Introduction
Previously, patients presenting with benign adenoma
and colorectal neoplasms at the T1 stage were advised to undergo an
endoscopic mucosal resection (EMR) (1). EMR is generally considered to be an
endoscopic alternative to the surgical resection of mucosal and
submucosal neoplastic lesions and intramucosal cancers (2). Various complications of EMR, including
hemorrhages and perforations, have been reported. Alternatively,
manifestations such as pneumothorax, pneumomediastinum,
pneumoperitoneum, pneumoretroperitoneum and subcutaneous emphysema
following EMR are extremely rare. At present, only 3 cases of
colonic perforation and 1 case of rectal perforation have been
described in the literature, and the clinical diagnoses and
treatments were varied, with no additional results of follow-up
studies being reported (3–6). The present study reports that for rectal
perforation, which is revealed by an acute clinical manifestation,
early imaging recognition by a computerized axial tomography (CT)
scan and appropriate management is associated with optimal results.
The results of a follow-up study that occurred 4 months
subsequently suggested that the recovery of the patient was
comprehensive. Written informed consent was obtained from the
patient.
Case report
In May 2014, a 51-year-old male underwent a
colonoscopy at the First Affiliated Hospital of Kunming Medical
University (Kunming, China). In June 2014, the patient returned to
the same hospital for an EMR of rectal adenoma. The patient
possessed a previous medical history of a brain abscess close to
the left basal ganglia region that was treated with ceftriaxone
sodium for 14 days. The colonoscopy was performed in the left
lateral position while the patient was sedated using 1.5 mg/kg
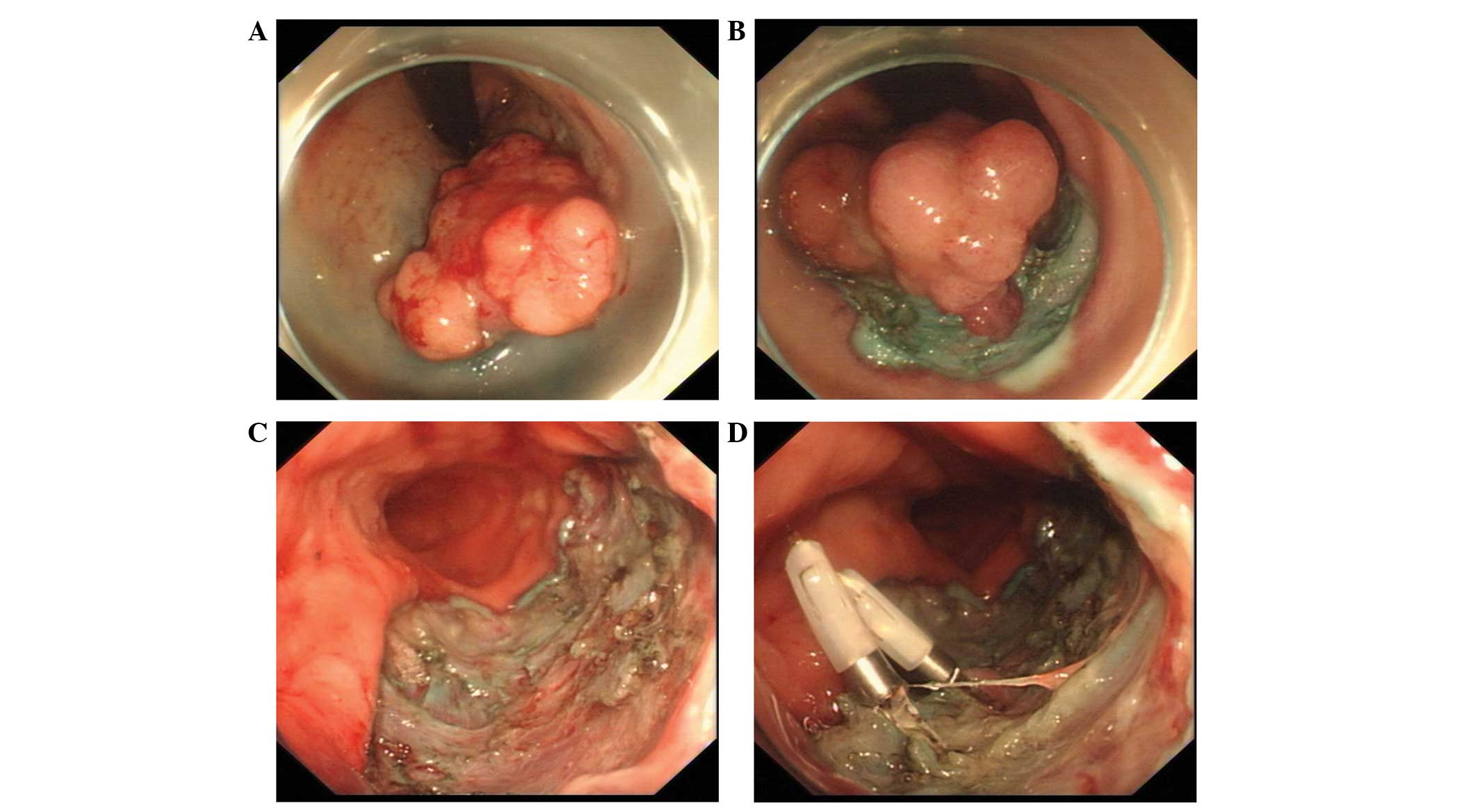
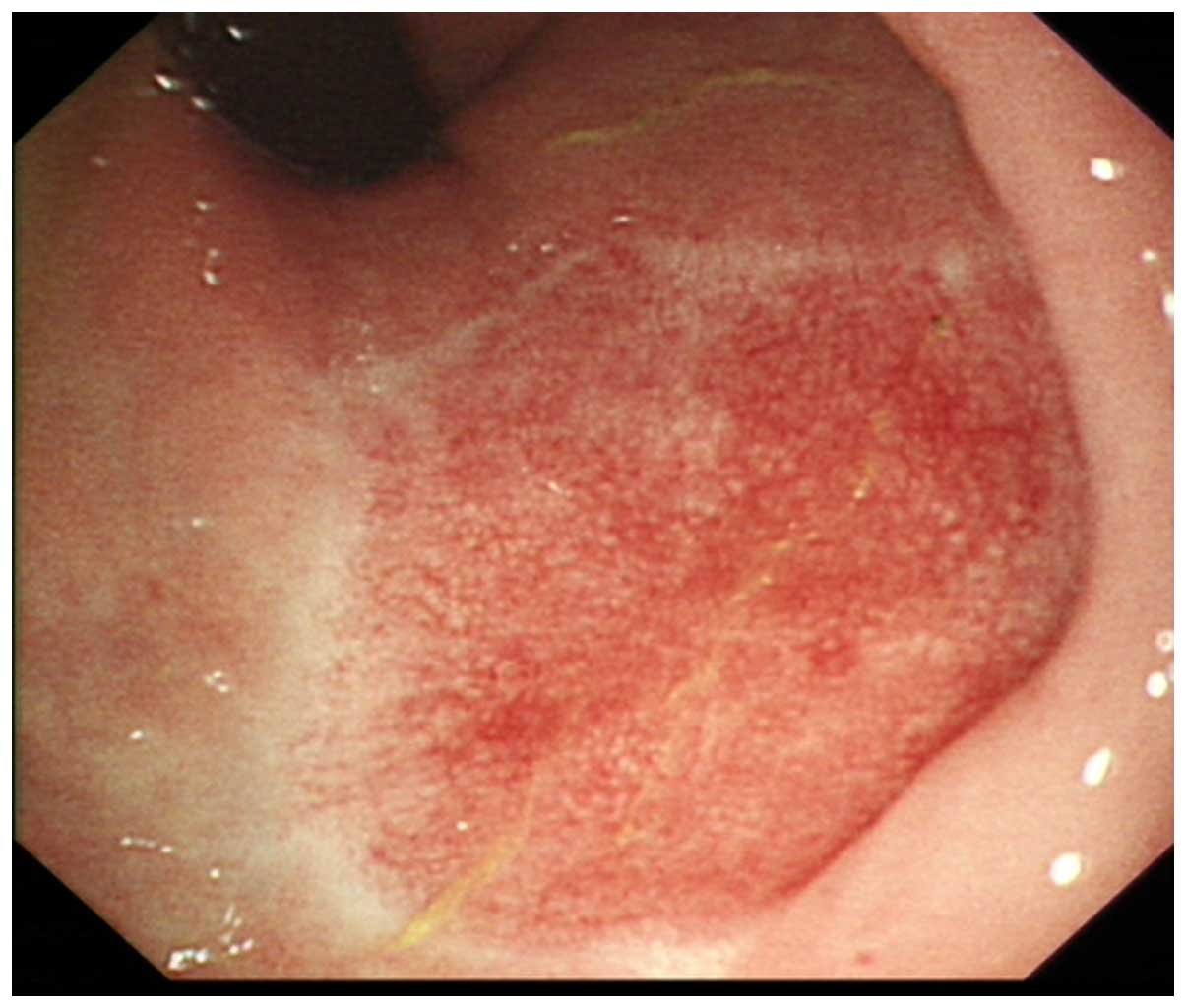
intravenous propofol. The colonoscopy revealed a lobulated rectal
adenoma, 1.5 cm in diameter, at the 4–6 o'clock position, located 5
cm from the anal verge, and the superficial margin was clear
(Fig. 1A). An endoscopic mucosal
