Introduction
Lymphoepithelioma-like gastric carcinoma (LELGC),
initially described by Watanabe et al (1) in 1976 as gastric carcinoma with a
lymphoid stroma, is a rare type of gastric carcinoma. It presents
with a unique histological pattern that is characterized by poorly
differentiated malignant cells along with massive lymphocyte
infiltration of the background stroma (2). LELGC constitutes 1.1–4.6% of all gastric
carcinoma cases (3), and is generally
considered to have a more favorable prognosis compared with other
types of gastric malignancy (4).
However, the reason for its better prognosis has not been fully
clarified and the underlying mechanism remains to be
elucidated.
Lymphoepithelioma-like carcinoma (LELC) has been
reported to occur at various anatomical sites, including the
salivary gland, thymus, larynx, lung, esophagus, uterine cervix,
urinary bladder and skin (5). As with
the majority of gastric carcinomas, LELGC typically occurs in
elderly people. Two histological patterns have been reported: The
first, Regaud type, exhibits well-defined epithelial nests
separated by broad areas of lymphocytic reaction, while the second
pattern is characterized by tumor cells growing in a diffuse manner
mimicking malignant lymphoma, and is known as the Schmincke type
(6).
LELGC may also be categorized into two subsets:
Epstein-Barr virus (EBV)-positive and microsatellite instability
(MSI)-high carcinoma (7). It has been
demonstrated that EBV is present in >80% of LELGC cases,
suggesting that LELGC is closely associated with EBV infection
(7). The prevalence of MSI-high
carcinoma in LELGC ranges from 7 to 39%, with apparent geographic
variability (7). LELGC also
demonstrates a male predominance and a predisposition to the
proximal stomach (8,9). More precisely, the predominant locations
of EBV-positive carcinomas are the cardia and middle portion of the
stomach, while MSI-high carcinomas are more common in the gastric
antrum (7).
The current study reports a case of LELGC occurring
in a male patient with a rectal laterally spreading tumor (LST); to
the best of our knowledge, this has not been reported previously.
This report highlights this rare variant of gastric carcinoma and
discusses the diagnosis and prognosis of LELGC.
Case report
A 50-year-old male patient with no specific past
medical history was admitted to Nanjing Drum Tower Hospital
affiliated to Nanjing University Medical School (Nanjing, Jiangsu)
in September 2014, complaining of epigastric discomfort and
occasional hematochezia. A colonoscopy performed at a local
hospital (Xuyi People's Hospital, Xuyi, China) revealed an LST in
the rectum, located 10 cm from the anus. A gastroscopy (Olympus
GIF-XQ260; Olympus Corp., Tokyo, Japan) also revealed a submucosal
columnar lesion with surface erosion at the anterior wall of the
gastric body. The physical examination and laboratory tests
initially performed at our hospital yielded no abnormal findings.
The results were as follows: Blood, white blood cells,
6.5×109 cells/l (normal range, 4.0–10.0×109
cells/l); neutrophils, 54.9% (normal range, 51.0–75.0%); urine,
negative; stool/occult blood test, negative; liver and kidney
functions, alanine aminotransferase, 18.9 units (U)/l (normal
range, 5.0–40.0 U/l); γ-glutamyl transferase, 17.5 U/l (normal
range, 7.0–35.0 U/l); total bilirubin, 20.4 µmol/l (normal range,
5.0–20.5 µmol/l); direct bilirubin, 4.7 µmol/l (normal range,
1.7–6.8 µmol/l); albumin, 40.0 g/l (normal range, 35.0–51.0 g/l);
blood urea nitrogen, 4.4 mmol/l (normal range, 2.9–7.5 mmol/l);
creatinine, 71 µmol/l (normal range, 44–106 µmol/l); triglyceride,
1.15 mmol/l (normal range, 0.56–1.70 mmol/l); total cholesterol,
5.10 mmol/l (normal range, 2.90–5.72 mmol/l); K+, 3.77
mmol/l (normal range, 3.50–5.50 mmol/l); C-reactive protein, 2.4
mg/l (normal range, 0.0–8.0 mg/l); blood clotting, fibrinogen, 2.1
g/l (normal range, 2.0–4.0 g/l); blood transfusion, human
immunodeficiency virus/hepatitis B/hepatitis C/syphilis, all
negative; tumor markers, α-fetoprotein, 2.30 ng/ml (normal range,
0.0–10.0 ng/ml); carcinoembryonic antigen, 0.43 ng/ml (normal
range, 0.0–10.0 ng/ml); CA72-4, 0.86 U/ml (normal range, 0.0–6.9
U/ml); CA125, 1.80 U/ml (normal range, 0.0–30.2 U/ml; CA19-9,
<0.6 U/ml (normal range, 0.0–39.0 U/ml); CA242, 3.51 U/ml
(normal range, 0.0–15.0 U/ml); electrocardiogram, sinus rhythm;
heart rate, 68 beats/min; chest X-ray, normal.
