Introduction
Total hysterectomy and bilateral
salpingo-oophorectomy with selective surgical staging is considered
the standard treatment in patients with endometrial cancer (EC);
however, in cases judged to be unsuitable for surgery due to severe
medical comorbidities, exclusive radiotherapy (RT; i.e., external
beam radiation plus brachytherapy) represents a valid option, since
it is well-tolerated and provides an acceptable rate of pelvic
control and long-term progression-free survival (1–3). The
documentation of multiple comorbidities in elderly patients
represents an even more complex condition, so that exclusive RT can
be hardly affordable given the poor performance status of patients,
their presumed higher risk of sequelae and in certain cases, the
existence of logistic obstacles. In this context, the efficacy of
palliative radiation schedules in terms of local symptom control
has been confirmed in several studies (4–8): in
particular, among palliative RT fractionation schedules utilized in
pelvic malignancies, the most common implies the use of doses
within 20–40 Gy in 5–20 fractions, as reported by clinical
experiences in other tumor sites (4).
Alternatively, shorter schedules have also been attempted, which
proved to achieve satisfying rates of overall symptom relief
(41–60%) (6,9). Besides palliative RT, hormonal treatment
has also been acknowledged as a potential alternative in selected
patients with endometrial endometrioid carcinoma (10–12).
Despite the limits inherent in a small sample series, progestin
administration has been reported to provide an encouraging rate of
response of 59% in early EC patients considered unfit for surgery
(13–15). Although intrauterine progestin
administration has been less frequently adopted compared with oral
progestin, its advantages in terms of the risk reduction of certain
conditions, including thrombophlebitis, weight gain and headache,
should not be underestimated in the setting of frail, elderly EC
patients, who often suffer from hypertension and obesity (16). Moreover, recent observations have
suggested that intrauterine progestin administration could be more
effective than oral administration in the treatment of complex
atypical hyperplasia in terms of the complete response rate, the
recurrence rate and the requirement to perform hysterectomies
(17,18). In this context, the combined use of
palliative RT and intrauterine progestin administration may
represent a valuable option to be tested in selected settings.
The present study thus investigated the combination
of the levonorgestrel-releasing intrauterine device (LNG-IUD) and
palliative RT as a potential approach to treating frail, elderly EC
patients considered unfit for curative oncological treatments.
Patients and methods
Study subjects
The clinicopathological features and outcome data
was collected for uterine tumor patients considered unfit for
radical treatment, and the combination of LNG-IUD and palliative
radiation was subsequently offered at the Radiotherapy Unit of the
Department of Oncology, ‘Giovanni Paolo II’ Foundation, Catholic
University of the Sacred Heart (Campobasso, Italy).
The assessment of the complete resolution of
bleeding, the duration of bleeding control, the actuarial rate of
relapse of symptoms, and the rate and pattern of toxicity were
recorded.
All procedures were approved by the head of the
Oncology Department of the ‘Giovanni Paolo II’ Foundation, Catholic
University of the Sacred Heart, Campobasso, Italy, on behalf of the
Internal Board Committee, and were in accordance with the Helsinki
Declaration, 2008 revision.
Inclusion criteria were an age of ≥65 years,
pathological confirmation (endometrial biopsy) of a uterine
neoplasm, a Charlson comorbidity index (CCI) value of ≥4 and the
presence of vaginal bleeding. Patients were excluded in cases that
lacked histological proof of a uterine tumor. Data regarding age,
Eastern Cooperative Oncology Group (ECOG) status, anemia (defined
as hemoglobin <11.5 g/dl), body mass index and comorbidities
were recorded.
Pretreatment assessment
All patients underwent a physical and gynecological
examination and complete laboratory tests, including full blood
count, blood electrolytes, creatinine, liver transaminases, serum
levels of cancer antigen (CA)-125. A histological diagnosis was
made by biopsies at hysteroscopy, and all samples were reviewed by
a dedicated gynecological pathologist. Extension of disease was
evaluated in all patients by abdominopelvic computed tomography
(CT) or magnetic resonance imaging.