resection using a transparent cap (EMR-C) (2,6) was
performed with the intent to cure (Fig.
1B) (6,7). Following the EMR, no residual tumors at
the periphery or any definite perforations were revealed using
magnified observation (Fig. 1C).
Subsequently, 2 titanium clips were used for wound hemostasis
(Fig. 1D). No complications, such as
massive bleeding or perforations, were identified during
colonoscopy.
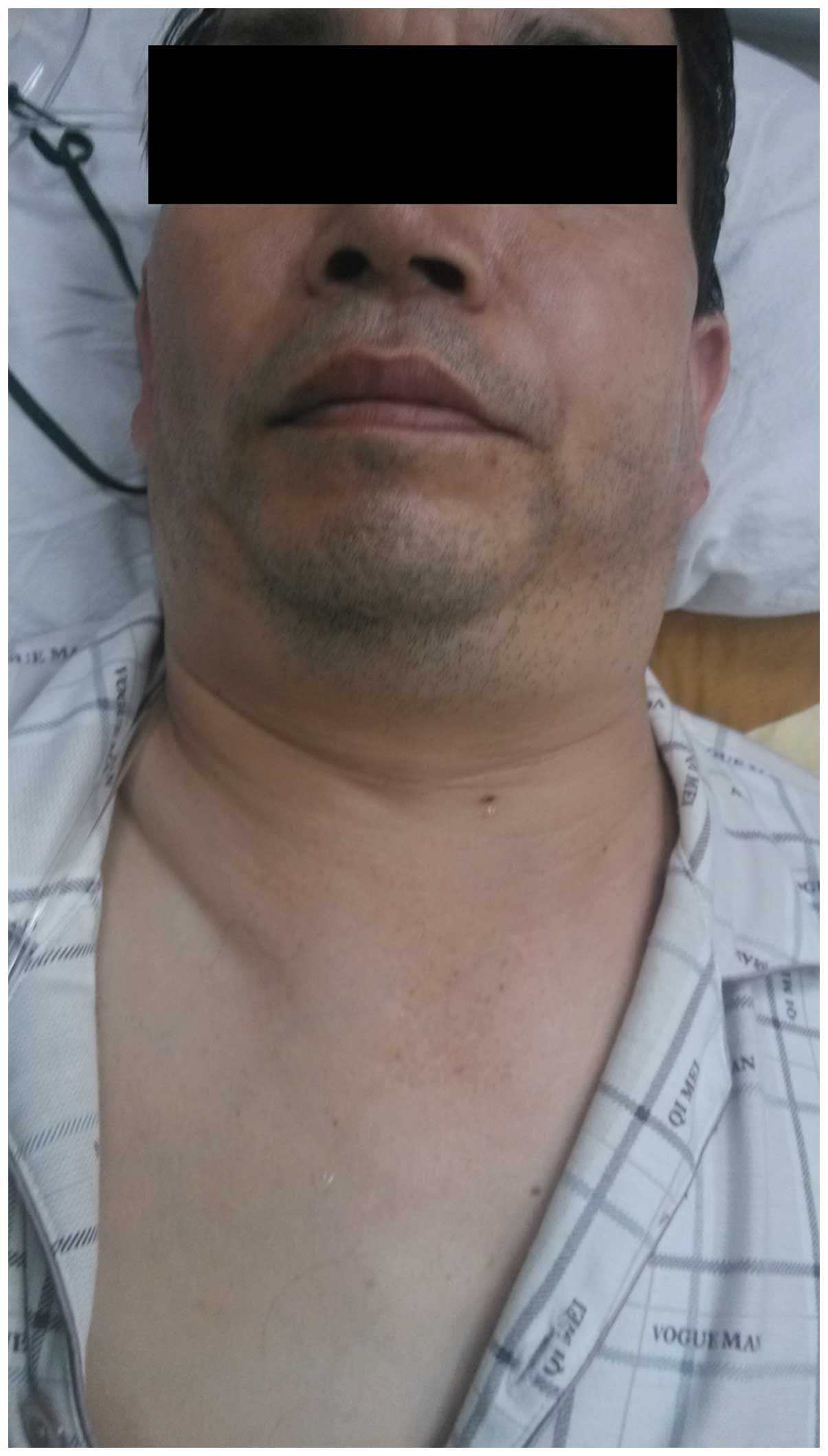
Following the EMR, the patient suddenly suffered
from breathing difficulties. At this point, the patient developed
acute subcutaneous emphysema of the neck (Fig. 2), posterior chest wall, and anterior