A contrast-enhanced computed tomography (CT;
Discovery CT750 HD; GE Healthcare Bio-Sciences, Pittsburgh, PA,
USA) scan of the abdomen was conducted, indicating a focal
thickening of the mucosa at the lesser curvature wall of the
gastric body. No evidence of perigastric infiltration, enlarged
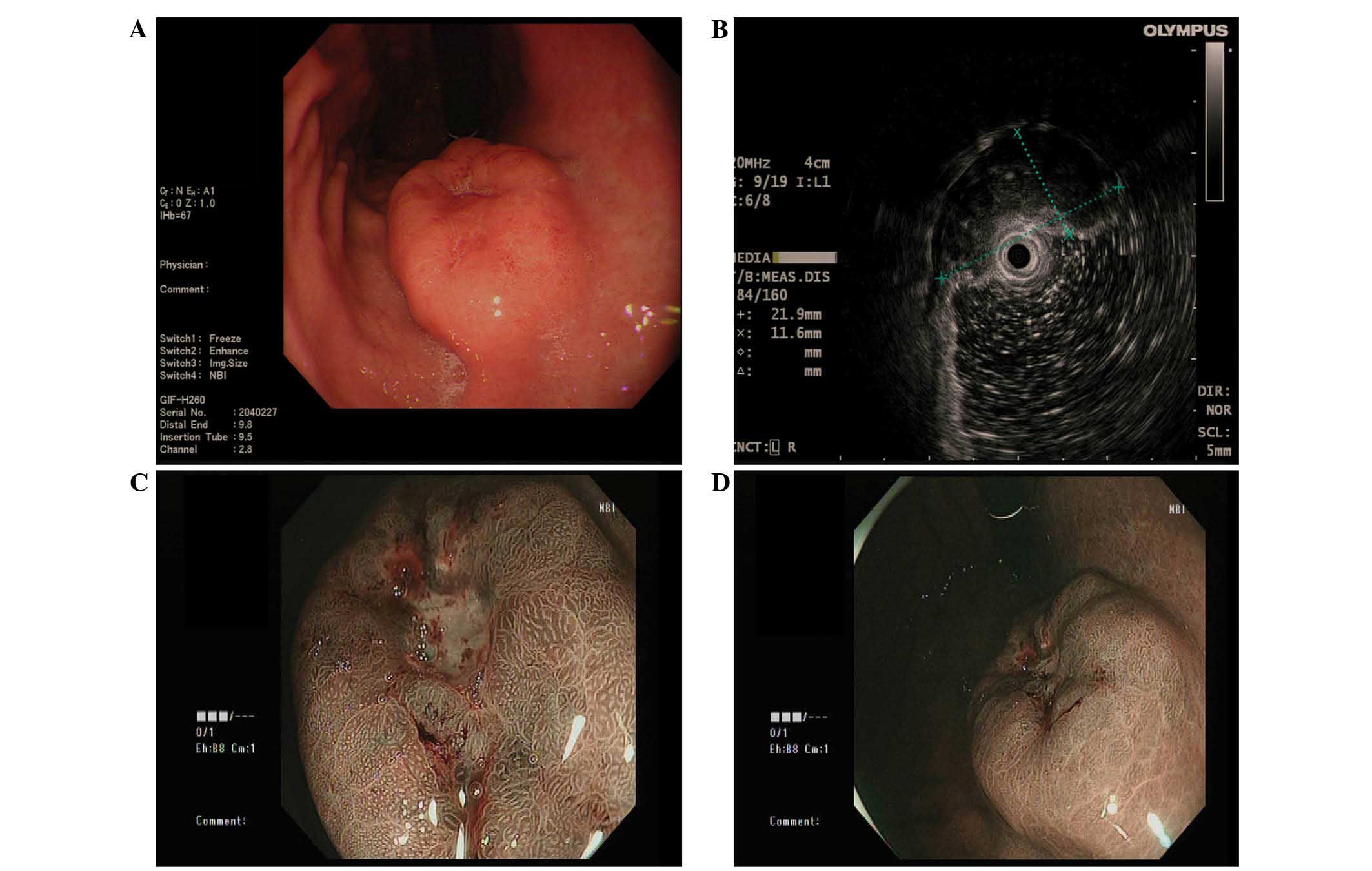
lymph nodes or distant metastasis was observed by CT. Endoscopic
ultrasound examination (Olympus EU-ME-1; Olympus Corp.)