Treatment
At the time of starting the pretreatment RT workup,
all patients were accurately counseled and were required to provide
written informed consent for all procedures. Patients were than
convened at the Gynecological Oncology Unit for intrauterine
insertion of an LNG-IUD system (Mirena®; Bayer Health
Care Pharmaceutical Inc., Wayne, NY, USA), which consists of a
T-shaped polyethylene device (19)
that releases 20 µg LNG daily for up to 5 years (20).
Thereafter, all patients underwent CT simulation
(CT-Sim) in the supine position, and CT-Sim images were captured at
5-mm increments over the region of interest.
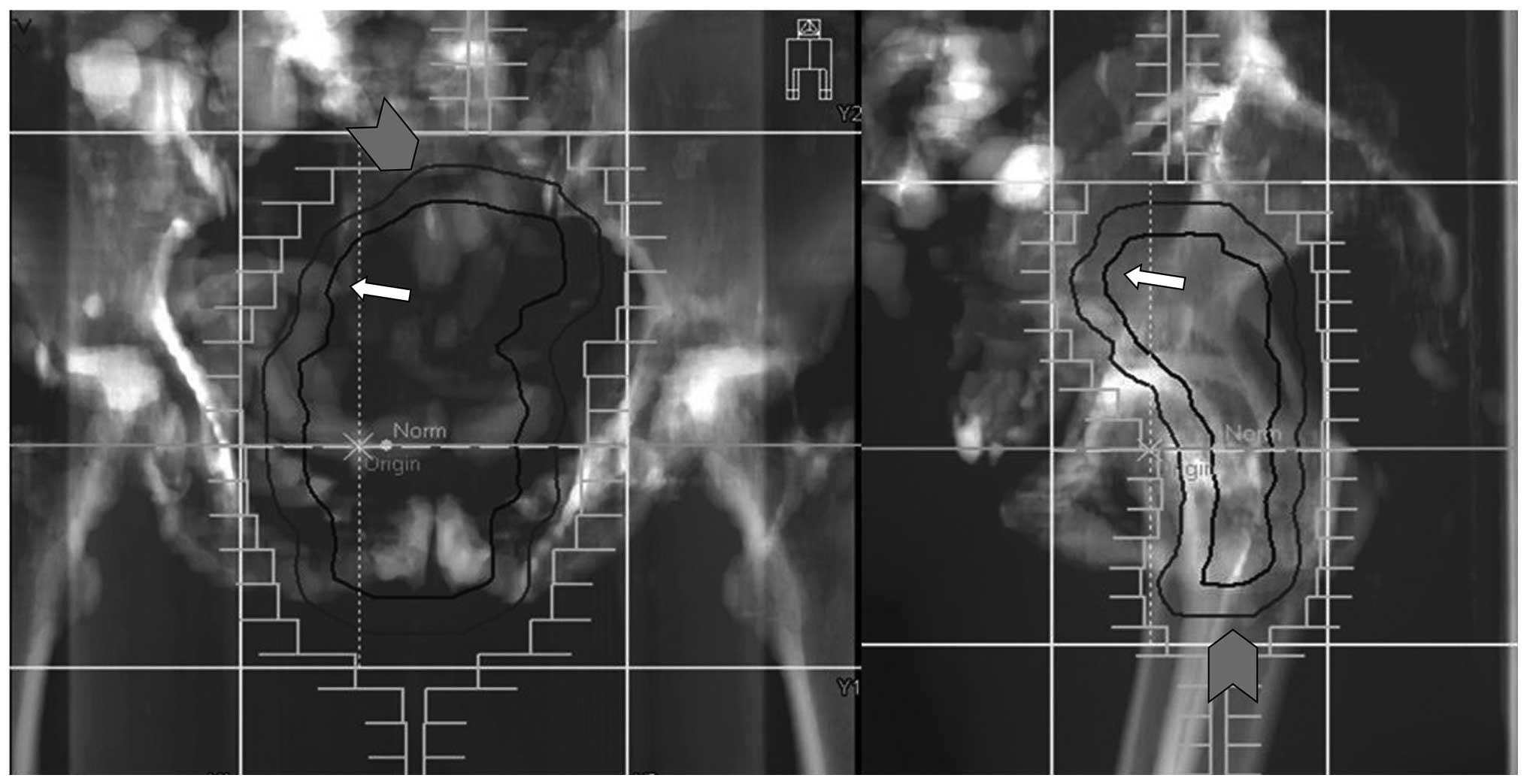
RT was delivered by 10 to 15-MV photon beams to a
planning target volume (PTV) defined as the clinical target volume
(CTV) plus a 1-cm isotropic margin (Fig.