and lateral abdominal walls. Following the intake of oxygen
(FiO2, 41%) for 5 min, the dyspnea symptoms demonstrated
no sign of improvement. An emergency chest X-ray examination was
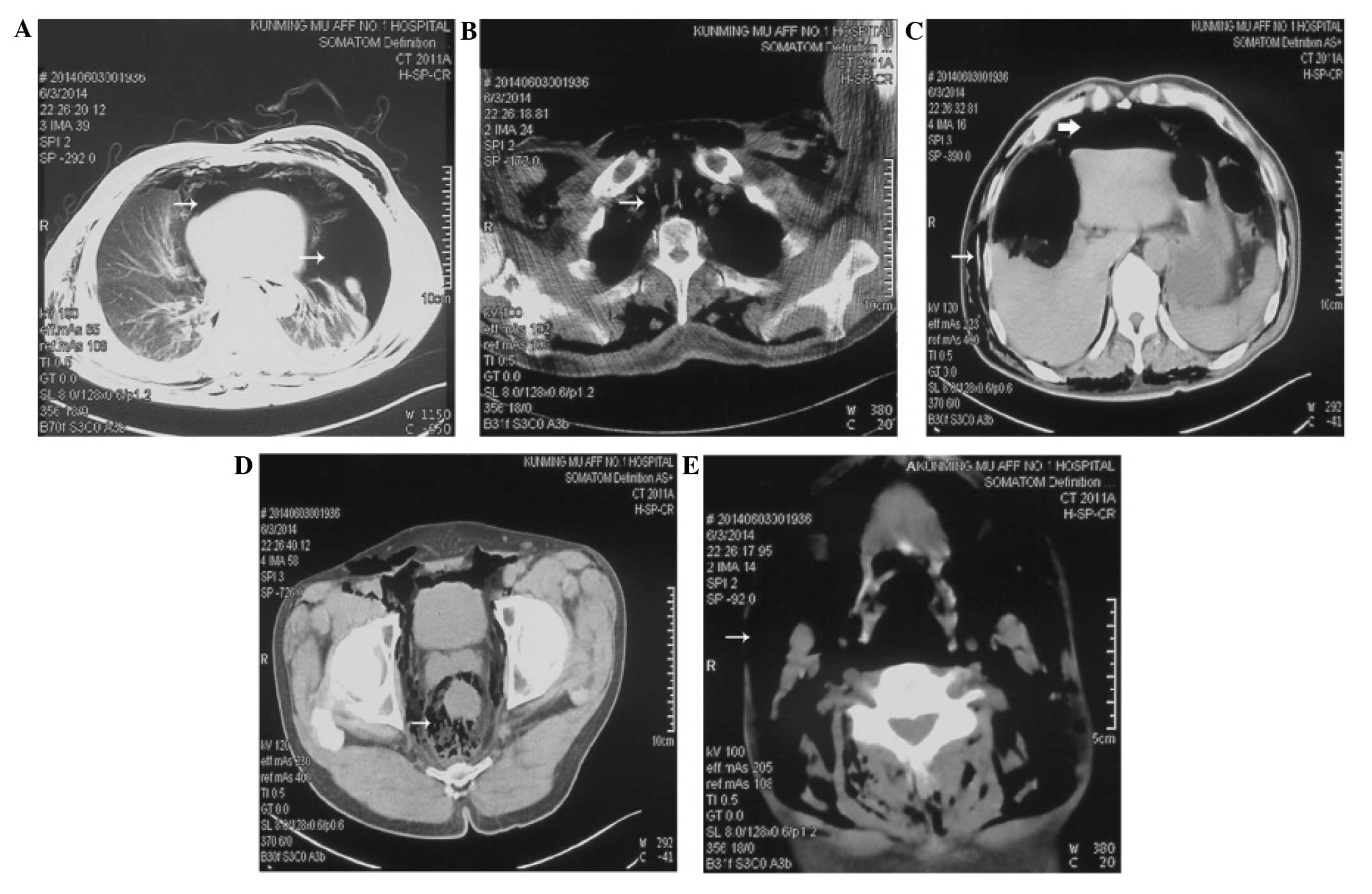
performed and a bilateral pneumothorax was indicated (Fig. 3). Additionally, a CT scan of the
chest, abdomen and pelvis was performed. The CT scan results also
demonstrated a bilateral pneumothorax, occupying ~70 and 20% of the
left and right thoracic cavities, respectively (Fig. 4A), pneumomediastinum (Fig. 4B), pneumoperitoneum (Fig. 4C), and pneumoretroperitoneum extending
down to the presacral space (Fig.
4D). Extensive cervical subcutaneous emphysema was also
identified (Fig. 4E).