demonstrated a heterogeneous hypoechoic mass at the lesion site,
originating from the submucosal layer and with intracavity
protrusion; its transverse section measured 21.9×11.6 mm (Fig. 1). The narrow band image observation of
the lesion suggested no evident glandular ducts in the central area
and normal glandular ducts in the peripheral area. A biopsy
indicated moderate chronic superficial gastritis with proliferation
of plasma cells. Simultaneously, numerous lymphoepithelial lesions
were observed. The tissues were sent to a pathologist at the
Nanjing Drum Tower Hospital affiliated to Nanjing University
Medical School for immunohistochemical analysis.
Immunohistochemical staining confirmed the proliferative plasma
cells to be of λ type. A pathological diagnosis of lymphoma could
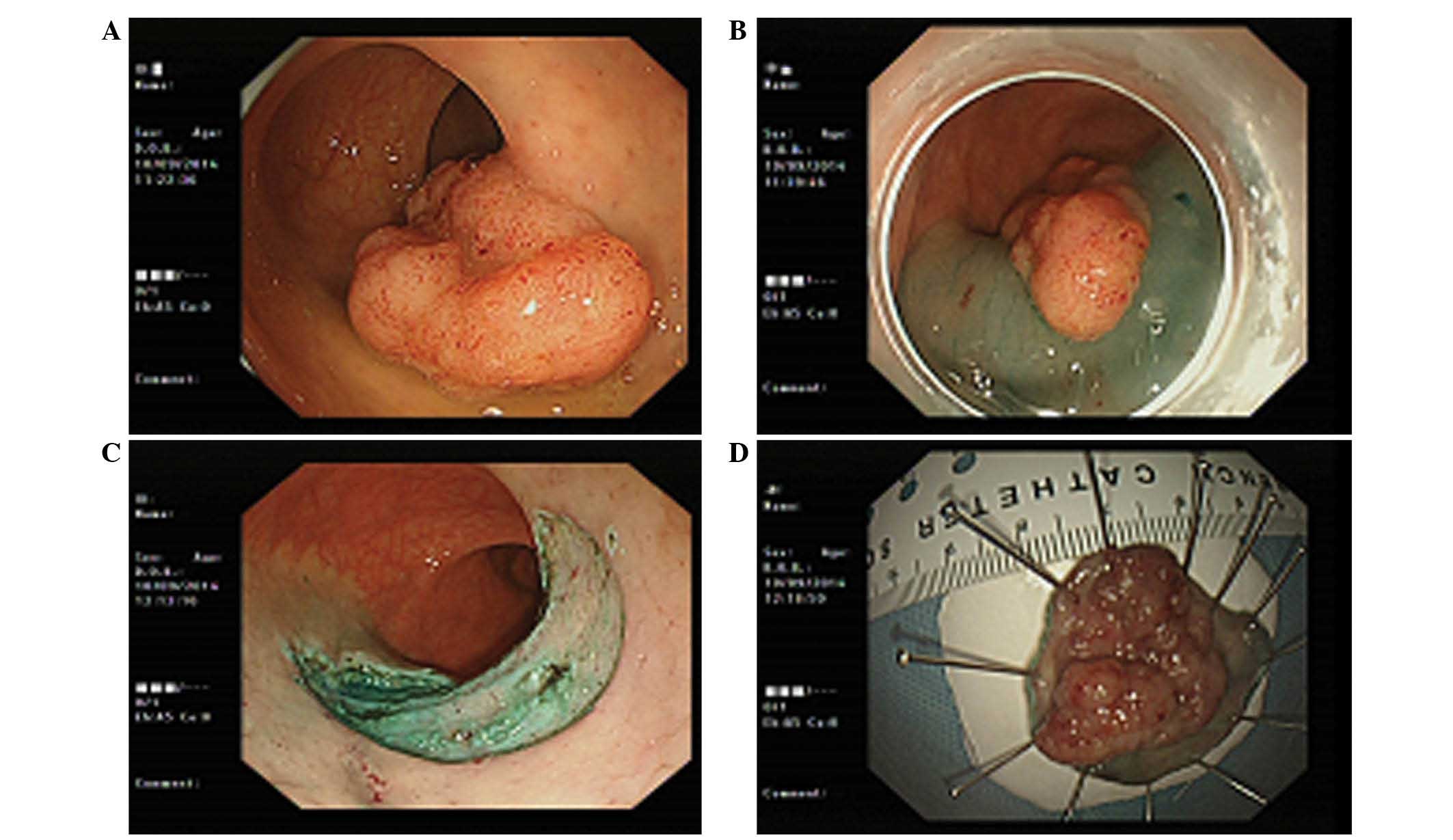
not be established due to a lack of evidence. Endoscopic submucosal
dissection (ESD) was first performed for the rectal LST (Fig. 2), and its postoperative pathology
revealed villous adenoma with low-grade intraepithelial neoplasia.