1). CTV was defined as the uterus and disease-involved tissues
in the pelvis plus a 1-cm margin. The PTV prescribed RT dose was a
total of 30 Gy in 3 Gy/fraction, and was administered by a
three-dimensional four-fields box technique in 10 fractions over 2
weeks. The target margin and dose were chosen due to their common
use for diverse palliative clinical scenarios. The dose was
specified according to the International Commission on Radiation
Units and Measurements Report 62 (21). All plans were generated with the
Masterplan Oncentra treatment planning system (TPS v.4.1; Nucletron
BV; Elekta, Veenendaal, Netherlands) and delivered by an Elekta
Precise linear accelerator (Elekta Ltd., Crawley, UK). Fields were
shaped using the beam's eye view projections of the PTV by means of
a standard multileaf collimator (2×40 leaves; width, 1 cm at the
isocenter distance). In all patients, daily portal images were
acquired prior to treatment on two orthogonal beams to ensure the
correct patient set-up; any deviation >5 mm in the isocenter
position was promptly corrected.
Follow-up evaluation
Subsequent to the completion of the treatment,
patients underwent the first follow-up at 30 days, and thereafter
at 3-month intervals. Follow-up visits included a physical
examination and complete laboratory tests. Acute and late radiation
toxicities were scored according to the Radiation Therapy Oncology
Group and European Organization for the Research and Treatment of
Cancer toxicity scales, respectively (22). Resolution of bleeding was considered
as a complete palliative response, while reduction of bleeding was
considered as a partial response.
Statistical analysis
Descriptive statistics were performed. The actuarial
bleeding-free survival was calculated from the date of LNG-IUD/RT
treatment to the date of bleeding relapse or the date of last
follow-up, and was analyzed using the Kaplan-Meier method (23). Overall survival (OS) was calculated on
a per patient basis from the date of diagnosis to the date of
mortality or the date of the last follow-up. Statistical analyses
were carried out using Systat v.10.2 (2002, for Windows; Systat
Software Inc., San Jose, CA, USA).
Results
Patient characteristics
Between May 2009 and April 2014, 9 patients meeting
the inclusion criteria were enrolled in the present prospective
study, and received an LNG-IUD plus RT. The clinical and
pathological characteristics of the patients are summarized in
Table I. The median age was 85 years
(range, 65–92 years), and the vast majority of patients (n=8;
88.8%) had an ECOG performance status of ≥2. Patients were
considered as overweight or obese in 4 and 5 cases, respectively;
the median Charlson comorbidity index was 5 (range, 4–11), with 2
patients presenting with ≤3 comorbidities and 7 patients with ≥4
comorbidities. Hypertension (88.8%), cardiac disease (66.6%) and
obesity (55.5%) were the most frequently documented
comorbidities.
 | Table I.Clinical and pathological
characteristics |
Table I.