The laboratory data revealed that the white blood
cell count was 11.5×1012cells/l (normal range,
4.0–10.0×1012 cells/l), and that the C-reactive protein
level was 65 mg/l (normal range, 0–3.3 mg/l). Due to the dyspnea
symptoms, intercostal drainage of the left pneumothorax was
performed immediately. A follow-up chest X-ray exhibited a
resolving pneumomediastinum and the resolution of the pneumothorax
1 day later. As no peritonitis developed, the patient was managed
conservatively with intravenous fluids and intravenous antibiotics
(ceftriaxone sodium; 2 g/day) for 72 h prior to the gradual
re-introduction of oral fluid and food. The pneumoperitoneum,
pneumoretroperitoneum and subcutaneous emphysema were almost
resolved within 7 days, and the CT reexamination and physical
examination revealed a rapid, but not comprehensive, recovery. The
white blood cell count and C-reactive protein levels decreased to
normal. The excised specimen was histologically diagnosed as
tubular adenoma, with focal carcinoma that was limited to within
the mucosal layer. No residual tumor was found at the basal region
of the tumor specimen. Following discharge, the patient reported no
complaints of dyspnea or hematochezia in the monthly telephone
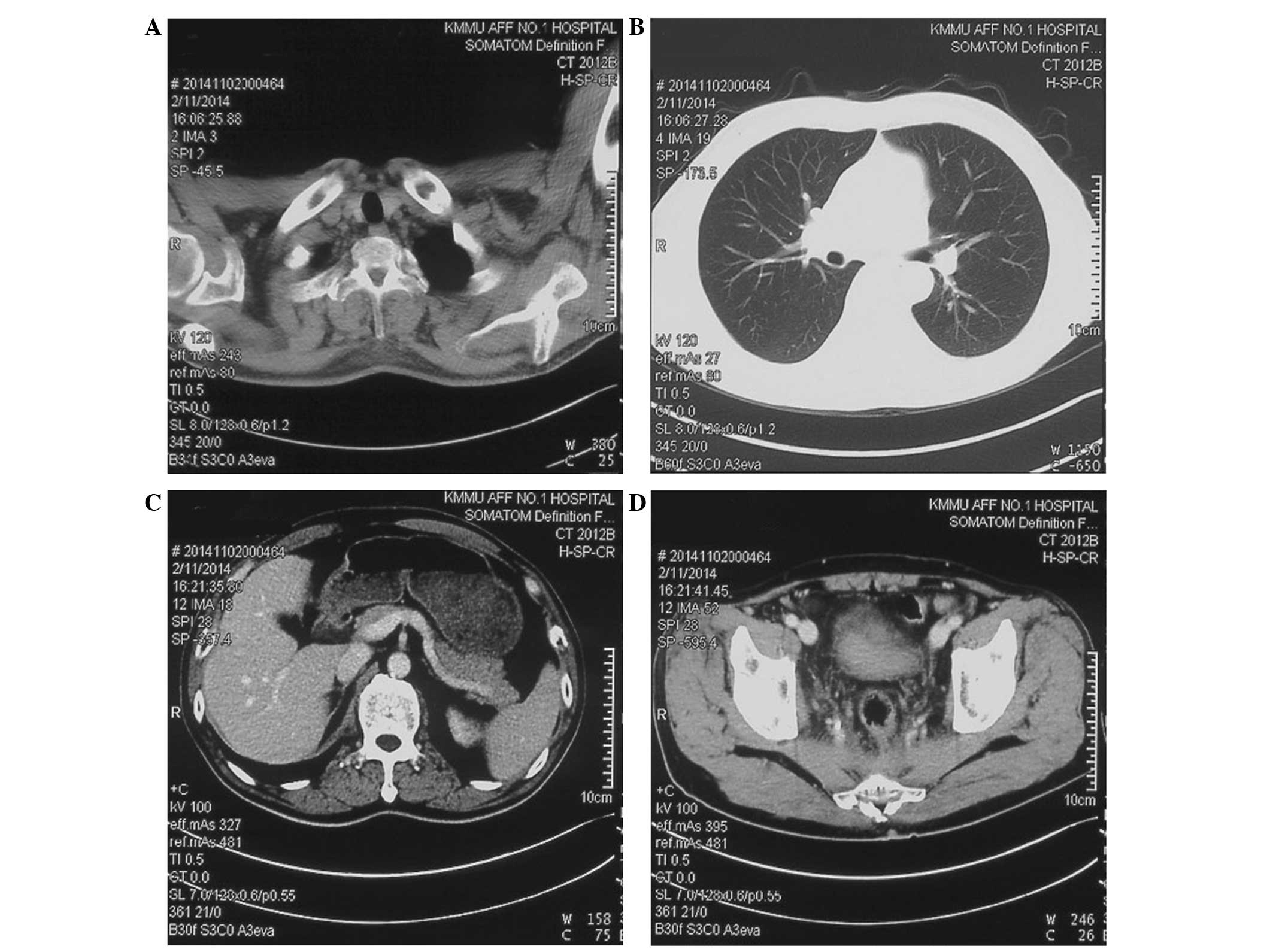
follow-ups. Subsequent to 4 months of follow up, a colonoscopy
demonstrated that the rectal mucosal wound and scar was healing
(Fig. 5), and a CT scan provided no
evidence of subcutaneous emphysema or interstitial pneumatosis
(Fig. 6).