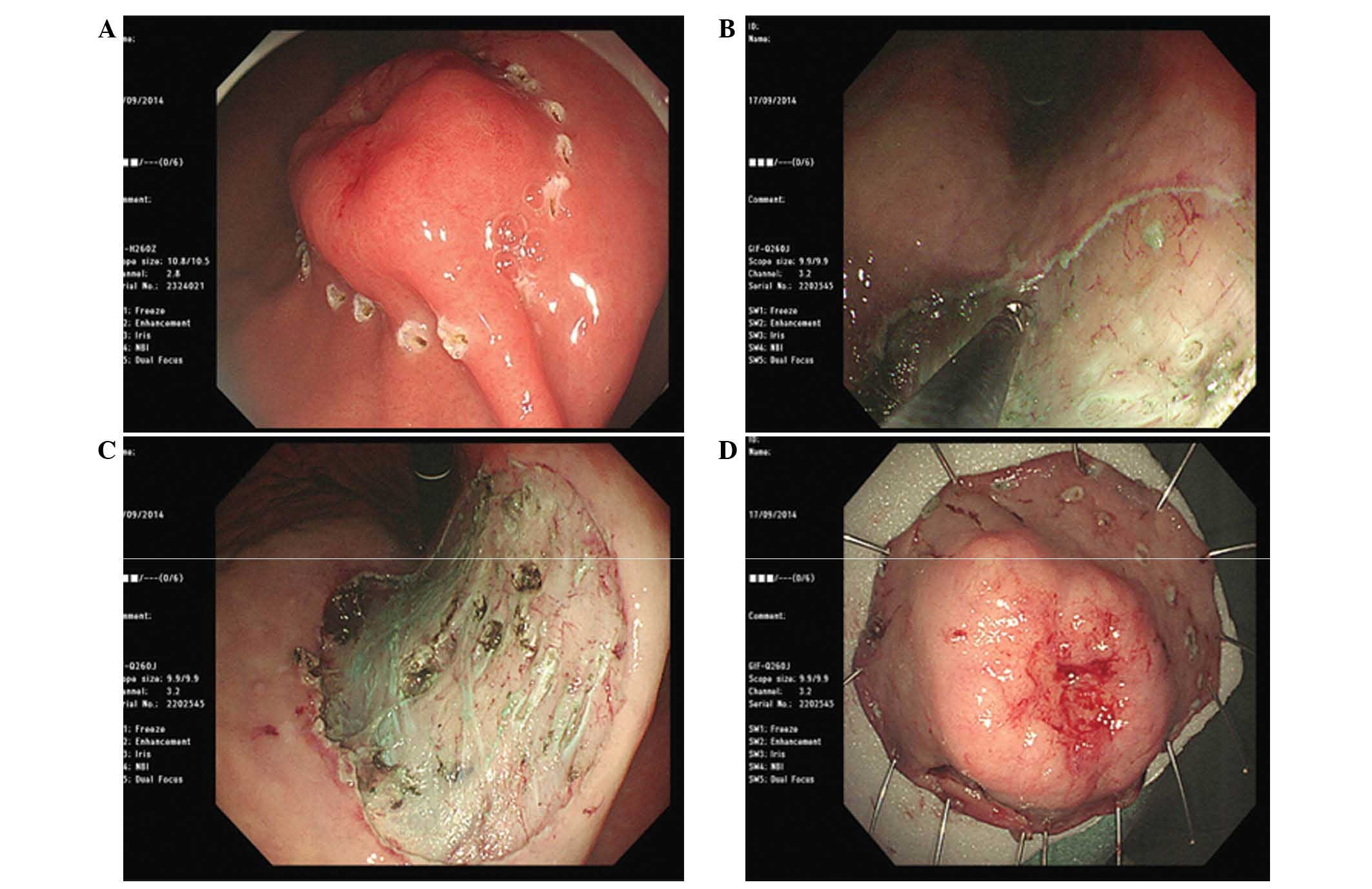
Subsequently. ESD of the gastric lesion was successfully performed
(Fig. 3). The lesion measured
2.5×2.5×0.4 cm. The specimen was obtained following the provision
of consent from the patient.
