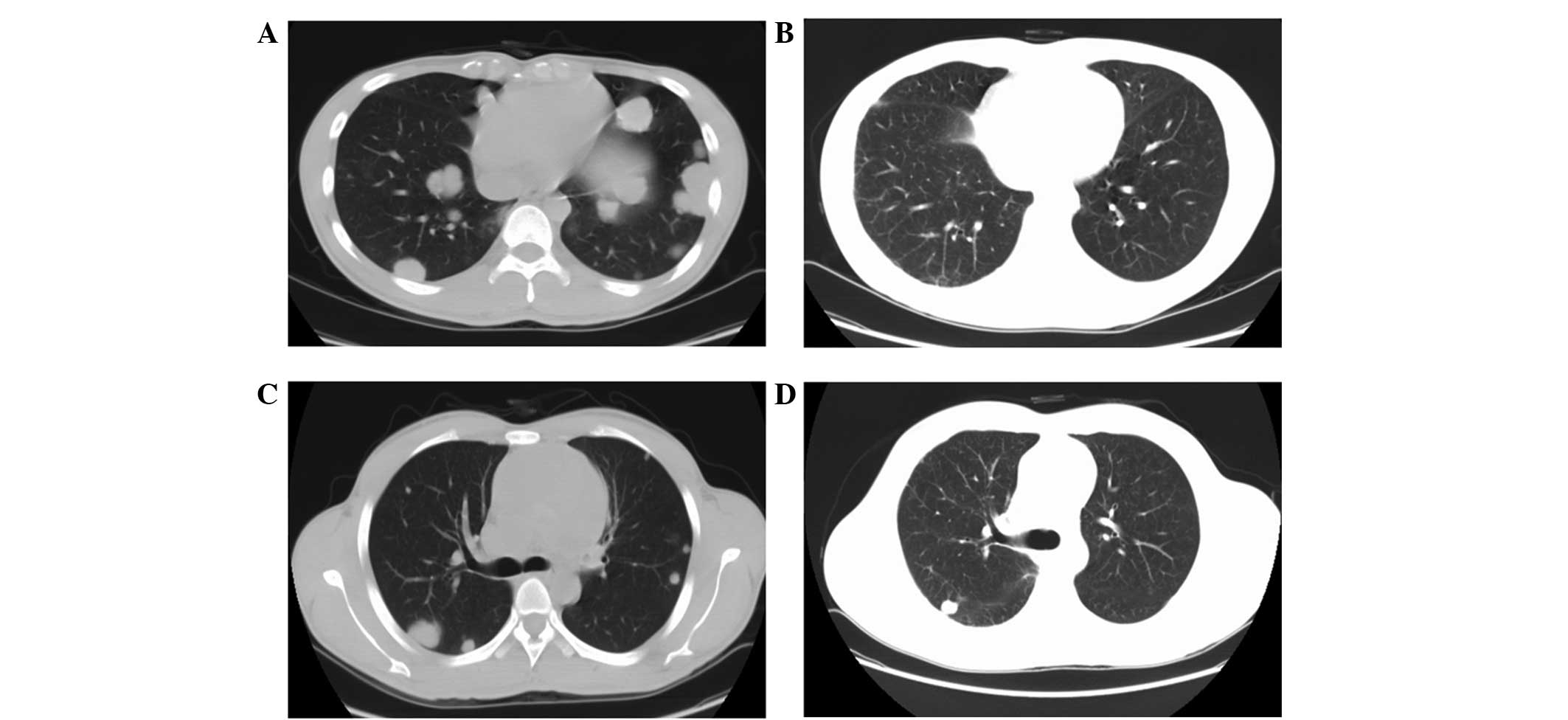
decreased to 144 U/l, which was in the normal range. Dynamic CT
evaluation revealed that the number and size of the lung lesions
was significantly reduced subsequent to 8 cycles of chemotherapy
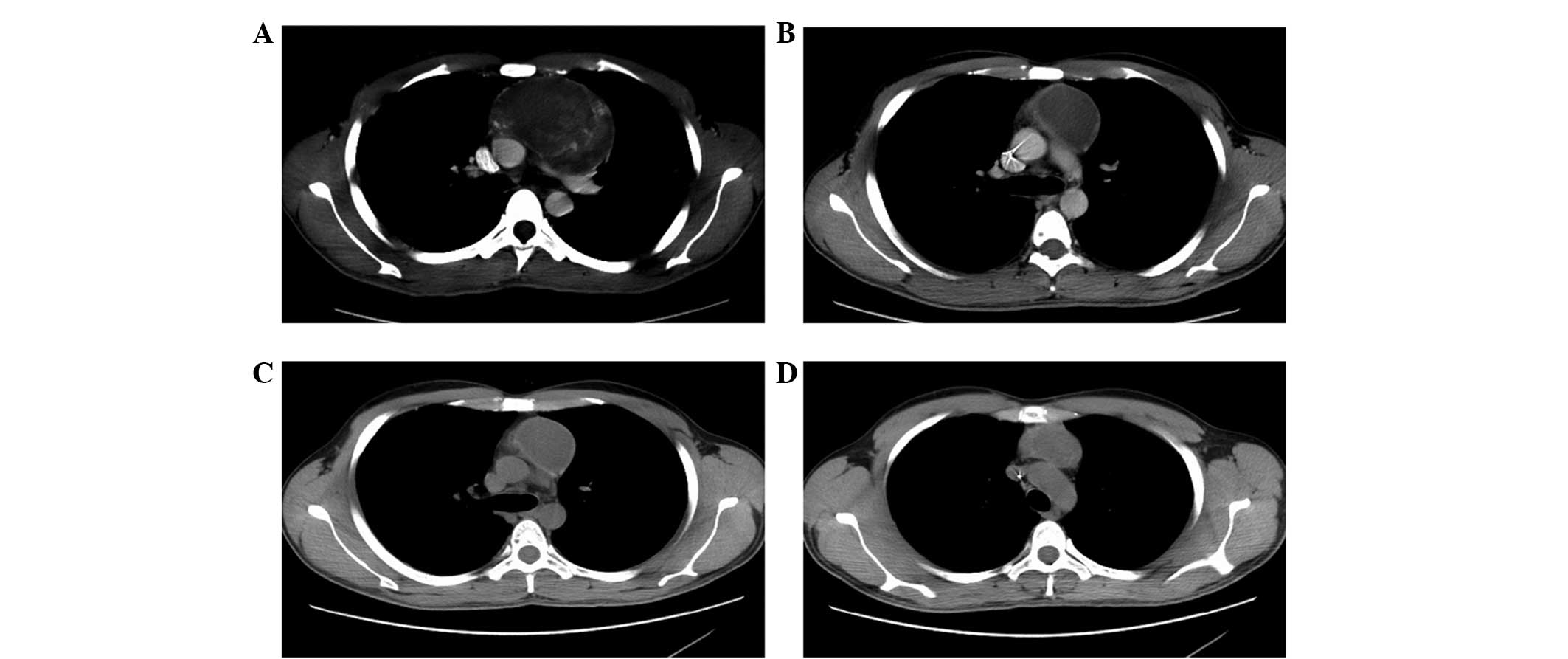
(Fig. 1A–D), and the size of the
mediastinal tumor was evidently reduced, with a less solid
component and a more cystic component (Fig. 2A–B). The response assessment
consistently indicated partial remission, according to Response
Evaluation Criteria in Solid Tumors v1.1 (16), every 2 cycles. When chemotherapy was
completed, the patient continued to experience left chest pain
without dyspnea. To obtain a better response, a radiation dose of
50 Gy was administered to the involved field of the mediastinum by
image-guided radiation therapy. The patient was treated with 2.0 Gy
a day and 5 fractions each week. Following radiotherapy, the β-HCG
level had also decreased to a normal level of 3.49 IU/l. CT
evaluation showed that the size of the residual lung lesions had
not evidently changed, and the mediastinal tumor was slightly
reduced in size (Fig. 2C), with a
much less solid component (Fig. 2D).
The patient refused to undergo surgery and did not receive
additional treatment following radiotherapy. At present, the
patient has survived >16 months of follow-up without any
symptoms, with the last evaluation performed on December 18,
2014.
Discussion
The prognosis of mediastinal choriocarcinoma appears
poor. Numerous patients succumb in a period of several weeks to a
few months (2,3,8,9,17). An
investigation based on 97 patients with male choriocarcinoma
revealed that the median overall survival (OS) time was 7.7 months
and the 6-month mortality rate was 45.4% (7). There was a consistent phenomenon among
patients with poor prognoses that β-HCG rapidly decreased to a
lower level during the treatment and then sharply rose when disease
relapsed (17). However, certain
studies have reported good results in male choriocarcinoma. A
clinical analysis of 13 men with primary choriocarcinoma indicated
that the median OS time was 54 months (range, 6–115 months), and
the 1- and 3-year survival rates were 53.8 and 43.1%, respectively,
although the prognosis was worse compared with the prognosis of
gestational choriocarcinoma (6).