Discussion
The incidence of colorectal perforation following
colonoscopy has been reported to range between 0.16% in diagnostic
colonoscopies and 0.44% in therapeutic colonoscopies (8). The major causes of perforation include
excessive air insufflation, instrumental trauma and the improper
use of electrocautery, while the factors that increase the risk of
perforation include old age, medical comorbidity and therapeutic
procedures, such as polypectomy, pneumatic dilation and endoscopic
mucosal resection (9–11). The majority of the signs of colonic
perforation are abdominal symptoms, such as acute peritonitis.
However, the current patient presented with bilateral pneumothorax
and subcutaneous emphysema as early signs of a rectal perforation
following EMR, which caused serious dyspnea symptoms and neck
swelling. In the present patient, pneumothorax was first indicated
by an emergency chest X-ray; however, additional CT imaging tests
comprehensively revealed the rare manifestations of pneumothorax,
pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum and
extensive subcutaneous emphysema. Thus, CT is effective and
recommended for early recognition in cases presenting with
colorectal perforation.
There are varying mechanisms through which
extraluminal air may reach the various body compartments, including
undue instrument manipulation, air insufflation or improper use of
diathermy (5,9,10). In the
present study, extraluminal air entered the body due to rectal
perforation following EMR. The retroperitoneal air resulted from a
direct retroperitoneal space in rectal perforation, then the
extraluminal air accumulated and passed along the mesentery to the
retroperitoneum. Subsequently, air travelled along the fascial
planes to enter the mediastinum, which caused the
pneumomediastinum. A subsequent rupture of the mediastinal pleura
allowed air to decompress into the pleural cavity and caused the
pneumothorax (5,12).
The choice of conservative or surgical treatment for
iatrogenic colonic perforation remains controversial (13–15).
Finding air in the pleural and abdominal cavity may be an early
sign of a life-threatening condition. In the present case, due to
the serious dyspnea, intercostal drainage was performed immediately
to improve the breathing difficulties. For patients that present
with colonic perforation and acute peritonitis, a fecal diversion
with a colostomy was suggested (10).
In the present study, the choice of conservative treatment for the
pneumoperitoneum was based on the following factors: First, the
abdominal pain was mild and localized, and no complaint of acute
peritonitis was observed; and second, the movement of air from the
peritoneal space is usually considered as non-infectious and may be
treated conservatively (3). In the
present patient, the pneumoperitoneum, pneumoretroperitoneum and
subcutaneous emphysema were almost resolved within 7 days of
treatment. A CT reexamination and physical examination revealed a
rapid and uneventful recovery, and a follow-up 4 months
subsequently revealed a comprehensive recovery without subcutaneous
emphysema or interstitial pneumatosis.
In conclusion, the present study reports a case of
rectal perforation following EMR. Dyspnea and neck swelling are
acute signs of extraluminal air resulting from rectal perforation.
CT examination is a fast and effective method for the early and
comprehensive assessment of the condition of a patient. Appropriate
management and close follow-up are crucial for optimal results.