The specimens were sent to a pathologist at the
Nanjing Drum Tower Hospital affiliated to Nanjing University
Medical School for histological and immunohistochemical analysis.
Briefly, the gastric ESD specimen was fixed in formalin (Hubei
Taikang Medical Equipment Co. Ltd., Xiaogan, China) and embedded in
paraffin (Hubei Taikang Medical Equipment Co. Ltd.). The tissue
sections were cut into 4-µm slices. For histological examination,
the sections were deparaffinized by xylene (2 times, 10 min each;
Hubei Taikang Medical Equipment Co. Ltd.), then rehydrated in
ethanol (2 changes for 5 min each, including 95% alcohol for 2 min
and 70% ethanol for 2 min; Hubei Taikang Medical Equipment Co.
Ltd.). The sections were briefly washed in distilled water prior to
being stained with Harris hematoxylin and eosin (Hubei Taikang
Medical Equipment Co. Ltd.) and mounted with xylene-based mounting
medium (Hubei Taikang Medical Equipment Co. Ltd.). For
immunohistochemical examination, the sections were baked at 60°C
for 6 h, and then dewaxed in xylene and rehydrated through a
sequence of decreasing concentration of alcoholic solutions (Hubei
Taikang Medical Equipment Co. Ltd.). Endogenous peroxidase activity
was quenched by 3% H2O2 (Nanjing Chemical
Reagent Co., Ltd., Nanjing, China) incubation for 10 min at room
temperature. For antigen retrieval, tissue slides were boiled in 1
mmol/l ethylenediaminetetraacetic acid (pH 8.0; Nanjing Chemical
Reagent Co., Ltd.) in an autoclave (catalog no., ALP-CL-32L; ALP
Co., Ltd., Tokyo, Japan) for 10 min. Subsequent to washing three
times for 5 min with PBS, the sections were incubated with mouse
anti-human anti-cytokeratin monoclonal antibody (dilution, 1:100;
catalog no., C2562; Sigma-Aldrich, St. Louis, MO, USA), at 4°C
overnight. Secondary antibody, an anti-mouse IgG antibody from the
PV-9000 kit (ZSGB-BIO, Beijing, China) was diluted to 1:1000 using
Tris-buffered saline with Tween 20 (100 ml) containing skim milk (5
g; Brightdairy Co. Ltd, Shanghai, China). The slices were then
incubated with the secondary for 30 min at room temperature
susequent to washing three times with PBS (Nanjing Chemical Reagent
Co., Ltd.). The immunoreactivity was revealed using
diaminobenzidine (Wuhan Boster Biological Technology, Ltd., Wuhan,
China) as the final chromogen. Finally, the sections were
counterstained with hematoxylin and then dehydrated and mounted.
Negative controls were carried out by omission of the primary
antibody. Known immunostaining positive slides were used as
positive controls. All slides were observed using an Olympus BX53
microscope (Olympus Corporation, Tokyo, Japan).
Histopathological and immunohistochemical
examinations of the gastric lesion ESD specimen were compatible
with LELGC (Fig. 4) (7). The cytokeratin (pan) staining revealed
the existence of tumor cells that were derived from epithelial
tissue, and in situ hybridization (ISH) was used to confirm
the presence of EBV. EBV-encoded small RNA (EBER) is abundant in
each latently infected cell (up to 107 molecules/cell).
Using EBER ISH (StatSpin ThermoBrite; Abbott Laboratories, Abbott
Park, IL, USA), all or the vast majority of neoplastic cells show
positive signals in positive cases. EBER-ISH has been used as a
gold standard to identify EBV-associated gastric carcinomas.
Furthermore, the basal margin was positive for carcinoma, whereas
the lateral margin was negative. The tumor had invaded the
submucosal layer. Therefore, on the 7th day after ESD, the patient
received an additional total radical gastrectomy. Dissection of
group 1–9 lymph nodes was completed. No local metastases, enlarged
lymph nodes or carcinoma-like tissues were observed in the stomach.
The postoperative pathological stage was IA T1bN0cM0 according to
the Tumor-Node-Metastasis classification of gastric carcinoma
(10). At a follow-up 3 months
subsequent to the ESD, the patient was found to have recovered well
from surgery, with no recurrence. The patient has received no
further treatment, and at the most recent follow-up appointment in
September 2015 no positive findings were observed following
gastroscopy and CT.