Clinical and pathological
characteristics
| Characteristics | Value |
|---|
| Total patients, n
(%) | 9 (100.0) |
| Median age (range),
years | 85 (65–92) |
| ECOG, n (%) |
|
| 1 | 1 (11.1) |
| 2 | 5 (55.6) |
| 3 | 3 (33.3) |
| Median BMI
(range) | 36.4 (24–55) |
| Median CCI
(range) | 5 (4–11) |
| Comorbidities, n
(%) |
|
|
Hypertension | 8 (88.9) |
| Cardiac
disease | 6 (66.7) |
| Obesity,
BMI ≥30.0 | 5 (55.6) |
|
Anemia | 4 (44.4) |
|
Diabetes | 4 (44.4) |
| Thyroid
disorders | 4 (44.4) |
| Chronic
obstructive pulmonary disease | 3 (33.3) |
| Previous
solid neoplasm | 3 (33.3) |
| Lower
limb venous insufficiency | 2 (22.2) |
| Previous
ictus cerebri | 2 (22.2) |
| HCV
positivity | 1 (11.1) |
| Lower
limb paresis | 1 (11.1) |
| Irritable
bowel syndrome | 1 (11.1) |
| Histology, n (%) |
|
|
Endometrial carcinoma, G1 | 3 (33.3) |
| Müllerian
adenosarcoma, G1 | 1 (11.1) |
|
Endometrial carcinoma, G2 | 4 (44.4) |
|
Endometrial carcinoma, G3 | 1 (11.1) |
| Clinical stage, n
(%) |
|
| I | 6 (66.7) |
| II | 1 (11.1) |
| IVB
(liver, lung) | 2 (22.2) |
| Median CA-125 at
diagnosis (range), IU/ml | 31.4 (9–226) |
The primary tumor was represented by endometrial
adenocarcinoma in 8 out of the 9 cases, and all but one was
well/moderately-differentiated. The majority of cases (77.7%)
exhibited stage I–II disease, according to the 2009 FIGO staging
system (24), and the CA-125 level
ranged between 9–226 international units (IU)/ml, with a median
value of 31.4 IU/ml (normal range, 0–35 IU/ml).
Efficacy
Details on the efficacy of the treatment are
provided in Table II: The complete
resolution of bleeding was documented in 8 patients (88.8%), while
the remaining patient experienced a marked improvement.
| Table II.Treatment details, response and
toxicity. |
Table II.
Treatment details, response and
toxicity.
|
|
|
|
|
| Acute toxicity |
|---|
|
|
|
|
|
|
|
|---|
| Patient no. | RT dose/fraction,
Gy | Bleeding
control | Bleeding control
duration, months | Bleeding
relapse | District | Grade | Type |
|---|
| 1 | 30/3 | Complete | 51 | Yes | GI | 1 | Diarrhea,
tenesmus |
| 2 | 30/3 | Complete | 22 | Yes | Skin | 1 | Erythema |
| 3 | 30/3 | Complete | 43 | No | GI | 2 | Diarrhea |
| 4 | 30/3 | Complete | 35 | No | GU | 1 | Dysuria |
| 5 | 30/3 | Partial | 2 | Yes | GI | 1 | Increased frequency
of bowel habits and tenesmus |
| 6 | 30/3 | Complete | 13 | No | – | – |
|
| 7 | 30/3 | Complete | 18 | Yes | Skin | 1 | Faint erythema |
| 8 | 30/3 | Complete | 15 | No | Skin | 2 | Moderate to brisk
erythema and moderate edema |
|
|
|
|
|
| GI | 2 | Diarrhea,
tenesmus |
| 9 | 30/3 | Complete | 2 | No | Skin | 1 | Faint erythema |
|
|
|
|
|
| GI | 2 | Diarrhea,
tenesmus |
All patients experienced an early onset of benefit
(within 10 days from the start of RT); the median duration of
palliation was 18 months (range, 2–51 months). The relapse of
bleeding was observed in 4 patients (at 51, 22, 18 and 2 months
after RT, respectively). Re-irradiation was proposed to all
patients who experienced a relapse of bleeding, with the exception
of 1 patient who did not undergo re-irradiation due to a sudden and
irreversible deterioration of renal function. In 3 of the patient,
short-course re-treatment was successfully performed at doses of
12–14 Gy, in twice daily fractions over 2 days; the complete (n=1)
and partial (n=2) remission of symptoms, still persisting at the
time of this report, were documented.
With a median follow-up time of 20 months (range,
9–60 months), the 2-year actuarial rate of bleeding-free survival
was 53.3%. Data on the objective response rate assessed by Response
Evaluation Criteria in Solid Tumors (25) were collected, although this was not
included in the study endpoints: a partial response was registered
in 7 patients, while 2 patients exhibited stable disease (data not
shown).
Overall, disease-associated mortality was documented
in 3 patients and the 2-year overall survival rate was 75%.
Safety
Table II also
presents the acute and late toxicity results; no LNG-IUD-related
complications were documented. The most common RT-related toxicity
was of the lower gastrointestinal tract (55.5%), and involved 3
patients presenting with grade 2 diarrhea and tenesmus, and 2
patients with grade 1 increased frequency of bowel habits and
tenesmus. Skin erythema was reported in 4 patients (grade 1 in 3
patients and grade 2 in 1 patient), while grade 1 dysuria was
observed in 1 patient. Overall, no patient developed grade 3 acute
toxicity.