References
|
1
|
Hurlstone DP, Sanders DS, Cross SS, Adam
I, Shorthouse AJ, Brown S, Drew K and Lobo AJ: Colonoscopic
resection of lateral spreading tumours: A prospective analysis of
endoscopic mucosal resection. Gut. 53:1334–1339. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Park SJ: Tips and tricks for better
endoscopic treatment of colorectal tumors: Usefulness of cap and
band in colorectal endoscopic mucosal resection. Clin Endosc.
46:492–494. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fu KI, Sano Y, Kato S, Fujii T, Sugito M,
Ono M, Saito N, Kawashima K, Yoshida S and Fujimori T:
Pneumoscrotum: A rare manifestation of perforation associated with
therapeutic colonoscopy. World J Gastroenterol. 11:5061–5063. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Marwan K, Farmer KC, Varley C and Chapple
KS: Pneumothorax, pneumomediastinum, pneumoperitoneum,
pneumoretroperitoneum and subcutaneous emphysema following
diagnostic colonoscopy. Ann R Coll Surg Engl. 89:W20–W21. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zeno BR and Sahn SA:
Colonoscopy-associated pneumothorax: A case of tension pneumothorax
and review of the literature. Am J Med Sci. 332:153–155. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Denadai R, Medeiros CC, Toledo AP,
Carvalho AF Jr and Muraro CA: Rectal perforation after colonoscopic
polypectomy presented as subcutaneous emphysema, pneumomediastinum
and pneumoretroperitoneum successfully treated conservatively in an
elderly adult. J Am Geriatr Soc. 61:1433–1435. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Endo S, Hirasaki S, Doi T, Endo H, Nishina
T, Moriwaki T, Nakauchi M, Masumoto T, Tanimizu M and Hyodo I:
Granular cell tumor occurring in the sigmoid colon treated by
endoscopic mucosal resection using a transparent cap (EMR-C). J
Gastroenterol. 38:385–389. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kim HH, Park SJ, Lee SH, Park HU, Song CS,
Park MI and Moon W: Efficacy of endoscopic submucosal resection
with a ligation device for removing small rectal carcinoid tumor
compared with endoscopic mucosal resection: Analysis of 100 cases.
Dig Endosc. 24:159–163. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bakker J, van Kersen F and Spruyt Bellaar
J: Pneumopericardium and pneumomediastinum after polypectomy.
Endoscopy. 23:46–47. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lohsiriwat V: Colonoscopic perforation:
Incidence, risk factors, management and outcome. World J
Gastroenterol. 16:425–430. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Castellví J, Pi F, Sueiras A, Vallet J,
Bollo J, Tomas A, Verge J, Caballero F, Iglesias C and De Castro J:
Colonoscopic perforation: Useful parameters for early diagnosis and
conservative treatment. Int J Colorectal Dis. 26:1183–1190. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ho HC, Burchell S, Morris P and Yu M:
Colon perforation, bilateral pneumothoraces, pneumopericardium,
pneumomediastinum, and subcutaneous emphysema complicating
endoscopic polypectomy: Anatomic and management considerations. Am
Surg. 62:770–774. 1996.PubMed/NCBI
|
|
13
|
La Torre M, Velluti F, Giuliani G, Di
Giulio E, Ziparo V and La Torre F: Promptness of diagnosis is the
main prognostic factor after colonoscopic perforation. Colorectal
Dis. 14:e23–e26. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Donatelli G, Vergeau BM, Dumont JL,
Altmann C, Dritsas S, Dhumane P, Tuszynski T and Meduri B: Delayed
successful treatment of iatrogenic colon perforation using an
over-the-scope clip. Endoscopy. 46(Suppl 1): E285–E286.
2014.PubMed/NCBI
|
|
15
|
Xiao YF, Bai JY, Yu J, Lin XL, Zhao XY,
Yang SM and Fan CQ: Endoscopic treatment of delayed colon
perforation: The enteroscopy overtube approach. Endoscopy.
46:503–508. 2014. View Article : Google Scholar : PubMed/NCBI
|