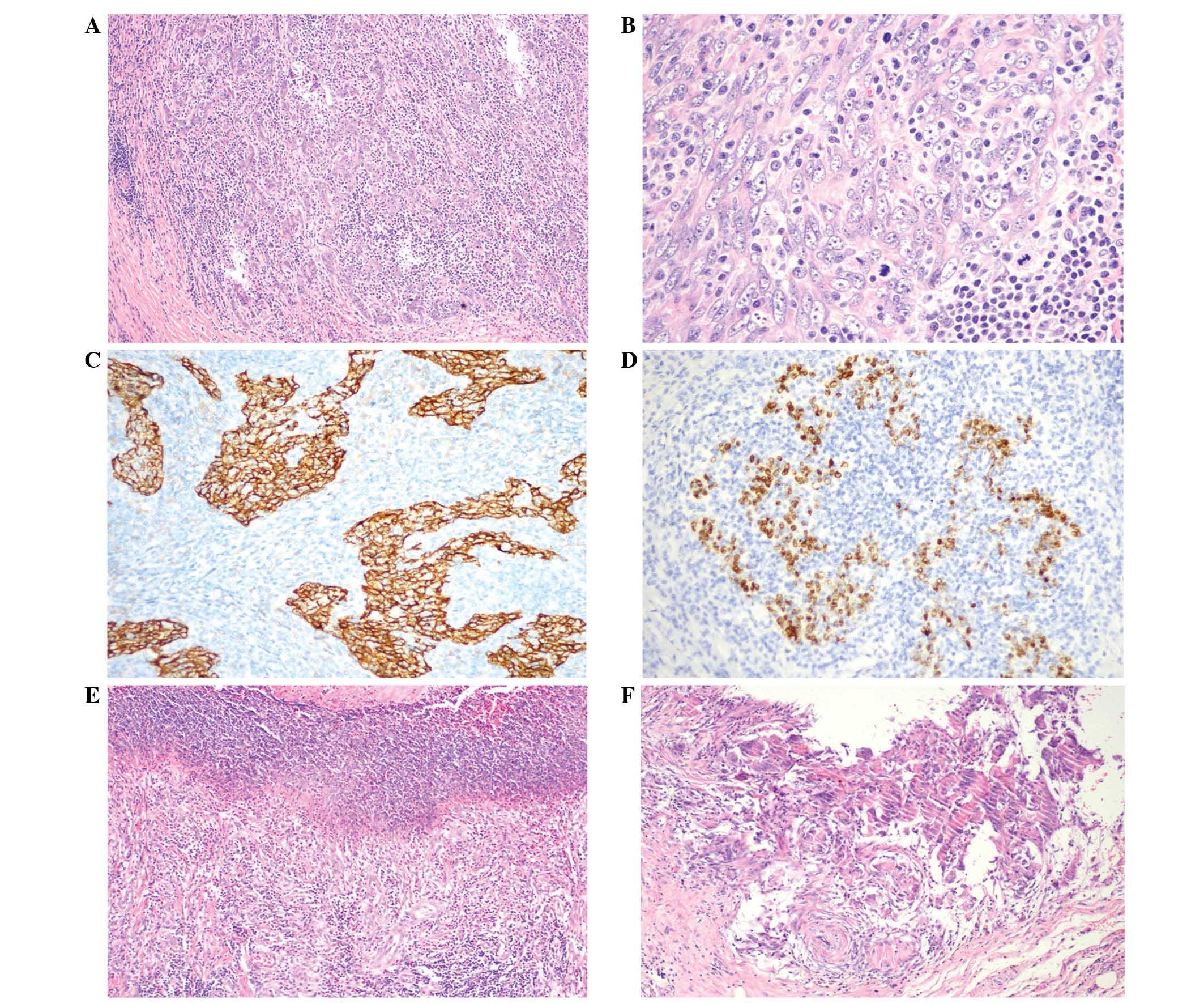 | Figure 4.Pathology of ESD specimen of the
gastric lesion. The histopathological and immunohistochemical
examinations were compatible with LELGC. The basal margin was
positive for carcinoma whereas the lateral margin was negative. The
tumor had invaded the submucosal layer. (A and B) The tumor
infiltrated uniformly with an abundance of lymphocytes and plasma
cells throughout the entire area of the tumor. [Hematoxylin and
eosin staining; (A) magnification, x100, (B) magnification, x400].