As far as late toxicity is concerned, 2 patients (1
with chronic obstructive pulmonary disease and 1 with lung
metastasis) developed a pulmonary embolism that was successfully
managed by medical intervention. Finally, a 92-year-old patient
developed proctitis 12 months after the completion of RT, and
presented with intermittent rectal bleeding that was managed with
topical steroids. There was no case of treatment discontinuation
due to major complications/adverse effects.
Discussion
To the best of our knowledge, this series represents
the first report on the activity and toxicity of LNG-IUD insertion
plus short-course RT in frail, elderly uterine cancer patients with
severe comorbidities who were judged to be unsuitable for curative
treatments.
The choice of combining LNG-IUD insertion plus
short-course RT sounded attractive given the well recognized
efficacy of RT schedules in palliative care, and the strong
rationale sustaining the use of LNG-IUD insertion, which is endowed
with a low toxicity rate and marked activity in uterine
hyperplastic/neoplastic lesions (16).
With the limits inherent in the evaluation of this
case series, complete resolution of bleeding was recorded in 88.8%
of cases; this data was well matched with the corresponding data
reported in the palliative setting of gynecological and
non-gynecological malignancies (4,9), while
providing favorable results in terms of type and severity of side
effects. This is particularly important in a clinical setting, in
which the main purpose of treatment is to preserve quality of life.
The documentation of 2 cases of pulmonary embolism occurring in the
long-term evaluation, which were successfully managed with medical
intervention, is hardly imputable to the LNG-intrauterine system,
considering that the 2 patients had medical histories of
respiratory failure, obesity and a CCI value of 5.
Moreover, despite the frailty of the present study
population, a prolonged median duration of bleeding control of 18
months was reported, a value which appears quite encouraging when
compared with the mean symptom-free duration (5 months) of
palliative radiation only (6,26).
Whether this finding could be ascribed to the
addition of LNG-IUD insertion to palliative RT is difficult to
ascertain, considering the heterogeneity and size of previously
reported studies, as well as the present sample. However, the
efficacy of progestin administration in fertility-sparing, as well
as in advanced/recurrent clinical settings, has been widely
established over time (10–15), and long-lasting responses, regardless
of type and dosage of progestin, have been reported in different
clinical settings (13–15,17,18,27).
Therefore, the possibility that progestin administration could have
contributed to the long-term duration of symptom remission induced
by palliative RT cannot be excluded in the present series.
One could question the lack of a requirement of
estrogen (ER) and progesterone receptor (PR) tumor expression
assessment within the inclusion criteria of the present study:
however, it is well known that despite the presence of ER and PR in
the vast majority of well-differentiated endometrial tumors, not
all grade 1 EC patients respond to progestin (27). On the other hand, patients bearing
grade 2 and grade 3 endometrial carcinomas, which express ER and PR
in a lower percentage of cases (28,29), have
been shown to exhibit a not negligible response to progestin in
different clinical settings (30–34).
These considerations, which highlight the
requirement to provide a more in-depth elucidation of molecular
mechanisms sustaining progestin activity beside and beyond those
driven by ER and PR, led us to propose the use of LNG-IUD insertion
in patients triaged to palliative treatment, regardless of steroid
hormone receptor expression.
In conclusion, the present study reports the first
case series of frail, elderly uterine tumor patients triaged to
palliative RT plus LNG-IUD insertion. A high rate of bleeding
remission, durable bleeding-free survival in the face of the easy
intrauterine insertion of an LNG-IUD, a lack of immediate or late
complications, and a negligible toxicity profile for the overall
treatment were documented. While the contribution of LNG-IUD
insertion to RT efficacy is difficult to ascertain, the encouraging
activity of this combination deserves further investigation in a
larger series.
References
|
1
|
Fishman DA, Roberts KB, Chambers JT,
Kohorn EI, Schwartz PE and Chambers SK: Radiation therapy as
exclusive treatment for medically inoperable patients with stage I
and II endometrioid carcinoma with endometrium. Gynecol Oncol.