Kathuria et al (18) reported
the case of a patient with mediastinal choriocarcinoma that
remained alive and asymptomatic 2 years subsequent to surgery and
chemotherapy. A regular occurrence in long-term survivors that
suffered from mediastinal choriocarcinoma was identified as
markedly elevated β-HCG levels that decreased to the normal range,
without signs of rising again, accompanied by complete clinical
remission (6). In the present study,
the patient experienced a biochemical remission and had a
relatively long survival time, though a small solid component
remained in the residual cystic mediastinal mass and two small
lesions remained in the lung. To the best of our knowledge, the
present study is the first to indicate that biochemical remission
may not be associated with clinical remission in male mediastinal
choriocarcinoma. The reason for this phenomenon is remains to be
elucidated. A possible reason is that the mediastinal mass may be
involved in the concurrent development of other germ cell tumors
that are resistant to chemotherapy and radiotherapy. However, this
may not explain the normalization of all tumor markers.
Primary mediastinal choriocarcinoma is an aggressive
and fatal cancer, and therefore rapid and appropriate treatment is
essential (2). However, there is no
standard management for this disease. Bokemeyer et al
(19) suggested that the management
principle for mediastinal choriocarcinoma was the same as that of
metastatic testicular germ cell tumors. Surgery is generally not
the primary treatment for mediastinal choriocarcinoma, due to
distant metastasis at initial diagnosis or surgical difficulties,
and is only performed if an emergent event associated with the
tumor exists, such as hemothorax (20). Chemotherapy is generally administered
as the primary initial treatment for male choriocarcinoma (9). Numerous studies had tried various
chemotherapy regimens, such as
methotrexate/actinomycin/chlorambucil and
5-fluorouracil/leucovorin/oxaliplatin, but these were shown to be
unsuccessful in this disease (21,22). The
most frequent systemic treatment is the BEP regimen. This
combination chemotherapy produces a poor response in numerous
patients; however, it shows potential for improving survival in
certain patients (3,23–26). Few
studies have reported the use of radiotherapy in mediastinal
choriocarcinoma. Gaude et al (3) suggested that deep radiation therapy was
not effective, as choriocarcinoma is a radioresistant tumor. The
patient in the present study refused a second biopsy and surgery,
so radiotherapy was then used to control the residual tumor in
order to improve the therapeutic effect. This demonstrated that
radiation has a mild effect on mediastinal choriocarcinoma. The
present results support the good response of the combination of
chemotherapy and radiotherapy in this malignancy.
In conclusion, there is no standard treatment for
mediastinal choriocarcinoma. BEP remains the optimal chemotherapy
regimen for this fatal disease, and multidisciplinary treatment may
improve its prognosis. However, it is necessary to explore new
treatment for patients with refractory mediastinal
choriocarcinoma.
Acknowledgements
The authors thank all nurses, pathologists and
laboratory technicians involved in the present study.
References
|
1
|
Collins DH and Pugh RC: Classification and
frequency of testicular tumours. Br J Urol. 36:1–11.
1964.PubMed/NCBI
|
|
2
|
Moran CA and Suster S: Primary mediastinal
choriocarcinomas: A clinicopathologic and immunohistochemical study
of eight cases. Am J Surg Pathol. 21:1007–1012. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gaude GS, Patil P, Malur PR, Kangale R,
Dhorigol V, Anurshetru S and Karanji J: Primary mediastinal
choriocarcinoma. South Asian J Cancer. 2:792013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lynch MJG and Blewitt GL: Choriocarcinoma
arising in the male mediastinum. Thorax. 8:157–161. 1953.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ramia JM, Alcalde J, Dhimes P and Cubedo
R: Metastasis from choriocarcinoma of the mediastinum producing
acute appendicitis. Dig Dis Sci. 3:332–334. 1998. View Article : Google Scholar
|
|
6
|
Jiang F, Xiang Y, Feng FZ, Ren T, Cui ZM
and Wan XR: Clinical analysis of 13 males with primary
choriocarcinoma and review of the literature. OncoTargets Ther.