(C) Cytokeratin expression was positive in the LELGC (Envision
double staining; magnification, x200) and (D) Epstein-Barr
virus-encoded RNA in situ hybridization also was positive
(magnification, x200). Postoperatively, lymphoepithelioma-like
carcinoma of the stomach was diagnosed and staged as IA T1bN0cM0
according to the Tumor-Node-Metastasis classification of gastric
carcinoma. (E) Ulceration was observed in the ESD specimen
(hematoxylin and eosin staining; magnification, x100); (F) no
carcinoma tissue was found in the ulcer (hematoxylin and eosin
staining; magnification, x200). ESD, endoscopic submucosal
dissection; LELGC, lymphoepithelioma-like gastric carcinoma. |
Discussion
LELGC is a type of gastric carcinoma with
characteristic clinicopathologic features (6,11); it is
also called gastric carcinoma with lymphoid stroma (9). Following the publication of the report
by Moore and Foote (12) indicating
that medullary carcinoma of the breast with lymphoid infiltration
is associated with EBV infection, similar findings were reported
regarding carcinomas of the stomach (1). According to the World Health
Organization classification of tumors of the digestive system,
LELGC is a type of tubular carcinoma (13). It has been reported that lymphocytic
infiltration in LELGC may be a host defensive reaction against the
cancer, and that a greater extent of lymphocytic infiltration may
be associated with better prognosis (4).
Patients with LELGCs frequently exhibit no
significant symptoms, and when clinical symptoms are exhibited they
are often similar to conventional gastric adenocarcinoma (8). Furthermore, LELGCs are often
macroscopically mistaken for submucosal tumors (SMTs) (6). Therefore, accurate diagnosis may be
difficult prior to surgery, even if an endoscopic biopsy is
performed. Lesions composed of lymphocytic infiltration may be
mistaken for an intense reactive lymphoid infiltrate or even
lymphoma (5). In fact, in the present
case, a definitive diagnosis of LELGC could not be established
using the sample obtained by endoscopic biopsy; despite performing
the endoscopic biopsy twice, a definitive diagnosis could not be
determined as the tumor mimicked SMT. Subsequently, ESD for local
resection was conducted, and a diagnosis of LELC was established on
the basis of the histological characteristics of the dissected
specimen. Takahashi et al (14) previously demonstrated a strategy for
the diagnosis and treatment of gastric SMTs by laparoscopic surgery
based on tumor measuring, and reported that this procedure may be
useful as it aids accurate diagnosis and may be followed by
curative surgery. Therefore, we speculate that laparoscopic surgery
could be replaced by ESD, as was conducted in the present case. Lee
et al (6) reported that ESD
treatment of EBV-associated early LELC may have favorable long-term
outcomes, despite deep submucosal invasion of tumor cells.
Therefore, a conservative management strategy without additional
surgery may be considered for EBV-positive early LELC with
submucosal invasion treated by ESD, particularly in patients with
severe comorbidity or high surgical risk (6). To enable conservative management,
intensive medical follow-up must be performed using
esophagogastroduodenoscopy (EGD) and abdominal CT scans (4).
As mentioned, LELGC has been reported to have a
favorable prognosis compared with ordinary gastric carcinoma
(4). Specifically, EBV-positive as
well as MSI-high tumors in general have themselves been variably
associated with a survival advantage (4). Whether the advantage is related to the
lymphoid infiltrate, or whether the EBV or MSI statuses themselves
serve as independent prognosticators remains to be explained
(7). However, large-scale research by
Beghelli et al (15) concluded
that the MSI phenotype (stage II only) is significantly associated
with survival.
In summary, the current study describes a case of
LELGC in a patient with rectal LST. LELGC is a rare morphological
variant of gastric carcinoma that has special clinical and
histological features that distinguish it from ordinary gastric
adenocarcinomas. The endoscopic findings revealed a submucosal
columnar lesion with surface erosion at the anterior wall of the
gastric body. The diagnosis of LELGC should primarily rely on the
characteristic morphology and detection of EBV by EBV-encoded RNA,
polymerase chain reaction (PCR), or Southern blot technique, or
detection of MSI-high status by immunohistochemistry for DNA repair
proteins and/or microsatellite PCR of specific markers. It is
recommended that screening using EGD is necessary for patients with
symptoms relating to the digestive system, including hematochezia.
Understanding the clinical and histopathological features of LELGC
is important in the preoperative diagnosis and in differentiating
this entity from other tumors, which has decisive effect on the
selection of treatment and the final outcome. The present study
describes a classical case of LELGC with positive EBV and
cytokeratin expression according to in situ hybridization
and immunohistochemical analysis.