61:189–196. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Coon D, Beriwal S, Heron DE, Kelley JL,
Edwards RP, Sukumvanich P, Zorn KK and Krivak TC: High-dose-rate
Rotte ‘Y’ applicator brachytherapy for definitive treatment of
medically inoperable endometrial cancer: 10-year results. Int J
Radiat Oncol Biol Phys. 71:779–783. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Niazi TM, Souhami L, Portelance L, Bahoric
B, Gilbert L and Stanimir G: Long-term results of high-dose-rate
brachytherapy in the primary treatment of medically inoperable
stage I–II endometrial carcinoma. Int J Radiat Oncol Biol Phys.
63:1108–1113. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lutz ST, Chow EL, Hartsell WF and Konski
AA: A review of hypofractionated palliative radiotherapy. Cancer.
109:1462–1470. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gill BS, Chapman BV, Hansen KJ,
Sukumvanich P and Beriwal S: Primary radiotherapy for nonsurgically
managed Stage I endometrial cancer: Utilization and impact of
brachytherapy. Brachytherapy. 14:373–379. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Caravatta L, Padula GD, Macchia G,
Ferrandina G, Bonomo P, Deodato F, Massaccesi M, Mignogna S,
Tambaro R, Rossi M, et al: Short-course accelerated radiotherapy in
palliative treatment of advanced pelvic malignancies: A phase I
study. Int J Radiat Oncol Biol Phys. 83:e627–e631. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim DH, Lee JH, Ki YK, Nam JH, Kim WT,
Jeon HS, Park D and Kim DW: Short-course palliative radiotherapy
for uterine cervical cancer. Radiat Oncol J. 31:216–21. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Spanos WJ Jr, Perez CA, Marcus S, Poulter
CA, Doggett RL, Steinfeld AD and Grigsby PW: Effect of rest
interval on tumor and normal tissue response-a report of phase III
study of accelerated split course palliative radiation for advanced
pelvic malignancies (RTOG-8502). Int J Radiat Oncol Biol Phys.
25:399–403. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yan J, Milosevic M, Fyles A, Manchul L,
Kelly V and Levin W: A hypofractionated radiotherapy regimen
(0-7-21) for advanced gynaecological cancer patients. Clin Oncol (R
Coll Radiol). 23:476–481. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lai CH and Huang HJ: The role of hormones
for the treatment of endometrial hyperplasia and endometrial
cancer. Curr Opin Obstet Gynecol. 18:29–34. 2006.PubMed/NCBI
|
|
11
|
Leslie KK, Thiel KW and Yang S:
Endometrial cancer: Potential treatment and prevention with
progestin-containing intrauterine devices. Obstet Gynecol.
119:419–420. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mountzios G, Pectasides D, Bournakis E,
Pectasides E, Bozas G, Dimopoulos MA and Papadimitriou CA:
Developments in the systemic treatment of endometrial cancer. Crit
Rev Oncol Hematol. 79:278–292. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dhar KK, NeedhiRajan T, Koslowski M and
Woolas RP: Is levonorgestrel intrauterine system effective for
treatment of early endometrial cancer? Report of four cases and
review of the literature. Gynecol Oncol. 97:924–927. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Giannopoulos T, Butler-Manuel S and Tailor
A: Levonorgestrel-releasing intrauterine system (LNG-IUS) as a
therapy for endometrial carcinoma. Gynecol Oncol. 95:762–764. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Montz FJ, Bristow RE, Bovicelli A,
Tomacruz R and Kurman RJ: Intrauterine progesterone treatment of
early endometrial cancer. Am J Obstet Gynecol. 186:651–657. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Toivonen J and Luukkainen T:
Progestin-releasing intrauterine devices. Curr Ther Endocrinol
Metab. 6:281–285. 1997.PubMed/NCBI
|
|
17
|
Gallos ID, Shehmar M, Thangaratinam S,
Papapostolou TK, Coomarasamy A and Gupta JK: Oral progestogens vs.