7:1135–1141. 2014. View Article : Google Scholar
|
|
7
|
Yokoi K, Tanaka N, Furukawa K, Ishikawa N,
Seya T, Horiba K, Kanazawa Y, Yamada T, Ohaki Y and Tajiri T: Male
choriocarcinoma with metastasis to the jejunum: A case report and
review of the literature. J Nippon Med Sch. 75:116–121. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Krema H, Navajas E, Simpson ER and Payne
D: Choroidal metastasis from a mediastinal choriocarcinoma in a
male. Can J Ophthalmol. 46:551–552. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shen HH, Zhang GS and Xu F: Primary
choriocarcinoma in the anterior mediastinum in a man: A case report
and review of the literatures. Chin Med J (Engl). 117:1743–1745.
2004.PubMed/NCBI
|
|
10
|
Fine G, Smith RW Jr and Pachter MR:
Primary extragenital choriocarcinoma in the male subject. Case
report and review of the literature. Am J Med. 32:776–794. 1962.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Deshpande JR and Kinare SG:
Choriocarcinomatous transformation in metastases of an anaplastic
lung carcinoma-a case report. Indian J Cancer. 24:161–166.
1987.PubMed/NCBI
|
|
12
|
Szturmowicz M, Slodkowska J, Zych J,
Rudzinski P, Sakowicz A and Rowinska-Zakrzewska E: Frequency and
clinical significance of beta-subunit human chorionic gonadotropin
expression in non-small cell lung cancer patients. Tumour Biol.
20:99–104. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tscherry G, Jacky E, Jost LM and Stahel
RA: Risk-adapted chemotherapy of germ cell tumors with carboplatin,
etoposide and bleomycin for low-risk and cisplatin, etoposide and
ifosfamide for high-risk patients. A single-center study. Oncology.
59:110–117. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Oshima J, Uemura M, Kato T, Nagahara A,
Kiuchi H, Tsujimura A and Nonomura N: Modified BEP regimen leads to
abatement of choriocarcinoma syndrome in a patient with extra
gonadal germ cell tumor: A case report. Hinyokika Kiyo. 60:183–187.
2014.(In Japanese). PubMed/NCBI
|
|
15
|
US Department of Health and Human
Services. Common Terminology Criteria for Adverse Events (CTCAE).
Version 3. National Institute of Health. National Cancer Institute.
(Washington, DC). 2006.
|
|
16
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Belliveau RE, Wiernik PH and Sickles EA:
Blood carcinoembryonic antigen, Regan isoenzyme, and human
chorionic gonadotrophin in a man with primary mediastinal
choriocarcinoma. Lancet. 1:22–24. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kathuria S and Jablokow VR: Primary
choriocarcinoma of mediastinum with immunohistochemical study and
review of the literature. J Surg Oncol. 34:39–42. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bokemeyer C, Nichols CR, Droz JP, Schmoll
HJ, Horwich A, Gerl A, Fossa SD, Beyer J, Pont J, Kanz L, et al:
Extragonadal germ cell tumors of the mediastinum and
retroperitoneum: Results from an international analysis. J Clin
Oncol. 20:1864–1873. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ruan Z, Wang S, Wang Z and Jing Y: A rare
case of bilateral massive hemothorax from spontaneous rupture of a
primary mediastinal mixed germ cell tumor. Ann Thorac Surg.
93:664–666. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yoon JH, Kim MS, Kook EH, Ahn SH, Jeong
SY, Han MS, Huh JK, Kang HJ, Na II, Cho SY, et al: Primary gastric
choriocarcinoma: Two case reports and review of the literatures.
Cancer Res Treat. 40:145–150. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cohen BA and Needle MA: Primary
mediastinal choriocarcinoma in a man. Chest. 67:106–108. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shastri A, Daver NG and Hayes TG: Primary
gastric chorioadenocarcinoma: A needle in a haystack. Rare Tumors.
3:e192011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhang F, Zhang W, Shi H, Ye G, Shi W, Shu
Y and Li G: Primary choriocarcinoma of the posterior mediastinum in
a male: A case report and review of the literature. Oncol Lett.
8:739–741. 2014.PubMed/NCBI
|
|
25
|
Liu Z, Mira JL and Cruz-Caudillo JC:
Primary gastric choriocarcinoma: A case report and review of the
literature. Arch Pathol Lab Med. 125:1601–1604. 2001.PubMed/NCBI
|
|
26
|
Yamane T, Egawa H, Deguchi N and Moritani
C: A case of primary mediastinal choriocarcinoma. Nihon Kokyuki
Gakkai Zasshi. 44:48–54. 2006.(In Japanese). PubMed/NCBI
|