Acknowledgements
The authors would like to thank Dr Xiangshan Fan and
Dr Qi Sun (Department of Pathology, Nanjing Drum Tower Hospital,
Nanjing, University Medical, School, Nanjing, China) for their
pathological guidance and diagnosis.
References
|
1
|
Watanabe H, Enjoji M and Imai T: Gastric
carcinoma with lymphoid stroma. Its morphologic characteristic and
prognostic correlations. Cancer. 38:232–243. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gromski MA, Miller CA, Lee SH, Lee TH,
Chung IK, Park SH, Kim SJ and Cho HD: Gastric
lymphoepithelioma-like carcinoma mimicking a subepithelial lesion
treated by endoscopic submucosal dissection. Gastrointest Endosc.
76:419–421. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shibata D, Tokunaga M, Uemura Y, Sato E,
Tanaka S and Weiss LM: Association of Epstein-Barr virus with
undifferentiated gastric carcinomas with intense lymphoid
infiltration. Lymphoepithelioma-like carcinoma. Am J Pathol.
139:469–474. 1991.PubMed/NCBI
|
|
4
|
van Beek J, zur Hausen A, Klein Kranenbarg
E, van de Velde CJ, Middledorp JM, van den Brule AJ, Meijer CJ and
Bloemena E: EBV-positive gastric adenocarcinomas: A distinct
clinicopathologic entity with a low frequency of lymph node
involvement. J Clin Oncol. 22:664–670. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shibata D and Weiss LM: Epstein-Barr
virus-associated gastric adenocarcinoma. Am J Pathol. 140:769–794.
1992.PubMed/NCBI
|
|
6
|
Lee JY, Kim KM, Min BH, Lee JH, Rhee PL
and Kim JJ: Epstein-Barr virus-associated lymphoepithelioma-like
early gastric carcinomas and endoscopic submucosal dissection: Case
series. World J Gastroenterol. 20:1365–1370. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Grogg KL, Lohse CM, Pankratz VS, Halling
KC and Smyrk TC: Lymphocyte-rich gastric cancer: Associations with
Epstein-Barr virus, microsatellite instability, histology and
survival. Mod Pathol. 16:641–651. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Song HJ, Srivastava A, Lee J, Kim YS, Kim
KM, Kang Ki W, Kim M and Kim S, Park CK and Kim S: Host
inflammatory resoponse predicts survival of patients with
Epstein-Barr virus-associated gastric carcinoma. Gastroenterology.
139:84–92. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Herath CH and Chetty R: Epstein-Barr
virus-associated lymphoepithelioma-like gastric carcinoma. Arch
Pathol Lab Med. 132:706–709. 2008.PubMed/NCBI
|
|
10
|
Ajani J, D'Amico TA, Hayman JA, Meropol NJ
and Minsky B: National Comprehensive Cancer Network: Gastric
cancer. Clinical practice guidelines in oncology. J Natl Compr Canc
Netw. 1:28–39. 2003.PubMed/NCBI
|
|
11
|
Cheng N, Hui DY, Liu Y, Zhang NN, Jiang Y,
Han J, Li HG, Ding YG, Du H, Chen JN and Shao CK: Is gastric
lymphoepithelioma-like carcinoma as a special subtype of
EBV-associated gastric carcinoma? New insight based on
clinicopathological features and EBV genoma polymorphisms. Gastric
Cancer. 18:246–255. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Moore OS Jr and Foote FW Jr: The
relatively favorable prognosis of medullary carcinoma of the
breast. Cancer. 2:635–642. 1949. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fenoglio-Preiser C, Carneiro F, Correa P,
Guilford P, Lambert R and Megraud F: Gastric carcinoma. World
Health Organization Classification of Tumours - Pathology and
Genetics of Tumours of the Digestive System. Hamilton SR and
Aaltonen LA: IARC Press. (Lyon, France). 37–52. 2000.
|
|
14
|
Takahashi T, Otani Y, Yoshida M, Furukawa
T, Kameyama K, Akiba Y, Saikawa Y, Kubota T, Kumai K, Kuramochi S,
et al: Gastric cancer mimicking a submucosal tumor diagnosed by
laparoscopic excision biopsy. J Laparoendosc Adv Surg Tech A.
15:51–56. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Beghelli S, de Manzoni G, Barbi S,
Tomezzoli A, Roviello F, Di Gregorio C, Vindigni C, Bortesi L,
Parisi A, Saragoni L, et al: Microsatellite instability in gastric
cancer is associated with better prognosis in only stage II
cancers. Surgery. 139:347–356. 2006. View Article : Google Scholar : PubMed/NCBI
|