levonorgestrel-releasing intrauterine system for endometrial
hyperplasia: A systematic review and meta-analysis. Am J Obstet
Gynecol. 203(547): e1–e10. 2010.PubMed/NCBI
|
|
18
|
Gallos ID, Krishan P, Shehmar M, Ganesan R
and Gupta JK: LNG-IUS versus oral progestogen treatment for
endometrial hyperplasia: A long-term comparative cohort study. Hum
Reprod. 28:2966–2971. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Guttinger A and Critchley H: Endometrial
effects of intrauterine levonorgestrel. Contraception. 75(6 Suppl):
S93–S98. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Luukkainen T, Lähteenmäki P and Toivonen
J: Levonorgestrel-releasing intrauterine device. Ann Med. 22:85–90.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
André Wambersie and Torsten Landberg: ICRU
report 62: Prescribing, recording and reporting photon beam therapy
(Supplement to ICRU Report 50). ICRU. Bethesda, MD: 1999.
|
|
22
|
Cox JD, Stetz J and Pajak TF: Toxicity
criteria of the Radiation Therapy Oncology Group (RTOG) and the
European Organization for Research and Treatment of Cancer (EORTC).
Int J Radiat Oncol Biol Phys. 31:1341–1346. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kaplan EL and Meier P: Non-parametric
estimation from incomplete observations. J Am Statist Assoc.
53:457–481. 1958. View Article : Google Scholar
|
|
24
|
Creasman W: Revised FIGO staging for
carcinoma of the endometrium. Int J Gynaecol Obstet. 105:1092009.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT, Christian MC and Gwyther SG: New guidelines to
evaluate the response to treatment in solid tumors. European
organization for research and treatment of cancer, national cancer
institute of the united states, national cancer institute of
canada. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mishra SK, Laskar S, Muckaden MA, Mohindra
P, Shrivastava SK and Dinshaw KA: Monthly palliative pelvic
radiotherapy in advanced carcinoma of uterine cervix. J Cancer Res
Ther. 1:208–212. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ramirez PT, Frumovitz M, Bodurka DC, Sun
CC and Levenback C: Hormonal therapy for the management of grade 1
endometrial adenocarcinoma: A literature review. Gynecol Oncol.
95:133–138. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Carcangiu ML, Chambers JT, Voynick IM,
Pirro M and Schwartz PE: Immunohistochemical evaluation of estrogen
and progesterone receptor content in 183 patients with endometrial
carcinoma. Part I: Clinical and histologic correlations. Am J Clin
Pathol. 94:247–254. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mhawech-Fauceglia P, Yan L, Liu S and
Pejovic T:
ER+/PR+/TFF3+/IMP3−
immunoprofile distinguishes endometrioid from serous and clear cell
carcinomas of the endometrium: A study of 401 cases.
Histopathology. 62:976–985. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bokhman JV, Chepick OF, Volkova AT and
Vishnevsky AS: Can primary endometrial carcinoma stage I be cured
without surgery and radiation therapy? Gynecol Oncol. 20:139–155.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gotlieb WH, Beiner ME, Shalmon B, Korach
Y, Segal Y, Zmira N, Koupolovic J and Ben-Baruch G: Outcome of
fertility-sparing treatment with progestins in young patients with
endometrial cancer. Obstet Gynecol. 102:718–725. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hahn HS, Yoon SG, Hong JS, Hong SR, Park
SJ, Lim JY, Kwon YS, Lee IH, Lim KT, Lee KH, et al: Conservative
treatment with progestin and pregnancy outcomes in endometrial
cancer. Int J Gynecol Cancer. 19:1068–1073. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kaku T, Yoshikawa H, Tsuda H, Sakamoto A,
Fukunaga M, Kuwabara Y, Hataeg M, Kodama S, Kuzuya K, Sato S, et
al: Conservative therapy for adenocarcinoma and atypical
endometrial hyperplasia of the endometrium in young women: Central
pathologic review and treatment outcome. Cancer Lett. 167:39–48.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Koskas M, Yazbeck C, Walker F, Clouqueur
E, Agostini A, Ruat S, Lucot JP, Lambaudie E, Luton D and Madelenat
P: Fertility-sparing management of grade 2 and 3 endometrial
adenocarcinomas. Anticancer Res. 31:3047–3049. 2011.PubMed/NCBI
|